You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
For successful restoration of the edentulous maxilla, consideration must be given to esthetics, phonetics, function, and anatomical limitations, while procedures should provide long-term stability and not compromise other intraoral structures.1,2 To achieve these goals, implant-supported restorations that are prosthetically driven and biologically executed are optimal for many patients. To attain such a restoration, a comprehensive, multidisciplinary approach is required that considers all available options, weighs patient desires, and contemplates anticipated outcomes associated with various treatment approaches.3
Tooth loss is associated with significant volumetric changes in the supporting alveolar bone.4 Complete tooth loss and use of removable prostheses without implant placement, particularly over an extended period, can result in initial rapid bone loss followed by continued atrophy over time.5 Additionally, in cases of complete maxillary edentulism, changes in jaw relationships, esthetic limitations related to lost structures, supra-eruption of remaining mandibular teeth, and alterations of facial musculature may lead to occlusal dysfunction and morphologic changes that must be addressed in any rehabilitation.6
When considering implant rehabilitation in the edentulous maxilla, overall prosthetic design is driven by several oral findings, including lip support, transition line position, and prosthetic space.7,8 These factors must also be considered in light of underlying anatomical structures, including those structures that should be avoided, existing bone volume, and whether or not necessary tissue reduction can be performed to achieve a particular restorative option without creating esthetic or functional problems.7,8 Comprehensive assessment of all patients requiring prosthetic reconstruction of an edentulous maxilla is necessary to provide clinicians with adequate data to develop a treatment plan that addresses the patient's esthetic, functional, physiologic, psychologic, financial, and timing goals. This article describes a systematic approach to decision-making in patients with an edentulous maxilla seeking implant reconstruction and presents a decision matrix to facilitate the step-by-step diagnostic processes.
Treatment Planning Considerations
A systematic approach to initial treatment planning of a patient seeking implant reconstruction in the edentulous maxilla is suggested. After review of medical and dental history and an overall evaluation of any remaining teeth, an initial assessment should include fabrication of an accurate denture or wax trial denture (denture duplicate) (Figure 1). In a patient with an edentulous maxilla seeking implant reconstruction, this denture fabrication plays an important role in the treatment planning process where both intraoral and extraoral data can be collected. A well-designed denture incorporates phonetic, anatomic, esthetic, and functional considerations, which are essential for successful therapy. This denture will provide information regarding three major variables-restorative space, lip support, and transition line-that aid in the decision regarding the final prosthesis and implant planning. Well-designed denture fabrication is also necessary to provide a guide to accurately capture radiographic data with proper jaw relationships and validate measures clinically and radiographically.
Assessment of Prosthetic Space
Alveolar bone resorption has a significant impact on prosthesis design. The severity of alveolar defects associated with edentulism can range from a tooth-only defect, in which only teeth are missing, to a composite defect, which consists of missing teeth along with soft- and hard-tissue resorption.9 Having an accurate denture and/or duplicate allows the practitioner to establish the type of defect by assessing acrylic thickness apical to the denture teeth. If there is a minimal amount of acrylic apical to the teeth, this indicates a tooth-only defect. If, however, acrylic thickness apical to the teeth is increased to achieve adequate seal, a composite defect is likely present, and the acrylic is accounting for the loss of soft and hard tissue.
The denture fabrication also allows for the calculation of sink depth. Sink depth describes the distance from the implant surface (platform) to the gingival margin10; the distance from the implant surface to the occlusal surface of the prosthesis represents a summation of the sink depth and the prosthetic space. The sink depth can be measured clinically by bone sounding and should be considered in cases where it is anticipated that soft-tissue thickness will be increased (eg, through soft-tissue grafting procedures) and in cases where a lack of prosthetic space is anticipated, necessitating a reduction in gingival or bone height. As noted by Avrampou et al, the space between the implant platform and the occlusal surfaces must accommodate teeth and adequate thickness of prosthetic materials.11 Based on the types of resorptive defect(s) present and the amount of ridge atrophy associated with complete edentulism in the maxilla, a patient may be a candidate for implant-supported fixed prostheses without other grafting procedures.
