You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Many of today’s medical testing and therapies rely heavily on the use of hypodermic needles. In dentistry, the needle is most commonly used for local anesthetic administration. Much of the general population closely associates the use of a needle with a visit to the dental office. Unfortunately, this association usually carries a negative connotation presented as pain, anxiety, and dissatisfaction.1 Different injection techniques and patient management methodologies have been proposed to decrease the fear patients may have concerning dental care. Regardless of these practices, the majority of patients still have a dislike of the injection and associate dentistry with the needle.2,3 Patients tend to think about the needle first when considering dental care.4 Because of its influential standing in the patient’s perspective of dental lore, dental providers would benefit from having an understanding of the technological advances, changes in techniques, and patient perceptions associated with the needle.
Practice Characteristics
Needle usage in dental practice has changed as improvements have been made in efficiency and safety. In the first half of the twentieth century, needles were reusable and required sharpening while occasionally being properly sterilized. In the 1960s, the disposable stainless-steel needle was introduced resulting in a collective acceptance by the dental profession. An evaluation of disposable needle purchases from Henry Schein® Dental and Septodont, Inc. in the United States revealed that 30-gauge needles were purchased most often (Schein: 56% / Septodont: 59%), followed by 27-gauge needles (Schein: 42% / Septodont: 38%) and 25-gauge needles (Schein: 1% / Septodont: 3%).5 According to cumulative data from both companies, the short needle was purchased more often (62.1%) than the long (30.5%) or extra short (7.5%) needles.5 Anecdotal evidence reveals that the most commonly purchased brands include: Monoject® (metal and plastic hub) (Kendall, www.kendallhealthcare.com); Septoject®, Septoject® XL, and Septoject® Evolution (Septodont, Inc., www.septodontusa.com); Accuject® (DENTSPLY, www.dentsply.com); J. Morita disposable dental needles (www.morita.com); Painless Steel® dental injection needles (www.painless-steel.com); and various private label brands (eg, Henry Schein [www.henryschein.com], Patterson Dental [www.pattersondental.com], etc.). Exact marketing data on total sales of each brand is not readily available for publication at this time.
Pain Perception and the Dental Injection
In order to appreciate the value of a quality needle, it is important to understand the pain perception process associated with the dental injection. The perception of pain usually occurs as a result of noxious stimuli. This body process relates to a desire for survival. Pain response is a means by which the body can communicate tissue damage or the possibility of damage to the brain in the hope of avoiding or eliminating danger. Noxious stimuli during the anesthetic injection, which can produce tissue damage, are detected by the terminal endings of two major classes of nociceptive (pain-detecting) afferent nerve fibers. (Considering this section as a review, the authors are presenting a broad nerve fiber classification instead of the many subgroups.) The two main sensory nerve fibers associated with injection pain are Type A and Type C.
The Type A fibers are relatively fast-conducting, lightly myelinated fibers that respond to mechanical pain as opposed to chemical or thermal stimulation.6,7 These fibers are proposed to arbitrate the preliminary sensation of pain, which has a sharp or vivid perceptual quality. The Type C fibers are slow-conducting, un-myelinated nerve fibers that react more to thermal and chemical stimulation. They are likely to mediate the pain response that occurs after the preliminary pain reaction has occurred, usually described as a dull, aching, or burning sensation.6
When considering a dental injection, the process of pain perception is best described using a chronological review (Table 1). As the needle penetrates the mucosa the Type A fibers communicate to the brain, the initial, sharp type of pain stimulation. Most dental providers use topical anesthetic to obtund the brightness of this pain response. However, the bevel, located at the point of the needle, is just as important in decreasing Type A pain reaction.8
Once the needle is located at the area of injection, the anesthetic solution is deposited to block the sensation of pain by hindering the propagation of nerve impulses. The deposition of solution into the tissue can be associated with a pain response, often described as a burning or aching pain. This pain response involves both Type A, due to expansion of tissue, and Type C nerve fibers, due to the chemical complexion and pH of the local anesthetic. Patients usually report this portion of the injection to be most painful. Controlling the speed of solution deposition, computer-controlled delivery, and the use of buffering agents have all been recommended to decrease the pain response of fluid deposition.9-11 As it relates to the needle, the bore design can play a key role in decreasing the pressure of solution flowing out of the device into the tissue.
