You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Edentulism is a chronic disease, and as the population of edentulous baby boomers continues to grow, so does the need for a variety of restorative options to meet the needs of these patients.1 Among the US geriatric population, an estimated 23 million individuals are completely edentulous, and 12 million are edentulous in one arch.2 Severe maxillary bone loss and atrophy can be caused by a variety of factors, including but not limited to advanced periodontal disease, terminal dentition conditions, surgical resection of a tumor, and trauma.3,4 The edentulous maxilla typically resorbs in a superior and posterior direction,5 resulting in a smaller osseous base that requires a volumetrically larger prosthesis to restore that patient's needs. Furthermore, the sinus tends to pneumatize, creating complex clinical situations, which are often treated with significant grafting procedures to develop a suitable osseous base to receive a group of implants and a fixed restoration.6
To Graft or Not to Graft
Deciding whether or not to graft is a key clinical treatment planning question. A number of research articles demonstrate the efficacy and high success rate grafting procedures.10-12 Sinus graft procedures and other full-arch grafts, such as a horseshoe-shaped graft from the autogenous ileum, have been used to reconstruct vertical, horizontal, and posterior defects.13 These grafting procedures have included autogenous bone as well as allogenic and xenograft bone and alloplasts.14-16 With these procedures, a significant amount of time is required for the grafted bone to integrate into the jaw and mature into a site that can receive implants. It is not uncommon to follow a 6-month bone graft integration phase with a 6-month implant integration phase.17 Therefore, these grafted cases require multiple surgeries, are associated with increased morbidity, and in almost all cases, result in more than a year of treatment. In addition to the time required for the surgical phase, the prosthetic phase of these cases is time-consuming and labor-intensive as well, and the removable prostheses that are worn during the healing period require significant adjustments. Although grafting approaches require significant time and procedures, they have been time-tested for advanced reconstruction.
Zygomatic and Pterygoid Implants
Alternatively, zygomatic and pterygoid implants have been considered in cases involving severe maxillary resorption. In 1988, Per-Ingvar Brånemark and his colleagues conceived of a "graftless solution" that involved using the patient's zygomatic bone to provide implant anchorage and stability for a fixed prosthesis.7 They successfully treated a series of patients, and after a decade of experimentation and follow-up, in 1998, they introduced an actual zygomatic implant fixture to the profession with clinical proof of its viability.7 This implant design was later modified and adjusted to include a 45° angle at the coronal head, which facilitated more optimal prosthetic positioning.8 In 2000, a modification of the intrasinus surgical technique as proposed by Brånemark and his team added a "sinus slot" to permit visualization of the lower surface of the zygomatic bone and to identify the entry point of the zygomatic implant.9 This slot concept was one of the first noted clinical improvements in the zygomatic implant protocol.
Multiple systematic reviews of zygomatic implants have shown that they have survival rates in the 96% to 99% range, even after a 12-year period.18-20 With a shift from the initial staged approach to immediate loading, patients can reach a final prosthetic restoration even sooner with a more minimally invasive and approach.21,22
Another option to facilitate implant placement in the posterior atrophic maxilla is the use of pterygoid implants. First described by Tulasne in 1989,23 implants placed in the pterygoid region are anchored to one or more anatomic structures, including the maxillary tuberosity, the pyramidal process of palatine bone, and the pterygoid process of the sphenoid bone,24 and can be used in conjunction with standard implants and/or zygomatic implants to deliver a full-arch prosthesis. Balshi, Wolfinger, and Balshi have presented several clinical reports as well as longitudinal studies in which both zygomatic and pterygoid implants demonstrated very high success rates and prosthesis stability.25,26
