You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Sleep breathing disorders, such as obstructive sleep apnea (OSA) and snoring, are the result of the unconscious collapse of the pharyngeal airway during sleep. OSA and snoring both have strong associations with the potential development of cardiovascular disease from vascular oxidative stress-inflammation (VOS).1 Oxidative stress induced by nocturnal hypoxia generates reactive oxygen species from leukocytes, reduced plasma levels of nitrite, increased lipid peroxidation, and lower antioxidant capacity. This is the mechanism that results in cardiovascular disease, for both adults and children. VOS can create increased blood clotting, which can lead to stroke and heart attack.
Meta-analyses by multiple groups have found the use of oral appliances for OSA to be equivalent to continuous positive airway pressure (CPAP) at reducing blood pressure in adults.2-4 Snoring patients have been shown to have a five-times increased risk of OSA.5 In women, regular snoring is associated with increased risk of coronary heart disease (risk ratio [RR] 2.18) and stroke (RR 1.88).6 Snoring was found to be a greater determinant factor of VOS than OSA7 and leads to an increased risk of carotid artery atherosclerosis.8,9
There are four components of OSA: Pcrit (critical pressure to collapse the pharyngeal airway), muscle tonus or recruitment, loop gain (response to apnea-transition to breathing), and arousal threshold (length of time it takes to be awakened to begin breathing). Pcrit and muscle tonus can be affected by the use of oral appliances, medications, and positive pressure, as well as surgery, orthopedic development in children, and myofunctional therapy, with the latter having been shown to reduce OSA by 50% in adults and 62% in children.10 Conversely, loop gain and arousal threshold are neurologic conditions. Carbon dioxide sensitivity is the main factor in these mechanisms. They are treated with medications, nasal breathing training, and exercises.
This article focuses on the function, design, and materials for optimal oral appliance therapy (OAT) to treat snoring and OSA.
Background on Oral Appliances
In the early 20th century, French dental surgeon Pierre Robin was the first to identify OSA in children with micrognathia (ie, a small lower jaw) and glossoptosis (ie, posterior tongue displacement into the pharynx). He produced the first oral appliance, which he termed the "monobloc." A detailed review of the history of OAT can be found in "The evolution of oral appliance therapy for snoring and sleep apnea," written by Demko in 2018.11 In 2005, the American Academy of Sleep Medicine's (AASM) practice parameters made the following recommendation: "[Oral appliances] are indicated for use in patients with mild to moderate OSA who prefer them to CPAP therapy, or who do not respond to, are not appropriate candidates for, or who fail treatment attempts with CPAP."12
The apnea-hypopnea index (AHI) is the combined average number of apneas and hypopneas that occur per hour of sleep. According to the AASM, AHI is categorized as mild (5 to <15 events per hour), moderate (15 to <30 events per hour), and severe (≥30 events per hour). Overall, OAT for OSA as compared to positive airway pressure (PAP) is less effective in AHI reduction; however, it is equally efficacious in symptom control, health benefits, and affordability. OAT is superior to PAP in adherence, tolerance, patient partner acceptance, and convenience.13 In patients with mild to moderate OSA, research has demonstrated that there are no differences in AHI reduction between OAT and nasal CPAP.14 The average compliance with OAT is more than 6 to 7 hours per night,15-18 while the average compliance with PAP is around 3.3 hours per night.19,20
French physician and researcher Christian Guilleminault, the developer of the AHI system, stated that the ultimate goal in the treatment of sleep apnea is the transformation of oral breathing to nasal breathing, both day and night.21 Regardless of the level of sleep pathology (eg, snoring, upper airway resistance syndrome, or OSA), four points of respiratory obstruction must be patent for proper breathing during sleep, as illustrated in Figure 1: the nasal valve, nasal pharynx, velopharynx, and oropharynx.22
Mechanism of Action
Oral appliances work by giving tonus to the muscles of the throat by mandibular positioning, specifically the velopharynx (ie, the narrowest portion of the pharyngeal airway, involved in 81% of patient cases) and the oropharynx (involved in 21.9% of patient cases).22 They directly affect muscle tonus (muscle responsiveness) and Pcrit in these areas.23 In addition, besides mandibular position, tongue position also requires management for effective treatment. Tongue restraining devices have been shown to affect upper airway structures in OSA in a similar manner to oral appliances.24 The use of a tongue positioner added to an oral appliance base can increase efficacy without discomfort by applying active force to the tongue in patients who are incomplete responders.25
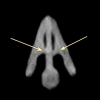