Lastly, both types of sensory nerve fibers can illicit response during the removal of the needle and/or postoperatively when the anesthetic effect has ceased. Postoperative pain has been associated with the pH of the anesthetic solution, administration of multiple injections, or poor injection technique.12-14 In addition, damage to the tissue and a continued pain response can occur from needle barbing, peeling, or splintering. The overall structural integrity and design of the needle, as well as the type of protective coating, are important aspects to preventing post-deposition or post-injection pain.
Needle Properties
Considerable variation exists regarding how a needle is selected for patient care. Just as there is variation in needle selection, there are differences in how manufacturers design and structure their needles. Given the goal to administer care with little or no pain, dental providers should obtain an understanding of the components of needle design that allow for comfortable anesthetic delivery.
Needle Gauge
The diameter of the needle is referred to as the gauge. The needles most readily available for dentistry are the 25-, 27-, and 30- gauge (the higher the gauge, the smaller the diameter of the needle). In the last few decades, there has been a noticeable shift to the use of smaller diameter needles, based on speculation that the smaller the needle, the less amount of pain felt.5 However, this conjecture is most likely unwarranted based on available empirical evidence. A published review article from the early 1990s investigated the probability of needle gauge relating to pain response with intraoral anesthetic injections.15 Citing additional publications, the authors concluded that reports of pain response was not related to needle gauge.16-18 In a recent study, Flanagan et al completed 930 intraoral injections using 25-, 27-, and 30-gauge needles during standard maxillary and mandibular injection techniques.19 At the completion of the study, the investigators concluded that there was no statistically significant difference in pain perception among subjects analyzed. As opposed to needle gauge, several researchers advocate that the sharpness and structure of the bevel plays a more significant role in decreasing the pain response.11,15
Bevel
The bevel is considered the “sloping tip” of the needle. As depicted in Figure 1, there are five main types of bevels: short, medium, long, multi, and scalpel. The role of the bevel is to provide a cutting surface that offers little resistance to mucosa as the needle penetrates and withdraws from the tissue. As resistance to tissue decreases, patient comfort has been reported to improve.20,21
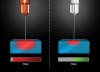
While several tip configurations are available to dental practitioners, the multi-beveled point is traditionally considered to produce the most effective puncture while eliciting the least amount of trauma.9 It should be noted that the advent of the new scalpel bevel for maxillary and periodontal ligament injections (this needle type is not recommended for any injection procedures in which a nerve may be directly contacted) may offer an advanced alternative. The scalpel bevel design (eg, Septoject Evolution) offers the nuance of having a surgical scalpel-like point. The scalpel design has been reported to allow for needle insertion with less tissue displacement, thus requiring less force to penetrate the mucosa (Figure 2).22
One prominent opinion within dentistry is that the bevel has been placed to aid the direction of the fluid deposition; therefore, the bevel should be oriented toward the area to be anesthetized. Actually, the aspect of bevel orientation during injection is rooted in needle deflection or displacement.23 Because of the bevel design, the needle tip is asymmetric and it creates an off-balance aspect to the needle. It has been proposed that because the tip is located off the central axis, the needle will deflect away from the bevel.9,14 Several publications have reported that the larger the angle of the bevel with the long axis of the needle, the greater will be the degree of deflection through tissue.14,20 The ideal needle design will allow for a centralized or balanced management of tissue force onto the needle tip. With an effectively engineered needle, the force of the tissue will translate directly down the center of the shaft, similar to driving a wedge or axe while splitting wood. These types of needles are at times referred to as “non-deflecting” needles. Available research indicates significantly less deflection with this design compared to a variety of conventional needles where orientation (toward or away from a target area) does not affect anesthesia success.21,23
Bore or Lumen