When treatment with zygomatic and pterygoid implants was still nascent, the highly skilled and trained oral and maxillofacial surgeons who were treating these cases were typically only providing them to patients with the most severely resorbed maxillae for whom all other options had been exhausted. More recently, however, zygomatic implants have become a more common treatment modality, and they have been utilized earlier in patients' dental journeys.27,28 Adding these implants can improve a prognosis in many ways. The advantages of zygomatic and pterygoid implants include better distribution and case stability,29 increased case composite torque value,30 improved anterior-posterior relationships,31 the elimination or significant reduction of cantilever length,32 and clinical opportunities as a revision implant(s) for failed cases.33 In addition, with the advent of cone-beam computed tomography (CBCT) and improved implant planning software, more precise positioning of implants in areas of minimal residual bone further optimized these techniques.34
Clinical Advances and Considerations
Malo and colleagues have published several significant review papers on zygomatic implants, including one that emphasized the "extramaxillary surgical technique."35 This paper documented the clinical outcomes of 352 patients who were rehabilitated with 747 zygomatic implants with follow-up of 6 months to 7 years. Earlier reports of zygomatic implant treatments from other clinicians, including Davo,36 Balshi,25,26 Bedrossian,37 and Aparacio,38,39 are noteworthy as well. These articles have demonstrated that zygomatic implants are a viable treatment alternative for the rehabilitation of a severely atrophic maxilla that results in reduced morbidity for the patient and a much shorter treatment time when compared with bone grafting and staged implant placement. Globally, immediate function with zygomatic implants is a growing trend. The impressive success rates of these implants are creating an appeal for their use in immediate loading protocols.
Improvements continue to be made, however, on Brånemark's initial technique in which the zygomatic implants were inserted internally from within the maxillary sinus. The external method or extramaxillary surgical technique, which was pioneered by Malo and others, entails the implants being placed externally either onto the maxillary sinus or laterally into the sinus cavity before anchoring into the zygomatic bone.35 The external or outer shaft of the implant may only be covered by soft tissue. Regarding placement, the "channel osteotomy" performed is basically connecting two points: the crest and the entry point into the zygoma.40 This channel facilitates the optimal path for the zygomatic implant into the buttress of the zygoma bone.
The apices of zygomatic implants have been modified by manufacturers in terms of the apical shape, thread pattern, and self-cutting features. Beyond modifications to specific aspects of the apical portion and surface treatments, other novel changes to the design of zygomatic implants from various manufacturers have included making the shaft of the implant a smooth machined surface that is more hospitable for the covering soft tissues,41 adding a 45° angle to the coronal aspect with an external hex being tilted into the implant design,42 and adding a 55° offset.43 Offsets at the coronal aspect of zygomatic implants are intended to allow for more ideal positioning of the screw access holes in the prostheses. This is a major prosthetic improvement on the earlier intrasinus techniques of the Brånemark group, whose prostheses often had screw access holes angling toward the palate, which interfered with patient comfort, oral hygiene, and speech.
In the early studies utilizing the original intrasinus protocol, it was suggested that these treatments be performed under general anesthesia.44 However, for the extramaxillary approach, many published clinicians have successfully and comfortably executed cases under intravenous or oral sedation coupled with local anesthesia.45,46 The anesthetic regimen utilized should be determined by the needs of the patient in each individual case.
For zygomatic implant cases, the postoperative surgical results are similar to those of most advanced and large conventional implant cases. The most frequent postoperative complications associated with the placement of zygomatic implants include rhinitis, sinusitis, paresthesia, and oroantral fistula.44 The mechanical complications in zygomatic cases are also similar to those of conventional implant full-arch cases; however, the literature reflects that very few of these result in a total failure of the prosthesis.47 Examples of mechanical complications associated with zygomatic implants include loose prosthetic components, chipped or broken prosthetic teeth, and occasionally, a frame fracture of the prosthesis.33 According to the results of one study of zygomatic implants, one third of the mechanical complications that occurred were in patients who had a preclinical diagnosis of bruxism.33 For these patients, consideration of the opposing dentition is essential, and delivery of a night guard is highly recommended.