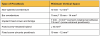
Prosthetic space should also be assessed prior to implant placement. Lack of adequate prosthetic space can lead to increased rate of prosthetic failure due to weak prosthetic substructure. Additionally, lack of prosthetic space may lead to poor physiological contours of the prostheses, reduced interocclusal restorative space, lack of access for oral hygiene procedures, and poor esthetics.12 The prosthetic space is defined as the vertical distance from the soft tissue of the edentulous ridge to the occlusal surface of the opposing dentition (in an ideal occlusal relationship) (Figure 2).11 This space must accommodate the bulk of the restorative materials and abutments/attachments and also allow for a prosthetic design that facilitates esthetics, phonetics, and proper hygiene measures. Different types of restorations require varying space requirements, which must be considered during the treatment planning phase (Table 1).13-17 Accurately mounted casts are critical when measuring the prosthetic space available. This space can be measured through several methods:
A periodontal probe or millimeter ruler may be used on mounted casts (Figure 3).
Radiographic measurements may be taken after capture of a CBCT image of both the patient and prosthesis using a dual-scan protocol and imaging software. Measurements are taken from the intaglio surface of the denture to the occlusal surface utilizing fiduciary markers to align the prosthesis (Figure 4 and Figure 5).
Measurements may be made directly on the denture prosthesis using a gauge to measure the distance from the intaglio surface of the denture to the occlusal surface of the teeth (Figure 6).
While these techniques allow for measurement of prosthetic space, they are contingent upon the accurate fabrication of transitional dentures and the accurate positioning of the dental arches in appropriate occlusal relationships.
In cases where prosthetic space is limited and the patient requires additional restorative space to accommodate the thickness of the planned prosthesis, the practitioner must determine whether additional prosthetic space can be achieved through alveoloplasty or if altering the planned prosthesis is preferable to the patient. A rational, step-by-step approach should be taken to determine the optimal prosthesis that includes assessment of the existing space and an objective review of the risks and benefits of alveoloplasty and other prosthetic options.
Alveoloplasty: Available prosthetic space can be directly increased through bone removal from the alveolar crest. In this manner, alveoloplasty may be used alone or in combination with other modalities to gain sufficient prosthetic space.18 When determining the feasibility of alveoloplasty, the dental team must consider the potential remaining bone after adequate prosthetic space is achieved. If bone removal required to achieve necessary prosthetic space would compromise implant placement, underlying anatomical structures, or ideal interocclusal relationships, other treatment options should be considered. In cases with severe space limitations, alveoloplasty may be employed with other bone grafting procedures, such as sinus augmentation or lateral ridge augmentation, to improve residual bone volume or position for ideal implant placement.
Alveoloplasty affords control of bone removal to ensure adequate prosthetic space gain without affecting phonetics, esthetics, or vertical dimension after placement of the prosthesis and provides increased ridge width.17 Drawbacks of alveoloplasty, however, include the potential over-reduction of the alveolus, minimal residual keratinized tissue, and/or loss of cortical plate postoperatively. Furthermore, alveoloplasty may result in a clinical situation in which there is no retreat for the practitioner if bone loss due to peri-implantitis occurs and implants must be replaced. Retrievability and long-term outcome must be considered if alveoloplasty is employed.
Increasing vertical dimension: The Glossary of Prosthodontic Terms defines vertical dimension as the distance between two selected anatomic points.19 When the mandibular teeth are occluding with the maxillary teeth, the vertical dimension is defined as the vertical dimension of occlusion (VDO). In cases of occlusal wear or long-standing loss of posterior support, increasing the VDO prior to implant placement may be advantageous. Increasing VDO through altering the prosthesis in the maxilla has been reported to be more challenging versus the mandible, which may make this a more suitable option in cases of complete edentulism requiring restoration.20 Increasing patient VDO outside of that which is diagnostically optimal, particularly in the maxilla, can lead to significant esthetic compromises, speech alterations, neuromuscular symptoms, and/or patient discomfort. An incremental approach to gradually increasing VDO in these cases is advised.21,22
Reducing soft-tissue thickness: In cases of excessive sink depth, ie, distance from the implant platform to the gingival margin, subsequent thinning of soft-tissue volume, while maintaining an adequate zone of keratinized tissue, should be considered, especially in cases with severely limited prosthetic space and significant thickness of overlying soft tissues. One notable rationale for soft-tissue reduction is availability of attachments of sufficient height. That is, if sink depth is high, an increased height of prosthetic attachments or abutments may be required. If such abutment heights are unavailable, the thinning of soft tissue in cases with excessive soft-tissue volume could allow for the use of shorter implant attachments, which, in turn, will increase available prosthetic space. Use of this technique alone may be appropriate only where a minimal gain of prosthetic space is needed and is dependent on the thickness of the existing soft tissue.