The two most significant predictive factors in OAT success are body mass index and nasal airway resistance.26 Nasal dilators have become an important component of OSA therapy. Nasal valve dilation has been shown to decrease intraluminal pressures in the oropharynx via the Starling resistor model, reducing apneic events.27 The Starling resistor model states that the pharyngeal airway (muscle) experiences increased extraluminal pressure as each end of the airway's cartilage (nasal valve and epiglottis) is narrowed. A recent multicenter retrospective analysis found a statistically significant association between nasal valve compromise (Figure 2) and temporomandibular joint (TMJ) capsulitis (odds ratio 3.73) and facial and cervical myositis (odds ratio 6.97).28
Appliance Design
Oral appliances used to treat snoring and OSA have the following capabilities and/or characteristics: maintain and/or advance the mandible in the supine position; be titratable, durable, retentive, adjustable, comfortable, and minimally invasive; provide minimal tooth movement; reduce the risk of temporomandibular disorder (TMD) or joint pain; and be US Food and Drug Administration (FDA)-cleared. These factors are especially important in light of the fact that 50% of patients discontinue use of an oral appliance in the first year.29
Oral appliances are essentially either monoblock or bi-block. Monoblock style is a one-piece device that engages both the upper and lower dentitions, while a bi-block device comprises separate upper and lower appliances that are joined by a connecting piece, allowing for adjustment or titration. Monoblock was found to be more effective than bi-block in a systematic review and meta-analysis.30
Immobilization of the TMJs while sleeping may lead to joint and facial muscle symptoms, as all joints require movement to lubricate. A normal rhythmic masticatory muscle activity occurs during sleep, which should not be confused with sleep bruxism. The protrusive advancement mechanisms in bi-block oral appliances are either elastics, rods, jack screws, hinges, or blocks for dorsal fin appliances. Hinge appliances may be lateral, such as the Herbst or lingual connector. Oral appliances typically are either made of acrylic (methyl methacrylate), have a pressure-molded base with acrylic, or are 3D-printed with type 12 nylon. Acrylic appliances are usually thicker than other types, so they have a greater effect on reducing oral volume. A summary of the advantages and disadvantages of the various oral appliance materials is provided below in the "Oral Appliance Materials" section.
It is important to note that Medicare has certain requirements for oral appliances, such as Herbst and hook mechanisms that act as "mechanical hinges." Also, oral appliances for OSA and snoring must be FDA-cleared for insurance coverage. Some insurance policies now require pricing, data, analysis, and coding (PDAC) certification.
Oral volume should always be considered when choosing an oral appliance design. Whether the patient has macroglossia, micrognathia, or any combination of anatomic compromise, appliances should be as thin and small as possible, as patients prefer appliances that are less bulky and minimize the interincisal vertical opening.31 The vertical changes that are necessary for appliance fabrication are balanced with lip size so the patient can maintain adequate lip seal during sleep and minimize drooling. The tongue should be managed (ie, prevented from retruding), especially in patients with tongues that retract on opening. Custom-made appliances generated from impressions or scans of the mouth and mounted on mechanical or virtual articulators have been found to be more effective and preferred by patients with snoring and/or OSA than premade over-the-counter devices.32,33
Oral Appliance Materials
Hard Acrylic
Advantages of oral appliances made of hard acrylic are that they can be adjusted or repaired easily at chairside-the appliance can be ground down it if it is too tight, or more acrylic can be added if it is too loose-and they are easy to insert and remove with the use of ball clasps. Additionally, if minor dental changes occur in the patient, hard acrylic can sometimes be modified rather than having to fabricate a new appliance. These appliances also complement most dentitions, and clasps can be added for stronger retention.
On the downside, hard acrylic appliances are very rigid; for patients with sensitivities, these appliances may feel tight and can irritate the gums and/or teeth. Also, because this material is less forgiving, it is critical to acquire accurate impressions to prevent chairside adjustment. Other drawbacks of hard acrylic appliances are that they wear over time with patients who brux, the rather bulky material may force the tongue to move posteriorly and reduce oral volume, and the porous material can leach, yielding a bad taste, irritation, and discoloration and attracting bacteria.34-37
Thermal Acrylic
Working with thermal acrylic oral appliances requires a learning curve for dentists, who must get a "feel" for how hot the water used for forming the appliance must be and how long the appliance must be left in the mouth before removing it. Also, more frequent replacement may be needed as compared to hard acrylic appliances, especially for clenchers or bruxers. These appliances also have a shorter shelf-life due to the composition of the material, as it breaks down over time due to its porosity.