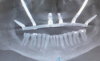
Treatment options for full-arch restorations include the placement of conventional implants in the anterior region accompanied by single zygomatic implants in the posterior left and right (Figure 1),48 the classic "quad zygoma" concept with four zygomatic implants in position (Figure 2),19,49 and the pterygoid fixated arch stabilization technique, which combines two anterior conventional implants, two zygomatic implants, and two pterygoid implants (Figure 3).50 Treatment plans can now be customized to optimize the implant positions based on each patient's anatomy and needs.
When placing zygomatic implants, it is crucial that clinicians always observe where the orbit is and ensure that the entry into the zygoma is of sufficient depth to result in a buccal plate that is thick enough to not fracture or resorb over time. In addition, when planning and delivering quadruple zygoma placements, clinicians must be mindful that there is sufficient bone to prevent "clashing" of the implants at their apices.
Education and Training
Placing zygomatic and pterygoid implants requires clinical knowledge that transcends what is taught about implants in most dental schools. A detailed knowledge of the related anatomy and a complete understanding of both the surgical protocols and the various treatment planning considerations is necessary.
So, where can clinicians who have decided that they might want to add these clinical treatments to their patient offerings acquire the necessary education and training, and what should the training path be? Initially, online resources can be helpful. There are many YouTube videos and recordings of webinars available from global educators. Next, clinicians should consider courses in which various models are used in order to learn the positioning and angulation of the implants and handpiece (Figure 4). Proper angulation is critical for the positioning of both zygomatic and pterygoid implants. When clinicians are ready for hands-on training, they should seek out courses involving human cadavers, which include needed anatomy and treatment planning didactics, model workshops, and intensive, interactive, supervised cadaver workshops. Although these courses have trained many very interested and talented clinicians to place these implants, anecdotally, as many as half of the initial placements performed by students require either a subtle or major reorientation in positioning. Therefore, the need for hands-on training prior to treating patients cannot be overemphasized.
The final portion of the journey is the "live patient experience," which involves the supervised placement of implants in live patients. Several clinics offer this type of training. A critical component of the success of these teaching groups is that they have prosthetically trained dentists who can handle postsurgical issues as well as the rehabilitation of cases performed by the participants. Ethical patient treatment and postoperative care are required for training.
Promising Growth
Systematic reviews analyzing the survival of pterygoid implants have shown promising data, but additional research is needed to further improve placement protocols.51,52 The zygoma anatomy-guided approach, which analyzes the anatomy of a patient's maxilla to guide a prosthetically driven minimally invasive zygomatic osteotomy, has shown magnificent results.53 In the zygoma anatomy-guided approach, for certain anatomies, the implant placement is totally external to the buccal aspect of the sinus, whereas for other anatomies, the implant is required to be placed within buccal plate and then within the sinus. Special surgical instruments and drills have been developed to facilitate these approaches.
Due to the need for precision and to overcome anatomic challenges, the incorporation of a guided approach appears to be a growing trend. Other advances in the digital aspects of case delivery, including those in the areas of design software, intraoral scanning, programetry, and facial analysis, are contributing to the growth of treatment with zygomatic and pterygoid implants as well (Figure 5 and Figure 6).
Many clinicians have made adjustments and changes to their treatment planning because a larger percentage of their cases are patients who present with terminal dentition as opposed to those who are totally edentulous. During the preoperative screening, the clinician can often visualize and demonstrate that when the teeth are removed, a minimal amount of bone may remain in zones 1 and 2 of the maxilla,54 creating the need for additional posterior support, including the utilization of the bone of the zygomatic and pterygoid areas.
The use of zygomatic and pterygoid implants is growing rapidly. The extramaxillary approach and the availability of educational opportunities seem to be driving this growth. Considering the overall success rates, with the advances in CAD and the integration of 3D printing technologies, coupled with the advances in guided surgery and guided prosthetics, treatment with zygomatic and pterygoid implants is becoming as exciting as treatment with conventional implants.
