You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Dental anxiety poses significant challenges for patients and dental care providers.1-3 Evidence suggests that anxiety inhibits individuals from seeking oral care services, leading to a vicious cycle of inconsistent dental visits that may contribute to the deterioration of oral health.4-9 Dental anxiety is generally defined as nonspecific lack of ease, apprehension, or negative thoughts about what may happen during a dental appointment. The specific cause of dental anxiety is unknown; however, researchers believe it results from a previous traumatic experience or from vicarious learning.10 People can develop dental anxiety at any stage of their lives, but childhood onset is often associated with a pattern of more severe and negative responses compared to onset during adolescence or adulthood.10 Noncognitive triggers, such as fear of the unknown, previous negative experiences, and perceptions of family members, friends, and the media, can increase dental anxiety.11 Cognitive factors such as vulnerability, negative expectations, patient–clinician relationships, perceptions of powerlessness, and negative thoughts appear to have greater impacts on dental anxiety than do noncognitive factors.11
Okawa et al concluded that patients reported high dental pain when their anxiety levels were also high.12 Fear of pain and negative previous experiences are reported as the primary reasons that individuals feel anxious during dental hygiene procedures.13,14 Consequently, it is important to manage dental anxiety to help reduce pain. Procedures, such as periodontal probing or scaling and root debridement, may elicit some level of pain coupled with anxiety; thus, these procedures represent scenarios that need to be controlled.8
The use of adjunctive therapy to reduce dental anxiety is not a new concept. The American Dental Association (ADA) supports the responsible use of pharmacological agents to manage anxious patients.15 Currently, general classes of drugs used to manage pain and anxiety include nonsteroidal anti-inflammatory drugs, acetaminophen, opioids, benzodiazepines, selective serotonin reuptake inhibitors, tricyclic antidepressants, and monoamine oxidase inhibitors.15,16 Although pharmaceutical medications can help patients with anxiety, the efficacy of these therapies is not guaranteed. Non-pharmacological interventions such as patient-centered communication, biofeedback, deep breathing exercises, and music distraction also have limitations. Therefore, additional non-pharmacological techniques, such as audiovisual immersion therapy, altered reality, and music distraction, are being studied to assist anxious patients. The use of ancillary therapies may help individuals have more positive overall experiences. These approaches allow patients to focus on the environment as a distraction from sensory factors such as fear, anxiety, and pain.17-25 Such distraction therapy may not only comfort the patient, but help the clinician provide better care to a more relaxed individual. Although distraction techniques partially interfere with the environment, the patient and the clinician are still able to interact and communicate.
The use of distraction techniques such as immersive visualization (IV), virtual reality (VR), and audiovisual (AV) are novel approaches to managing a wide variety of conditions. Although the exact neurobiological mechanism behind distraction techniques is unclear, these systems have been shown to reduce elements such as stress, general distress, pain, anxiety, and fear without interfering with treatment. For example, the use of AV distraction minimized children’s discomfort and distress during dental restorative treatments.22 Similarly, AV distraction reduced adults’ anxiety and fear during an oral prophylaxis and was associated with shorter appointment times.23 Likewise, immersive VR techniques were able to minimize anxiety and pain during scaling and root planing.24 All of the participants reported they had a positive experience and would use the distraction systems for future dental procedures.22-24
The purpose of the present study was to evaluate the effects of a portable immersive visualization eyewear system on adult anxiety during routine oral prophylaxis.
Methods and Materials
The study was conducted at the Dental Hygiene Research Center at Old Dominion University. Institutional review board approval was obtained prior to the beginning of the study. Participants were recruited through flyers and the university’s campus-wide email system. Informed consent was obtained prior to data collection.
At screening, a full-mouth oral examination was performed to assess periodontal status, caries, and dental calculus. One experienced dental hygienist performed all procedures in a single 1-hour appointment. Volunteers were enrolled in the study if they were: 18 years or older, scored a 9 or higher on the Corah’s Dental Anxiety Scale Revised (DAS-R),26 and were generally healthy. Subjects were excluded if they presented with severe dental calculus (Class IV or V), severe periodontal disease (American Academy of Periodontology status of 3 or higher), severe dental caries (3 or more open large lesions), required antibiotic premedication, reported the current use of anxiety medication or psychotropic drugs, or had a history of seizures or convulsive disorders, vertigo, or equilibrium disorder. Subjects were excluded if they were medically treated for anxiety. The researchers were not authorized to provide medical advice and no other mental health tests or guidance was provided. During treatment if participants felt uncomfortable with the IV eyewear or dental procedures, they were free to exit the study. Individuals who did not qualify for the study because of excessive caries, periodontal disease, or dental calculus were referred to the dental hygiene care facility at the same institution for evaluation.