There are numerous advantages to thermal acrylic, however. Because this material is soft and pliable at warm temperatures, it allows for comfortable and easy seating, which helps engage undercuts that harder materials such as acrylic cannot. It also provides better retention for a crowded dentition because the material can flex; clasps can be added for further retention. The pliability of thermal acrylic allows the material to flex over crowns and bridges, making it a good choice for patients with restorations, as well as those with sensitivities and edentulous patients (provided they have a good bony ridge).
Dual Laminate
These appliances possess the rigidity of hard acrylic externally with a soft inner liner that buffers the teeth/tissue. They have more "give," requiring less blockout, and they are recommended for patients with sensitive teeth or cosmetic dental work.
Disadvantages of dual laminate oral appliances include the following: they are not as durable as hard acrylic; the soft side can delaminate and absorb moisture; the porous material yellows over time and, depending on diet, may require more frequent replacement; and clasps and acrylic cannot be added for further retention. Moreover, these appliances can be difficult to adjust, as the material "gums up" when using a high-speed bur; low speed has little to no effect on the soft material.
Polyamide/Nylon
The introduction of type 12 nylon appliances, which are CAD/CAM printed devices, has been a momentous advancement, allowing for appliance size reduction and increased comfort, accuracy, and durability. These devices are designed using proprietary software specific to each manufacturer and printed using selective laser sintering technology that ensures a consistent and accurate device. Digital impressions are captured using intraoral or desktop scanners; offices are not required to own a scanner as laboratories can digitize stone models to an STL format. By transitioning to a digital process, offices can eliminate the patient discomfort and inconvenience of physical impressions and bite registrations as well as the need to store bulky physical models. The introduction of CAD design also allows laboratories to digitize their workflow, which greatly reduces the fabrication process and turnaround times. Design changes can be made with superior accuracy and minimal effort, allowing for a high degree of customizable devices to suit the complex anatomy of individual patients.
Other Factors Associated With Oral Appliances
Side effects such as jaw and muscle pain, drooling, tooth sensations, tongue tenderness, problems with swallowing, and bite changes are common with the use of oral appliances for snoring and OSA.38 Posterior open bite has been found to occur in almost 18% of patients using oral appliances for OSA.39 Clinically significant changes in occlusion are progressive in nature with appliance usage. These include reduction of overbite and overjet, less anterior crowding, increase in lower canine width, and molars assuming more of a class I relationship.40-42
OSA is strongly associated with TMD, primary headaches (migraine, tension type, cluster), and sleep bruxism.43 Conservative appliance introduction is important to minimize side effects. It has been demonstrated that the number of side effects increases as protrusion exceeds 50% from baseline.44 Bite techniques that reduce the need for protrusive adjustments, such as phonetics, minimize the risk of these side effects. A study comparing the George Gauge® (GG) and phonetic techniques found that they have equal efficacy; however, the phonetic technique required less than one adjustment per patient while the GG required 2.7 adjustments, starting at 50% protrusion.45 Because the phonetic technique is physiologic and 3-dimensional, minimal protrusion of the mandible is needed to achieve an increased volume and reduced collapse of the pharyngeal airway.46
For patients with severe apnea, predominately central apneas, obesity, a large tongue, small oral volume, TMD, TMJ osteoarthritis, temporal headaches, PAP compliance issues, or any combination of these conditions, hybrid therapy combining OAT and CPAP has been shown to be effective.47,48 Connecting a nasal PAP delivery device to the oral appliance lowers titration pressure and eliminates the use of head straps that can result in headache or aggravate patients prone to headaches and claustrophobia.
Conclusion
Many dental pathologies that dentists treat every day, such as bruxism, tooth wear, abfraction lesions, cracked teeth, periodontitis, and caries, are comorbid with OSA. The American Dental Association recommends that all dental patients be screened for sleep breathing disorders. Although custom-made oral appliances to treat snoring and OSA when compared to all levels of severity with PAP are less effective in AHI reduction, their usage is equally efficacious in symptom control, health benefits, and affordability. Moreover, positive pressure therapies have low utilization. OAT is superior to PAP in adherence, tolerance, patient partner acceptance, and convenience. In patients with mild to moderate OSA, no differences in AHI reduction have been shown between OAT and nasal CPAP. Sometimes hybrid therapy may be indicated, thus allowing dentists to participate in even the most severe cases of OSA.