Assessment of Facial and Lip Support
Lip support is critical to overall esthetics, but as alveolar bone is lost after tooth extraction, buccal resorption in the premaxilla can lead to significant deficiencies in lip support that compromise prosthetic outcomes. In addition to the teeth, the underlying soft tissues of the lips, ie, musculature, salivary and sebaceous glands, and connective tissue, and hard tissues of the alveolar ridge and anterior teeth combine to provide lip support.23 Tooth extraction and the resultant ridge resorption may result in a relative retruded position of the anterior maxilla,24 which can cause significant facial collapse and alteration of overall facial contours.
Although patients tend to prefer fixed prostheses over removable ones, facial support is an important factor that may determine the relative advantages of utilizing a removable prosthesis over a fixed one. Facial support can be created or supported by the buccal flange of a denture (Figure 7).25,26 This support can be assessed by inserting the denture and/or duplicate in place with and without a flange. This allows for visualization by the patient and practitioner of the resultant esthetics in a removable or fixed prosthesis. Evaluation of lip support in this manner should be performed with lips at rest and in function and assessed in both frontal and profile views. If lip support is adequate without the flange in place, a fixed prosthesis may be used; however, if lip support without the flange in place is deemed unacceptable, the addition of a flange with a removable prosthesis may be optimal (Figure 8 and Figure 9). Involving the patient in this evaluation and providing visual evidence of the lip support that could be lost as a limitation of a fixed prosthetic option is crucial to providing necessary informed consent for reconstruction of the edentulous maxilla.
Determination of the Position of the Transition and Smile Lines
The transition line refers to the line that is formed between the implant-supported prosthesis and the residual soft-tissue crest (Figure 10). The smile line is the dynamic position of the upper lip in full smile and the resultant visibility of the residual ridge and should be evaluated during speech and smiling. To evaluate these two factors, the patient is asked to smile without his or her denture in place. This allows for an evaluation of the relationship between the transition line and smile line, which can serve to determine the best type of prosthesis for the individual patient. The visibility of the residual ridge can be classified into three categories: hidden, partially visible, and visible (Figure 11 through Figure 13).
If the transition line is apical to the smile line, and the residual ridge is hidden, any type of prosthesis may be suitable. If the residual ridge is partially or completely visible, ie, the smile line is apical to the transition line, a hybrid prosthesis is a high esthetic risk unless the transition or smile line can be altered. If the transition line is visible, reduction of the residual ridge to displace the transition line apical to the smile line may be considered. However, if this reduction will compromise the amount of bone height required to place implants or will violate any anatomical structures, either a fixed crown-and-bridge prosthesis or a removable overdenture should be used.
Comprehensive Patient Assessment
All three parameters discussed-prosthetic space, lip support, and transition line-should be evaluated in combination to determine the best prosthetic option for each case using a comprehensive, systematic, clinical approach. Each parameter plays an important role. For example, if lip support is needed based on the appropriate clinical evaluation, practitioners should utilize a removable prosthesis to maximize esthetics and phonetics. Also, in cases where the transition line is visible or prosthetic space is limited, alveoloplasty may be considered. In such cases, however, if alveoloplasty might compromise implant placement, a fixed crown-and-bridge or removable prosthesis is recommended. Other parameters such as bone quantity, patient finances, and systemic health are additional factors for both the patient and practitioner to consider in determining the optimum course of treatment.
Discussion
Dental implants enable the delivery of stable, implant-supported restorations that are capable of reducing ongoing bony resorption and restoring oral function, esthetics, phonetics, and facial contours in fully edentulous patients. In patients who have lost all of their maxillary teeth, morphology, musculature, alveolar bone support, and other determinants of facial esthetics become altered, and continued resorption and atrophy of tissues may occur post-extraction. Given the volumetric and maxillomandibular relationship changes that occur over time after tooth extraction and the numerous conditions that can lead to the need for tooth extraction, variability exists among individuals seeking full-arch maxillary implant-supported restorations, and this variability can influence which restorative option is best. These myriad influences that can affect patient outcomes dictate that careful treatment planning prior to implant placement and prosthetic design be carried out so that lost and/or altered structures to be restored in a final prosthesis can be evaluated to ensure patient comfort, function, and esthetics.