Queries regarding this course may be submitted to authorqueries@aegiscomm.com
About the Author
Jack T. Krauser, DMD
Fellow
Academy of Osseointegration
Diplomate
International Congress of Oral Implantologists
Private Practice
North Palm Beach, Florida
References
1. Syrop J. Preparing your business for the boomer generation. Inside Dentistry. 2010;10(9):114-121.
2. Facts & Figures. American College of Prosthodontists website. https://www.gotoapro.org/facts-figures/. Accessed April 8, 2022.
3. Baj A, Trapella G, Lauritano D, et al. An overview on bone reconstruction of atrophic maxilla: success parameters and critical issues. J Biol Regul Homeost Agents. 2016;30(2 Suppl 1):209-215.
4. Salvatori P, Mincione A, Rizzi L, et al. Maxillary resection for cancer, zygomatic implants insertion, and palatal repair as single-stage procedure: report of three cases. Maxillofac Plast Reconstr Surg. 2017;39(1):13.
5. Foundation for Oral Rehabilitation. Skeletal consequences of edentulism. FOR website. https://www.for.org/en/treat/treatment-guidelines/
edentulous/diagnostics/clinical-findings/skeletal-consequences-edentulism. Accessed April 8, 2022.
6. Crivellaro VR, Zielak JC, Deliberador TM, et al. Pneumatization within a maxillary sinus graft: a case report. Int J Implant Dent. 2016;2(1):3.
7. Brånemark PI, Gröndahl K, Worthington P. Osseointegration and Autogenous Onlay Bone Grafts: Reconstruction of the Edentulous Atrophic Maxilla. Quintessence Publishing Co, Inc; 2001:112-134.
8. Aparicio C, Manresa C, Francisco K, et al. The long-term use of zygomatic implants: a 10-year clinical and radiographic report. Clin Implant Dent Relat Res. 2014;16(3):447-459.
9. Stella JP, Warner MR. Sinus slot technique for simplification and improved orientation of zygomaticus dental implants: a technical note. Int J Oral Maxillofac Implants. 2000;15(6):889-893.
10. Yun KI, Choi H, Wright RF, et al. Efficacy of alveolar vertical distraction osteogenesis and autogenous bone grafting for dental implants: systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2016;31(1):26-36.
11. Altiparmak N, Akdeniz SS, Diker N, et al. Comparison of success rate of dental implants placed in autogenous bone graft regenerated areas and pristine bone. J Craniofac Surg. 2020;31(6):1572-1577.
12. Torres Y, Raoul G, Lauwers L, Ferri J. The use of onlay bone grafting for implant restoration in the extremely atrophic anterior maxilla. A case series. Swiss Dent J. 2019;129(4):274-285.
13. Kahnberg KE, Nystrom E, Bartholdsson L. Combined use of bone grafts and Brånemark fixtures in the treatment of severely resorbed maxillae. Int J Oral Maxillofac Implants. 1989;4(4):297-304.
14. Olson JW, Dent CD, Morris HF, Ochi S. Long-term assessment (5 to 71 months) of endosseous dental implants placed in the augmented maxillary sinus. Ann Periodontol. 2000;5(1):152-156.
15. Hallman M. On healing of titanium implants in xenografts. Thesis, University of Umeå, Sweden; 2002.
16. Szabó G, Huys L, Coulthard P, et al. A prospective multicenter randomized clinical trial of autogenous bone versus beta-tricalcium phosphate graft alone for bilateral sinus elevation: histologic and histomorphometric evaluation. Int J Oral Maxillofac Implants. 2005;20(3):371-381.
17. Spin-Neto R, Stavropoulos A, Coletti FL, et al. Graft incorporation and implant osseointegration following the use of autologous and fresh-frozen allogeneic block bone grafts for lateral ridge augmentation. Clin Oral Implants Res. 2014;25(2):226-233.
18. Maló P, de Araújo Nobre M, Lopes A, et al. Five-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded zygomatic implants placed extra-maxillary. Eur J Oral Implantol. 2014;7(3):267-281.
19. Lan K, Wang F, Huang W,et al. Quad zygomatic implants: a systematic review and meta-analysis on survival and complications. Int J Oral Maxillofac Implants. 2021;36(1):21-29.