The hollow portion, or tube, of the needle is referred to as the lumen or bore. The correlation between bore design and patient comfort relates to injection pressure. Injection pressure was found to directly influence the intensity of perceived pain at the start of a dental injection as well as influence the anxiety level of patients.24 In addition, Pashley et al revealed that the pressure generated during dental local anesthesia administration had high values, ranging from 17,061 to 34,122 mm Hg (325 to 675 PSI).25
Injection pressure is created when the plunger of the anesthetic cartridge is depressed creating a flow of solution into the tissue. When this process occurs, a narrow bore produces jet under pressure causing tissue injury and pain.26 On the other hand, larger bore needles have been found to reduce pain and edema after injection due to a lower pressure requirement to depress the plunger.27
Length
The injection technique and operator inclination will determine what length of needle is used. Currently, there are three lengths available to the dental provider: long (1.10 to 1.65 inch); short (0.75 to 1.00 inch); and ultra-short (0.4 to 0.5 inch). The length of the needle has not directly been associated with an increase in pain response, although needle length can play a part in occasional pain as long needles are more likely used with injections that can contact bone.
Coating
Coating of the hypodermic needle with silicon dates back to the late 1960s when it was proposed as a method to improve coefficient of friction. The coefficient of friction is the ratio of the force that maintains contact with an object and the force that resists motion of the object (eg, the tissue’s force upon the progression and withdrawal of the needle). Originally, the idea of coating the needle was rooted in having a smoother transition through the tissue to target area. It should also be noted that some studies imply that by decreasing the frictional action of the tissues with coating, the quality of the needle tip can be maintained for a longer period of time.28,29
Complications and Adverse Occurrences
The administration of local anesthetics in dentistry has a remarkable record of safety. Severe adverse outcomes related to dental local anesthesia are extremely rare, and studies evaluating administration demonstrate a low risk of complication.30 Although complications are an uncommon occurrence, dental providers should understand how they may occur, as well as appropriate treatment protocols, and, most importantly, how to prevent complications from happening. The following represents an abbreviated review of reported complications that can directly involve the hypodermic needle in dentistry.
Needle Breakage
A Medline review performed by Malamed et al revealed the availability of 26 case reports relating to needle breakage and management.5 Analysis of these reports demonstrates that the majority involves the inferior alveolar nerve block injection (IANB) and, to a lesser degree, the posterior superior alveolar nerve block (PSA) injection. An additional report by Pogrel of 16 occurrences of needle breakage stated that 15 reports involved the IANB injection and 1 occurred during a PSA injection.31 Additionally, it was found that the majority (81.3%) of the needle breakage occurrences involved 30-gauge short needles. Commonalities reported with needle breakage include: the use of 30-gauge needles; inserting the needle flush with the mucosa; the use of an IANB or PSA injection with short needles; and needle fracture at the hub. It should be noted that in cases of post-breakage needle evaluation, no evidence of manufacturing defects have been proposed.5
Recommendations to prevent needle breakage include: avoiding short needles for IANB injections; not inserting the needle where the hub is flush with oral mucosa; not bending needles; and not using 30-gauge needles for injection types that require a deeper target area. If needle breakage does occur and a portion of the needle remains visible, the practitioner can use hemostats or cotton pliers to carefully grab and gently remove the needle. Following removal, radiographic evaluation of the area is recommended to ensure that no remnants are still in tissue. If the needle is completely engulfed in tissue upon breakage, the dental provider should: inform the patient and reassure to keep him or her calm; take a standard panoramic radiograph and, if possible, additional radiographs in both lateral and frontal planes (computed tomographic [CT] scanning is ideal if available); save the remaining syringe, including the needle hub, for structural evaluation after the needle fragment has been removed from the tissue; and refer the patient immediately to an oral surgeon, plastic surgeon, or operating provider to remove the retained fragment.