Advances in technology have led to improvements in the design and fabrication of oral appliances to treat snoring and OSA. Training for the treatment of OSA in dental schools is still limited; however, it is increasing. OSA is associated with primary headaches, orofacial pain, and TMD. Nasal obstruction has been found to be comorbid with facial/cervical myositis and capsulitis of the TMJ. Because of the frequency of these conditions, all dentists should be aware of sleep breathing pathology. Special training is needed in this area, and board certification can be achieved through continuing education courses and written and oral examinations by accredited academies.
About the Author
Steven R. Olmos, DDS
Private Practice, La Mesa, California; Past President, American Academy of Craniofacial Pain; Diplomate, American Board of Dental Sleep Medicine; Diplomate, American Board of Craniofacial Pain; Diplomate, American Board of Craniofacial Dental Sleep Medicine
Queries to the author regarding this course may be submitted to authorqueries@broadcastmed.com.
References
1. Eisele HJ, Markart P, Schulz R. Obstructive sleep apnea, oxidative stress, and cardiovascular disease: evidence from human studies. Oxid Med Cell Longev. 2015;2015:608438.
2. Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773-827.
3. Zhang M, Liu Y, Liu Y, et al. Effectiveness of oral appliances versus continuous positive airway pressure in treatment of OSA patients: an updated meta-analysis. Cranio. 2019;37(6):347-364.
4. De Vries GE, Wijkstra PJ, Houwerzijl EJ, et al. Cardiovascular effects of oral appliance therapy in obstructive sleep apnea: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:55-68.
5. Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):
1230-1235.
6. Hu FB, Willett WC, Manson JE, et al. Snoring and risk of cardiovascular disease in women. J Am Coll Cardiol. 2000;35(2):308-313.
7. Alvarez RF, Cuadrado GR, Arias RA, et al. Snoring as a determinant factor of oxidative stress in the airway of patients with obstructive sleep apnea. Lung. 2016;194(3):469-473.
8. Lee SA, Amis TC, Byth K, et al. Heavy snoring as a cause of carotid artery atherosclerosis. Sleep. 2008;31(9):1207-1213.
9. Kirkham EM, Hatsukami TS, Heckbert SR, et al. Association between snoring and high-risk carotid plague features. Otolaryngol Head Neck Surg. 2017;157(2):336-344.
10. Camacho M, Cetal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38(5):669-675.
11. Demko BG. The evolution of oral appliance therapy for snoring and sleep apnea: where did we come from, where are we, and where are we going? Sleep Med Clin. 2018;13(4):467-487.
12. Kushida CA, Morgenthaler TI, Litler MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep. 2006;29(2):240-243.
13. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013;187(8);879-887.
14. Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Oral appliance therapy versus nasal continuous positive airway pressure in obstructive sleep apnea: a randomized, placebo-controlled trial. Respiration. 2011;81(5):411-419.
15. Lowe AA, Sjoholm TT, Ryan CF, et al. Treatment, airway and compliance effects of a titratable oral appliance. Sleep. 2000;23(suppl 4):S172-S178.
16. Vanderveken OM, Dieltjens M, Wouters K, et al. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax. 2013;68(1):91-96.
17. Dieltjens M, Verbruggen AE, Braem MJ, et al. Determinants of objective compliance during oral appliance therapy in patients with sleep-disordered breathing: a prospective clinical trial. JAMA Otolaryngol Head Neck Surg. 2015;14(10):894-900.
18. Bachour P, Bachour A, Kauppi P, et al. Oral appliance in sleep apnea treatment: respiratory and clinical effects and long-term adherence. Sleep Breath. 2016;20(2):805-812.
19. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919-931.
20. Mokhlesi B, Ayas NT. Cardiovascular events in obstructive sleep apnea - can CPAP therapy SAVE lives? N Engl J Med. 2016;375(10):994-996.
21. Guilleminault C, Sullivan SS. Towards restoration of continuous nasal breathing as the ultimate treatment goal in pediatric obstructive sleep apnea. Enliven: Pediatr Neonatol Biol. 2014:1(1):1-5.
22. Vroegop AV, Vanderveken OM, Boudewyns AN, et al. Drug-induced sleep endoscopy in sleep-disordered breathing: report on 1,249 cases. Laryngoscope. 2014;124(3):797-802.
23. Ryan CF, Love LL, Peat D, et al. Mandibular advancement oral appliance therapy for obstructive sleep apnea: effect on awake caliber of the velopharynx. Thorax. 1999;54(11):972-977.