A split-mouth design was utilized using a left/right side comparison rather than half of the subjects using the IV and the other half not because of the variation in perception of anxiety. By using this method the same individual rated their level of anxiety with and without the use of the IV system. Subjects were randomly assigned into two groups: Group A used IV during the first half of the appointment and Group B wore IV during the second half of the appointment.
Portable Immersive Visualization Vuzix iWear AV 920 video eyewear, which costs approximately $200, was integrated with a common smartphone (iPhone 5) to render videos (Figure 1). A small black disposable cloth barrier was attached to the top of the IV headset to minimize light and outside distractions. Subjects’ peripheral vision was not constricted in an attempt to minimize any anxiety that might result from such “unknowns” as the unfamiliar treatment room and instruments.
Prior to IV treatment, subjects had the opportunity to select one of three videos:
1. A documentary about Oregon
2. A set of music videos
3. An episode of Mr. Bean, a popular comic TV series
Subjects could use a Bluetooth switch to display the video with audio, listen to the audio only, or stop the video and audio. Subjects were able to adjust the volume and could turn the IV eyewear off at any time. Instructions for using the IV system were provided to all participants prior to starting the treatment.
The DAS-R was identified as a reliable instrument for assessing dental anxiety.26,27 The DAS-R was scored and recorded at screening to determine eligibility and again at baseline to validate the subject’s anxiety status. The DAS-R consists of four multiple-choice questions that measure anxiety levels related to dental visits. Total possible scores range from 4 to 20 points: 15 to 20 (severe anxiety), 13 to 14 (high anxiety), 9 to 12 (moderate anxiety), and 8 or less (low anxiety). The Calmness Scale was a researcher-designed question: “How calm do you feel right now?” which was scored and recorded before and after IV treatment, on a 7-point Likert scale. Scores ranged from 1 (very calm) to 7 (less calm).
After the completion of the oral prophylaxis, subjects completed a post-IV opinion survey. Items were scored on a 7-point Likert scale. The survey consisted of following three questions:
1. How anxious were you during your dental treatment when wearing the Immersive Visualization eyewear (1 = not anxious to 7 = very anxious)?
2. Did you find wearing the Immersive Visualization eyewear helped to reduce your anxiety during treatment (1 = not at all to 7 = very much)?
3. Did you enjoy wearing the eyewear during the treatment (1 = not enjoyable to 7 = very enjoyable)?
Statistical Analysis
Data were entered into Microsoft Excel for Mac 2011 (Microsoft Corporation Version 14.3.5) and analyzed with SAS® 9.3 statistical software. Data were reviewed three times for validity and quality assurance. Descriptive statistics and analysis of variance (ANOVA for Generalized Linear Regression Model) fits were carried out with a level of significance of 0.05.
Results
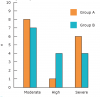
Fifty individuals were screened for the study, and 30 subjects qualified. The sample was composed of 23 females (76.7%) and 7 males (23%) with a mean age of 29.96 ± 7.8 (ranging from 18 to 51 years). Fourteen subjects (46.7%) self-identified as Caucasian, 6 (20%) as African American, 5 (16.65%) as Hispanic, and 5 (16.65%) as Asian. At baseline, 15 subjects (50%) self-reported moderate anxiety, 5 (16.7%) high anxiety, and 10 (33%) severe anxiety on the DAS-R scale (Figure 2). Female subjects reported higher levels of anxiety than men, both before treatment (female 4.83 ± 0.94 versus male 4.42 ± 0.53) and after (female 2.83 ± 1.70 versus male 2.00 ± 1.15).
The DAS-R was scored at baseline to determine anxiety levels. The results showed no statistically significant differences between groups with regard to the baseline anxiety (Group A = 13.33 ± 3.15 and Group B = 12.93 ± 2.40, P = .7).
Comparisons of calmness mean scores are presented in Table 1. Group A used the IV system during the right side of treatment while Group B used the IV system during the left side of treatment. Within Group A, the ANOVA fit showed a statistically significant difference in calmness (P < .01) between pre (4.66 ± 1.04) and post (2.93 ± 1.22) in IV use. Likewise, within Group B the fit revealed a statistically significant difference (P < .01) between pre (4.33 ± 1.54) and post (2.13 ± 0.99) in calmness with IV treatment. Results indicate that the use of IV system during oral debridement had a positive effect in lowering anxiety levels in the adult population. Regardless of whether subjects started wearing the IV system at the beginning of the appointment (Group A), or as the clinician switched sides (Group B), anxiety was reduced. Combined calmness mean scores data of Group A and Group B showed a decrease from 4.50 ± 1.31 pre-IV treatment to 2.53 ± 1.17 posttreatment, which indicates all participants benefitted.