Needle Barbing
Barbing of the needle is considered to occur when the point, or tip, of the needle becomes bent, usually at microscopic levels. Barbing can occur during syringe preparation, advancement of the needle through tissue, with multiple injections, or when contacting bone during injection. Needle barbs can be dangerous as they can tear tissues, including nerve fibers, upon removal or with subsequent re-insertion. Overall, reports of barbing incidence are demonstrated between 30% and 78% of the time, with a higher occurrence for injections in which bone is contacted.32-34
Barbing can rarely be seen with the naked human eye. However, a practitioner can check for barbing by drawing the needle across a piece of gauze, which will result in threads of the gauze being grabbed by the barb.9,14 It has been recommended that a needle should not be inserted into tissue more than three to four times to avoid barbing or dulling.14 Additionally, some practitioners will replace the needle when changing the cartridge or use more than one syringe set-up to deliver anesthetic during multiple injection appointments. Ultimately, the use of a new needle at each injection will provide a higher level of confidence in sharpness, decrease the chance of barbing, and limit possible contamination with a gauze test.
A needle with manufacturing defects is more likely to have existing, or easily created, barbing and splintering, which may result in issues with the penetration process of the needle, damage to soft and neuronal tissues, hemorrhage, or causing moderate to severe pain.34 During the manufacturing process, the cutting of the needle bevel can lead to irregularities in the stainless steel, which may result in these adverse outcomes (Figure 3). The creation of the irregularities is related to both the cutting process and the quality of steel being used.35
ISO (International Organization for Standardization) provides standards on the type of stainless steel as well as the minimum thickness of steel used in needle manufacturing. Because of organizations like ISO, manufacturing defects continue to decrease. However, defects still exist, especially on a microscopic level.35 In fact, a recent study evaluating the most commonly purchased needles found that the homogeneity in the metal alloys did not generally conform to international manufacturing guidelines.36 In addition, the authors concluded that a wide variation between applied standards exist and it appears that most manufacturers apply their own standards to the manufacturing process. Ultimately, the quality of material and the type of finish of the needle bevel is vital in decreasing the irregularities, which aids in decreasing barbing.34,35
Selecting a Quality Needle
The selection of a needle is usually based on the practice of an individual provider and his or her perceptions of their patient population. Currently, there is no universal acceptance of what needle is the best for dentists to use. However, a review of available research does provide ideal needle characteristics such as: a multi-beveled/scapel-beveled point9,22; a bevel design that is centralized with the long axis of the needle (non-deflecting)5,14; larger bore needles24-27; silicon coating28,29; the appropriate metal alloy used in manufacturing34-36; and appropriate metal finishing.35 Ultimately, the design should aid the practitioner in providing the most effective and safe anesthetic administration while causing the least amount of pain as possible.
Overall, the availability of comparative needle studies is limited. The majority of research evaluates specific characteristics and rarely includes a multiple sample of marketed brands. However, some accord can be ascertained by evaluating the few existing studies available. A recent microscopic assessment of unused needles evaluated seven different brands to verify the quality of the bevel zone of each needle.35 The authors concluded that the needles with a good finish are SOPIRA® Carpule® (Heraeus Kulzer, www.heraeus-kulzer.com) and Terumo® dental needles (Terumo Medical Corp., www.terumotmp.com), while the aforementioned Septoject needle offered the best overall quality. In an analysis published in 2006, needles of various lengths and gauges from seven different manufacturers were subjected to tensile tests for breakage force evaluation.37 The investigators found that the needles manufactured by different companies all have different properties and that length and gauge do not directly affect performance during tensile testing. Given the comparison of data and the variation in properties of each needle evaluated, statistically significant differences were difficult to ascertain between manufacturers. Albergo et al noted that the Carpule Free Flow needle (Heraeus Kulzer) showed better clinical characteristics than the standard Carpule needle.38 Almendros Marqués et al did not find any differences in bevel deformation between the Monoprotect® (Sofic, www.sofic.com) / Septoject standard needles and the larger bore Monoprotect® XL / Septoject XL needles.34 Given that significant differences exist between different manufacturers’ needles, further research is needed that compare the quality, efficacy, and safety, of dental hypodermic needles.