20. Chrcanovic BR, Abreu MHNG. Survival and complications of zygomatic implants: a systematic review. Oral Maxillofac Surg. 2013;17(2):81-93.
21. Agliardi EL, Romeo D, Panigatti S, et al. Immediate full-arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: a prospective clinical study with minimum follow-up of 6 years. Int J Oral Maxillofac Surg. 2017;46(12):1592-1599.
22. Mozzati M, Monfrin SB, Pedretti G, et al. Immediate loading of maxillary fixed prostheses retained by zygomatic and conventional implants: 24-month preliminary data for a series of clinical case reports. Int J Oral Maxillofac Implants. 2008;23(2):308-314.
23. Tulasne JF. Implant treatment of missing posterior dentition. In: Albrektsson T, Zarb GA, eds. The Branemark Osseointegrated Implant. Quintessence; 1989:103.
24. Reiser GM. Implant use in the tuberosity, pterygoid, and palatine region: anatomic and surgical considerations. In: Nevins M, Mellonig JT, eds. Implant Therapy: Clinical Approaches and Evidence of Success. Vol 2. Quintessence; 1998:197.
25. Balshi SF, Wolfinger GJ, Balshi TJ. A retrospective analysis of 110 zygomatic implants in a single-stage immediate loading protocol. Int J Oral Maxillofac Implants. 2009;24(2):335-341.
26. Balshi TJ, Wolfinger GJ, Balshi SF. Analysis of 356 pterygomaxillary implants in edentulous arches for fixed prosthesis anchorage. Int J Oral Maxillofac Implants. 1999;14(3):398-406.
27. Rosenstein J, Dym H. Zygomatic implants: a solution for the atrophic maxilla: 2021 update. Dent Clin North Am. 2021;65(1):229-239.
28. Ramezanzade S, Yates J, Tuminelli FJ, et al. Zygomatic implants placed in atrophic maxilla: an overview of current systematic reviews and meta-analysis. Maxillofac Plast Reconstr Surg. 2021;43(1):1.
29. Korkmaz FM, Korkmaz YT, Yaluğ S, Korkmaz T. Impact of dental and zygomatic implants on stress distribution in maxillary defects: a 3-dimensional finite element analysis study. J Oral Implantol. 2012;38(5):557-567.
30. Salvatori P, Mincione A, Rizzi L, et al. Maxillary resection for cancer, zygomatic implants insertion, and palatal repair as single-stage procedure: report of three cases. Maxillofac Plast Reconstr Surg. 2017;39(1):13.
31. Fortin Y. Placement of zygomatic implants into the malar prominence of the maxillary bone for apical fixation: a clinical report of 5 to 13 years. Int J Oral Maxillofac Implants. 2017;32(3):633-641.
32. Almeida PHT, Cacciacane SH, França FMG. Stresses generated by two zygomatic implant placement techniques associated with conventional inclined anterior implants. Ann Med Surg (Lond). 2018;30:22-27.
33. Gunaseelan R, Saravanakumar M, Hariharan R. Restoration of failing maxillary implant-supported fixed prosthesis with cross arch splinted unilateral zygomatic implant: a clinical report. J Oral Implantol. 2012;38(6):751-755.
34. Rinaldi M, Ganz SD. Computer-guided approach for placement of zygomatic implants: novel protocol and surgical guide. Compend Contin Educ Dent. 2019;40(6):368-385.
35. Maló P, de Araújo Nobre M, Lopes A, et al. Extramaxillary surgical technique: clinical outcome of 352 patients rehabilitated with 747 zygomatic implants with a follow-up between 6 months and 7 years. Clin Implant Dent Relat Res. 2015;17(Suppl 1):e153-e162.
36. Davó R, Malevez C, Rojas J, et al. Clinical outcome of 42 patients treated with 81 immediately loaded zygomatic implants: a 12- to 42-month retrospective study. Eur J Oral Implantol. 2008;1(2):141-150.