Prior to oral prophylaxis, subjects had the opportunity to choose the type of video they wanted to watch: 15 (50%) chose the documentary, 10 (33%) subjects opted for the music videos, and 5 (17%) chose the comic TV show. None of the participants elected to stop the video or audio while wearing the IV system.
Results obtained from the Post IV Opinion survey are displayed in Table 2. Subjects responded positively to wearing the IV eyewear system and they felt it helped to reduce their level of anxiety. During posttreatment debriefing, all the subjects reported that wearing the IV eyewear was enjoyable and did not interfere with treatment procedures. The clinician also reported that the IV system did not interfere with treatment.
Discussion
Patients with dental anxiety may exhibit behaviors that make rendering treatment difficult and may keep them from seeking oral care, thus contributing to the deterioration of their oral health. The aim of this study was to determine whether a portable IV eyewear system could reduce anxiety in adult patients during oral prophylaxis treatment. Previous investigations have offered patients the use of head-mounted AV and music distraction during dental and dental hygiene procedures with similarly positive experiences.18,19,21-24 IV was determined to be a safe, economical, easy-to-use, non-pharmacological approach to short-term reduction of dental anxiety. The present study is in line with other studies that have shown females are more prevalent to report or experience dental anxiety and fear when compared to the male population.1-4,8,11,14,28 The authors also postulate that perhaps more women seek out dental treatment than men and are more comfortable in reporting their anxiety and fear.
Results from the Calmness Scale showed Group A to be slightly more anxious compared to Group B. One possible explanation could be that Group A started with higher mean calmness scores compared to group B (4.6 and 4.3, respectively). From the study design, Group A started using the IV eyewear in the beginning of the appointment and was not wearing the IV on the second half of the study. Both groups showed statistically significant differences in anxiety levels between pre- and post-IV eyewear use. Group B’s level of anxiety did not change significantly during the first half of the treatment without the use of IV, but was more than 50% lower after the IV treatment. Several other confounding factors could be the reason for such disparities. One factor may be that Group A enrolled a higher ratio of women (n = 13) compared to men (n = 2) and included more individuals with severe anxiety (n = 6) compared to Group B (n = 4).
Nausea has been reported as one of the possible side effects of virtual reality and virtual immersion;29 however, in the present study, none of the subjects experienced this side effect. Two subjects reported that the IV equipment was “heavy” and “uncomfortable,” and one subject reported missing the patient–clinician interaction during the procedure, but all subjects reported that they would wear the IV system during dental care if available. In future studies, using a microphone connected to the IV system headset is recommended to provide better communication between the patient and the clinician.
Study Limitations
Although the sample size was relatively small, information gathered in this study can be used to validate previous research and to provide support for future studies. Neither the clinician nor the subjects were blinded to the treatment; due to design study characteristics, this was not feasible. There is some evidence that anxiety may influence blood pressure and heart rate during dental treatment.23,30 The present study did not include monitoring vital signs although this may be a consideration for other research. Future studies should also consider expanding the questionnaire to include age of anxiety onset since literature suggests that variations occur among age of traumatic dental experience and management techniques.10 The portable IV system used in this study did not constrict the patient’s peripheral vision because it was believed that leaving some peripheral vision may provide additional comfort to the subjects. It is also important to note that researchers relied on participants’ self-reported levels of anxiety and calmness. The use of additional screening tools to identify patients who are anxious may merit further investigation.
Conclusion
Evidence in the literature indicates that dental anxiety is a very real problem that can complicate oral care or prevent individuals from seeking dental services all together. Because the portable IV system used in this study operates with a common smartphone and an affordable head-mount display, this state-of-the-art technology has the potential to become widely adopted as a distraction technique. Results from this study support the use of IV eyewear as an effective distraction technique to help decrease or manage short-term anxiety in adult patients during routine oral debridement.
About the Authors
Carmelo Padrino-Barrios, BSDH, MS, works in private practice in Oakton, Virginia. Gayle McCombs, RDH, MS, is a professor and graduate faculty at the School of Dental Hygiene, Old Dominion University. Norou Diawara, PhD, is an associate professor and the statistics graduate program director in the Mathematics and Statistics Department at Old Dominion University. Gianluca De Leo, PhD, MBA, is the Chair of the Clinical and Digital Health Sciences Department at Augusta University.
References
1. Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety—an epidemiological study on its clinical correlation and effects on oral health. J Oral Rehabil. 2006;33(8):588-593.
2. Doerr P, Lang P, Nyquist L, Ronis D. Factors associated with dental anxiety. J Am Dent Assoc. 1998;129(8):1111-1119.
3. Fiset L, Milgram P, Weinstein P, Melnick S. Common fears and their relationship to dental fear and utilization of the dentist. Anesth Prog. 1989;36:258-264.