Conclusion
Alleviating patients’ concerns regarding the dental needle is an important aspect of providing quality, reassuring dental care. There are notable variations between different brands and types of needles. Dental providers should be knowledgeable about the most advantageous needle characteristics and types of needles available for their patients. Ultimately, a quality dental hypodermic needle can improve the patient experience.
DISCLOSURE
The author has served as a consultant to Septodont, Inc. regarding development of new agents/devices for dentistry, and as an investigator for FDA-required clinical research contracts awarded by Septodont. In addition, he has presented continuing education courses partially sponsored by Henry Schein Dental and Septodont.
ABOUT THE AUTHOR
Sean G. Boynes, DMD
Director of Dental Medicine, CareSouth Carolina, Society Hill, SC
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
REFERENCES
1. Hamilton JG. Needle phobia: a neglected diagnosis. J Fam Pract. 1995;41(2):169-175.
2. Milgrom P, Weinstein P, Getz, T. Treating Fearful Dental Patients: A Patient Management Handbook. 2nd ed. Seattle, WA: University of Washington Continuing Dental Education; 1995.
3. Matthews DC, Rocchi A, Gafni A. Factors affecting patients’ and potential patients’ choices among anesthetics for periodontal recall visits. J Dent. 2001;29(3):173-179.
4. de St Georges J. How dentists are judged by patients. Dent Today. 2004 23(8):98-99.
5. Malamed SF, Reed K, Poorsattar S. Needle breakage: incidence and prevention. Dent Clin North Am. 2010;54(4):745-756.
6. Dionne RA, Phero J, Becker DG. Management of Pain and Anxiety in the Dental Office. Philadelphia, PA: WB Saunders; 2002.
7. Iggo A, ed. Handbook of Sensory Physiology. Volume II. Somatosensory System. Berlin, Germany: Springer-Verlag; 1973.
8. Vedrine L, Prais W, Laurent PE, et al. Improving needle-point sharpness in pre-fillable syringes. Med Device Technol. 2003;14(4):32-35.
9. Jastak JT, Yagiela JA, Donaldson D. Local Anesthesia for the Oral Cavity. Philadelphia, PA: WB Saunders; 1995.
10. Hanna MN, Elhassan A, Veloso PM, et al. Efficacy of bicarbonate in decreasing pain on intradermal injection of local anesthetics: a meta-analysis. Reg Anesth Pain Med. 2009;34(2):122-125.
11. Davies RJ. Buffering the pain of local anesthetics: a systematic review. Emerg Med (Fremantle). 2003;15(1):81-88.
12. Kaufman E, Epstein JB, Naveh E. A survey of pain, pressure, and discomfort induced by commonly used oral local anesthetic injections. Anesth Prog. 2005;52(4):122-127.
13. Oikarinen VJ, Ylipaavalniemi P, Evers H. Pain and temperature sensations related to local anesthesia. Int J Oral Surg. 1975;4(4):151-156.
14. Malamed SF. Handbook of Local Anesthesia. 5th ed. St. Louis, MO: Elsevier Mosby; 2004.
15. Farsakian LR, Weine FS. The significance of needle gauge in dental injections. Compend Contin Educ Dent. 1991;12(4):262-268.
16. Brownbill JW, Walker PO, Bourcy BD, Keenan KM. Comparison of inferior dental nerve block injections in child patients using 30- gauge and 25- gauge short needles. Anesth Prog. 1987;34(6):215-219.