37. Bedrossian E. Rehabilitation of the edentulous maxilla with the zygoma concept: a 7-year prospective study. Int J Oral Maxillofac Implants. 2010;25(6):1213-1221.
38. Aparicio C, Ouazzani W, Garcia R, et al. A prospective clinical study on titanium implants in the zygomatic arch for prosthetic rehabilitation of the atrophic edentulous maxilla with a follow-up of 6 months to 5 years. Clin Implant Dent Relat Res. 2006;8(3):114-122.
39. Aparicio C, Ouazzani W, Aparicio A, et al. Immediate/early loading of zygomatic implants: clinical experiences after 2 to 5 years of follow-up. Clin Implant Dent Relat Res. 2010;12(Suppl 1):e77-e82.
40. Aparicio C, Polido WD, Zarrinkelk HM. The zygoma anatomy-guided approach for placement of zygomatic implants. Atlas Oral Maxillofac Surg Clin North Am. 2021;29(2):203-231.
41. Holtzclaw D. Treatment of the severely atrophic arch with zygomatic, pterygoid, and vomer dental implants. Noris Medical website. https://www.norismedical.com/academy/clinical-cases-2/treatment-of-the-severely-atrophic-arch-with-zygomatic-pterygoid-and-vomer-dental-implants/. Accessed April 11, 2022.
42. Malo P. NobelZygoma™ - dramatically shortens time-to-teeth. Nobel Biocare website. https://www.nobelbiocare.com/blog/products-and-solutions/
nobelzygoma-dramatically-shortens-time-to-teeth/. Published March 21, 2018. Accessed April 11, 2022.
43. Zygomatic and oncology dental implants. Southern Implants website. https://southernimplants.com/solutions/innovative-products/zygomatic-implants/. Accessed April 11, 2022.
44. Grecchi F, Bianchi AE, Siervo S, et al. A new surgical and technical approach in zygomatic implantology. Oral Implantol (Rome). 2017;10(2):197-208.
45. Blanc O, Shilo D, Weitman E, et al. Extramaxillary zygomatic implants: an alternative approach for the reconstruction of the atrophic maxilla. Ann Maxillofac Surg. 2020;10(1):127-132.
46. Almeida PHT, Salvoni AD, França FMG. Evaluation of satisfaction of individuals rehabilitated with zygomatic implants as regards anesthetic and sedative procedure: a prospective cohort study. Ann Med Surg (Lond). 2017;22:22-29.
47. Tzerbos F, Bountaniotis F, Theologie-Lygidakis N, et al. Complications of zygomatic implants: our clinical experience with 4 cases. Acta Stomatol Croat. 2016;50(3):251-257.
48. Ugurlu F, Yıldız C, Sener BC, Sertgoz A. Rehabilitation of posterior maxilla with zygomatic and dental implant after tumor resection: a case report. Case Rep Dent. 2013;2013:930345.
49. Davó R, David L. Quad zygoma: technique and realities. Oral Maxillofac Surg Clin North Am. 2019;31(2):285-297.
50. Holtzclaw D, Telles R. Pterygoid fixated arch stabilization technique (PFAST): a retrospective study of pterygoid dental implants used for immediately loaded full arch prosthetics. J Implant Adv Clin Dent. 2018;10(7):6-17.
51. Bidra AS, Huynh-Ba G. Implants in the pterygoid region: a systematic review of the literature. Int J Oral Maxillofac Surg. 2011;40(8):773-781.
52. Graves SL. The pterygoid plate implant: a solution for restoring the posterior maxilla. Int J Periodontics Restorative Dent. 1994;14(6):512-523.
53. Aparicio C, Olivo A, de Paz V, et al. The zygoma anatomy-guided approach (ZAGA) for rehabilitation of the atrophic maxilla. Clinical Dentistry Reviewed. 2022;6:2.
54. Bedrossian E, Bedrossian EA. Zygomatic implant redesigned: rationale and biomechanical principles. Compend Contin Educ Dent. 2021;42(1):SSS1-SSS4.