4. De Jongh A, Stouthard M. Anxiety about dental hygienist treatment. Community Dent Oral Epidemil. 1993;21:91-95.
5. Locker D. Psychosocial consequences of dental fear and anxiety. Community Dent Oral Epidemiol. 2003;31:144-151.
6. Okawa K, Ichinohe T, Kaneko Y. Anxiety may enhance pain during dental treatment. Bull Tokyo Dent Coll. 2005;46(3):51-58.
7. Hakeberg M, Cunha L. Dental anxiety and pain related to dental hygienist treatment. Acta Odontologica Scandinavica. 2008;66(6):374-379.
8. Sanikop S, Agrawal P, Patil S. Relationship between dental anxiety and pain perception during scaling. J Oral Sci. 2011;53(3):341-348.
9. DeDonno M. Dental anxiety, dental visits and oral hygiene practices. Oral Health Preventive Dentistry. 2012;10(2):129-133.
10. Locker D, Liddell A, Dempster L, Shapiro D. Age of onset of dental anxiety. J Dent Res. 1999;78(3):790-796.
11. Carrillo-Diaz M, Crego A, Armfield JM, Romero-Maroto M. Assessing the relative efficacy of cognitive and non-cognitive factors as predictors of dental anxiety. Eur J Oral Sci. 2012;120(1):82-88.
12. Okawa K, Ichinohe T, Kaneko Y. Anxiety may enhance pain during dental treatment. Bull Tokyo Dent Coll. 2005;46(3):51-58.
13. Fardal O, Hansen B. Interviewing self-reported highly anxious patients during periodontal treatment. J Periodontol. 2007;78(6):1037-1042.
14. Guzeldemir E, Toygar HU, Cilasun U. Pain perception and anxiety during scaling in periodontally healthy subjects. J Periodontol. 2008;79(12):2247-2255.
15. Guidelines for the Use of Sedation and General Anesthesia by Dentists. American Dental Association [Internet]. 2012 [cited 2014 September 15]. Available from: http://www.ada.org/~/media/ADA/About%20the%20ADA/Files/anesthesia_use_guidelines.ashx.
16. Huang D, Wun E, Stern A. Current treatments and advances in pain and anxiety management. Dent Clin N Am. 2011;55(3):609-618.
17. Botella C, Gracia-Palacios A, Banos R, et al. Virtual reality in the treatment of pain. J Cyber Therapy & Rehabil. 2008;1(1):93-100.
18. Man AKY, Yap JCM, Kwan SY, et al. The effect of intra-operative video on patient anxiety. Anaesthesia. 2003;58(1):64-68.
19. Lahmann C, Schoen R, Henningsen P, et al. Brief relaxation versus music distraction in the treatment of dental anxiety. J Am Dent Assoc. 2008;139(3):317-324.
20. Taylor V, Stevens R, Canfield T. Performance models of interactive, immersive visualization for scientific applications. Proceedings of the International Workshop on High Performance Computing for Computer Graphics [Internet]. 1995 [cited 2012 September 19]. Available from: http://citeseerx.ist.psu.edu/viewdoc/ summary?doi=10.1.1. 45.2930.
21. Parsons TD, Rizzo AA. Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: A meta-analysis. J Behav Ther Exp Psychiatry. 2008;39(3):250-261.
22. Ram D, Shapira J, Holan G, et al. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int. 2010;41(8):673-679.
23. Frere CL, Crout R, Yorty J, McNeil DW. Effects of audiovisual distraction during dental prophylaxis. J Am Dent Assoc. 2001;132(7):1031-1038.
24. Furman E, Jasinevicius TR, Bissada NF, et al. Virtual reality distraction for pain control during periodontal scaling and root planing procedures. J Am Dent Assoc. 2009;140(12):1508-1516.
25. Wismeijer AAJ, Vingerhoets JJM. The use of virtual reality and audiovisual eyeglass systems as adjunct analgesic techniques: A review of the literature. Annals Behav Med. 2005;30(3):268-278.
26. Corah N. Development of a dental anxiety scale. J Dent Res. 1969;48(4):596.
27. Humphris GM, Freeman R, Campbell J, et al. Further evidence for reliability and validity of the modified dental anxiety scale. Int Dent J. 2000;50(6):367-370.
28. Heft MW, Meng X, Bradley MM, Lang PJ. Gender differences in reported dental fear and fear of dental pain. Community Dent Oral Epidemiol. 2007;35(6):421-428.
29. Virtual Reality - How Does It Affect Us. Virtual Reality [Internet]. 2009 [cited 2014 October 6]. Available from: http://www.vrs.org.uk/virtual-reality/how-does-it-affect-us.html.
30. Fernandes Goulart JC, Dias Pinhero M, Ventura Rodrigues R, et al. Influence of anxiety on blood pressure and heart rate during dental treatment. Rev Odonto Ciencia. 2012;27(1):31-35.