17. Fuller NP, Menke RA, Meyers WJ. Perception of pain to three different intraoral penetrations of needles. J Am Dent Assoc. 1979;99(5):822-824.
18. Mollen AJ, Ficara AJ, Provant DR. Needles–25 gauge versus 27 gauge–can patients really tell? Gen Dent. 1981;29(5):417-418.
19. Flanagan T, Wahl MJ, Schmitt MM, Wahl JA. Size doesn’t matter: needle gauge and injection pain. Gen Dent. 2007;55(3):216-217.
20. Aldous JA. Needle deflection: a factor in the administration of local anesthetics. J Am Dent Assoc. 1968;77(3):602-604.
21. Jeske AH, Boshart BF. Deflection of conventional versus non-deflecting dental needles in vitro. Anesth Prog. 1985;32(2):62-64.
22. Steele AC, German MJ, Haas J, et al. An in vitro investigation of the effect of bevel design on the penetration and withdrawal forces of dental needles. J Dent. 2013;41(2):164-169.
23. Steinkruger G, Nusstein J, Reader A, et al. The significance of needle bevel orientation in achieving a successful inferior alveolar nerve block. J Am Dent Assoc. 2006;137(12):1685-1691.
24. Robison SF, Mahew RB, Cowan RD, Hawley RJ. Comparative study of deflection characteristics and fragility of 25-, 27-, and 30- gauge short dental needles. J Am Dent Assoc. 1984;109(6):920-924.
25. Pashley EL, Nelson R, Pashley DH. Pressures created by dental injections. J Dent Res. 1981;60(10):1742-1748.
26. Diggle L, Deeks JJ, Pollard AJ. Effect of needle size on immunogenicity and reactogenicity of vaccines in infants: a randomized controlled trial. BMJ. 2006;333(7568):571.
27. King L. Subcutaneous insulin injection technique. Nurs Stand. 2003;17(34):45-52.
28. Trombelli L, Nonato M, Ferrari-Carpino C, et al. Needles in dental practice. Clinical evaluation and experiments on deformation and siliconization. G Anest Stomatol. 1990;19(2):7-14.
29. Kinast P. Quality testing of medical needles-laboratory and practice. Med Device Technol. 1992;3(6):46-49.
30. Daublander M, Muller R, Lipp MD. The incidence of complications associated with local anesthesia in dentistry. Anesth Prog. 1997;44(4):132-141.
31. Pogrel MA. Broken local anesthetic needles: a case series of 16 patients, with recommendations. J Am Dent Assoc. 2009;140(12):1517-1522.
32. Smith MH, Lung KE. Nerve injuries after dental injection: a review of the literature. J Can Dent Assoc. 2006;72(6):559-564.
33. Rout PG, Saksena A, Fisher SE. An investigation of the effect on 27-gauge needle tips following single local anesthetic injection. Dent Update. 2003;30(7):370-374.
34. Almendros Marqués NA, Delgado Molina Ed, Tamarit Borras M, et al. Comparison of two needle models in terms of bevel deformation during truncal block of the inferior alveolar nerve. Med Oral Patol Oral Cir Buccal. 2007;12(4):E317-322.
35. Sanchez DE, Fernandez RE. Microscopic assessment of dental needles. University Centre of Health Sciences, Guadalajara University. http://www/septodont.com.br/pdfs/BevelEvaluationGB.doc. Accessed August 26, 2014.
36. Safer A, Behbehani E, Al Hadad A, et al. Dental anaesthesia needle: a NEDS study. Annals of the first African and Middle-East IADR Federation conference. Jabriya-Kuwait; 2005
37. Behbehani E, Al-Hadad A. Effect of length and gauge on performance of dental anesthesia needles: a strain study. Dental News. 2006;13(3):12-20.
38. Albergo G, Bedini R, Pain S, et al. Mechanical evaluation of new injection needles for dental anesthesia. Minerva Stomatol. 2008;57(1-2):9-20.