24. Sutherland K, Deane SA, Chan ASL, et al. Comparative effects of two oral appliances on upper airway structure in obstructive sleep apnea. Sleep. 2011;34(4):469-477.
25. Turek G. A novel device for passive restraint of the tongue as an adjunct to mandibular advancement therapy in incomplete responders. J Dent Sleep Med. 2019;6(2).
26. Zeng B, Ng AT, Qian J, et al. Influence of nasal resistance on oral appliance treatment outcome in obstructive sleep apnea. Sleep. 2008;31
(4):543-547.
27. Michels Dde S, Rodrigues Ada M, Nakanishi M, et al. Nasal involvement in obstructive sleep apnea syndrome. Int J Otolaryngol. 2014;2014:717419.
28. Olmos SR. Nasal airway obstruction and orofacial pain: a multicenter retrospective analysis. Gen Dent. 2022;70(6):28-33.
29. Izci B, McDonald JP, Coleman EL, et al. Clinical audit of subjects with snoring and sleep apnoea/hypopnea syndrome fitted with mandibular repositioning splint. Respir Med. 2005;99(3):337-346.
30. Ishiyama H, Hasebe D, Sato K, et al. The efficacy of device designs (mono-block or bi-block) in oral appliance therapy for obstructive sleep apnea patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2019;16(17):3182.
31. Bishop B, Verrett R, Girvan T. A randomized crossover study comparing two mandibular repositioning appliances for treatment of obstructive sleep apnea. Sleep Breath. 2014;18(1):125-131.
32. Johal A, Agha B. Ready-made versus custom-made mandibular advancement appliances in obstructive sleep apnea: a systematic review and meta-analysis. J Sleep Res. 2018;27(6):e12660. doi: 10.1111/jsr.12660.
33. Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med. 2008;178(2):197-202.
34. Cruz JPP, Santos NCND, Pithon MM, de Morais Marcílio Cerqueira E. Biomonitoring of children and adolescents using orthodontic appliances made of acrylic resins through micronucleus testing of exfoliated buccal and palatal mucosa cells. Am J Orthod Dentofacial Orthop. 2021;160(2):193-199.
35. Nikolopoulou M, Ahlberg J, Visscher CM, et al. Effects of occlusal stabilization splints on obstructive sleep apnea: a randomized controlled trial. J Orofac Pain. 2013;27(3):199-205.
36. Gagnon Y, Mayer P, Morisson F, et al. Aggravation of respiratory disturbances by the use of an occlusal splint in apneic patients: a pilot study. Int J Prosthodont. 2004;17(4):447-453.
37. Nikolopoulou M, Naeije M, Aarab G, et al. The effect of raising the bite without mandibular protrusion on obstructive sleep apnoea. J Oral Rehabil. 2011;38(9):643-647.
38. Fritsch KM, Iseli A, Russi EW, Bloch KE. Side effects of mandibular advancement devices for sleep apnea treatment. Am J Respir and Crit Care Med. 2001;164(5):813-818.
39. Perez CV, de Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2013;17(1):323-332.
40. Marklund M. Subjective versus objective dental side effects from oral sleep apnea appliances. Sleep Breath. 2020;24(1):111-117.
41. Ng JH, Yow M. Oral appliances in the management of obstructive sleep apnea. Sleep Med Clin. 2020;15(2):241-250.
42. Minagi HO, Okuno K, Nohara K, Sakai T. Predictors of side effects with long-term oral appliance therapy for obstructive sleep apnea. J Clin Sleep Med. 2018;14(1):119-125.
43. Olmos SR. Comorbidities of chronic facial pain and obstructive sleep apnea. Curr Opin Pulm Med. 2016;22(6):570-575.
44. Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14(3):339-345.
45. Viviano J, Klauer D, Olmos S, Viviano JD. Retrospective comparison of the George Gauge™ registration and the sibilant phoneme registration for constructing OSA oral appliances. Cranio. 2022;40(1):5-13.
46. Singh GD, Olmos S. Use of a sibilant phoneme registration protocol to prevent upper airway collapse in patients with TMD. Sleep Breath. 2007;11(4):209-216.
47. Liu HW, Chen YJ, Lai YC, et al. Combining MAD and CPAP as an effective strategy for treating patients with severe sleep apnea intolerant to high-pressure PAP and unresponsive to MAD. PLoS One. 2017;12(10):e0187032.
48. Tanaka Y, Adame JM, Kaplan A, Almeida FR. The simultaneous use of positive airway pressure and oral appliance therapy with and without connector: a preliminary study. J Dent Sleep Med. 2022;9(2).