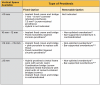
Numerous types of prostheses may be useful in maxillary full-arch restoration, including implant-supported fixed, removable, and hybrid protheses. Determining the ideal treatment modality requires systematic data acquisition and utilization of clinical, radiographic, photographic, and functional findings to develop a treatment plan to best meet individual patient needs. The use of prosthetic, functional, and radiographic data combined with 3D computerized modeling may provide an advantage when selecting viable treatment options. Critical decision-making regarding prosthetic options requires assessment of key factors that influence the optimal treatment modalities for individual patients. These include: (1) assessment of existing prosthetic space, (2) determination of the feasibility of altering the prosthetic space, if necessary, (3) assessment of facial and lip support, and (4) determination of the position of transition and smile lines. Careful, comprehensive examination allows for assessment of the best options for individual patients based on the available prosthetic space (Table 2).13-17
Bedrossian et al established a systematic treatment planning protocol to address implant therapies in the fully edentulous maxilla.7,9 This protocol was based on three variables: presence or absence of composite defect, visibility of the residual ridge crest, and radiographic evaluation of bone quantity, quality, and position. While these variables are critical to overall success, they do not consider lip support and its importance in the determination of final prosthesis design. While previous authors have highlighted the variables discussed here, it is important to review specific techniques to best evaluate each variable, to discuss their weight in decision-making, and to assess opportunities to potentially manage each parameter.
It should also be noted that these clinical and radiographic findings should be combined with a patient-level assessment of expectations (eg, timeline, financial situation, prosthetic preferences), systemic health conditions, existing oral diseases, risk factors, and medical/dental history. When the team is restoring a patient with an edentulous maxilla with a full-arch dental implant-supported prosthesis, a holistic approach that considers all of these factors should be taken.
Conclusion
The principles presented here are intended to offer a comprehensive diagnostic approach that assesses three prosthetic parameters to help identify appropriate prosthetic solutions that suit each patient and aid in planning for full-arch implant treatment. These parameters can only be assessed if appropriate therapeutic diagnostic techniques, including the use of proper radiographic studies, articulator-mounted models, and other diagnostic tests, are performed. While other patient-centered factors should also be considered regarding the optimal final prosthesis, the decision-making processes presented here allow for a reliable diagnosis that can prevent significant errors that may compromise both function and esthetics.
About the Authors
Hussein S. Basma, DDS, DESS, MS
Assistant Professor, Department of Periodontology, University of Alabama at Birmingham School of Dentistry
Birmingham, AL
Nicolaas C. Geurs DDS, MS
Weatherford-Palcanis Endowed Professor and Chair, Department of Periodontology, University of Alabama at Birmingham School of Dentistry
Birmingham, AL
Maria L. Geisinger DDS, MS
Professor, Department of Periodontology, University of Alabama at Birmingham School of Dentistry
Birmingham, AL
References
1. Schnitman PA. The profile prosthesis: an aesthetic fixed implant-supported restoration for the resorbed maxilla. Pract Periodontics Aesthet Dent. 1999;11(1):143-151.
2. Zitzmann NU, Marinello CP. Fixed or removable implant-supported restorations in the edentulous maxilla: literature review. Pract Periodontics Aesthet Dent. 2000;12(6):599-608.
3. Desjardins RP. Prosthesis design for osseointegrated implants in the edentulous maxilla. Int J Oral Maxillofac Implants. 1992;7(3):311-320.
4. Van der Weijden F, Dell'Acqua F, Slot DE. Alveolar bone dimensional change of post-extraction sockets in humans: a systematic review. J Clin Periodontol. 2009;36(12):1048-1058.
5. Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: a mixed-longitudinal study covering 25 years. J Prosthet Dent. 2003;89(5):427-435.
6. Cawood JI, Howell RA. Reconstructive preprosthetic surgery. I. Anatomical considerations. Int J Oral Maxillofac Surg. 1991;20(2):75-82.
7. Bedrossian E, Sullivan RM, Fortin Y, et al. Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method. J Oral Maxillofac Surg. 2008;66(1):112-122.
8. Jivraj S, Chee W, Corrado P. Treatment planning of the edentulous maxilla. Br Dent J. 2006;20(5):261-279.
9. Bedrossian E, Bedrossian EA. Systematic treatment planning protocol of the edentulous maxilla for an implant-supported fixed prosthesis. Compend Contin Educ Dent. 2009;40(1):20-25.
10. Carpentieri J, Greenstein G, Cavallaro J. Hierarchy of restorative space required for different types of dental implant prostheses. J Am Dent Assoc. 2019;150(8):695-706.
11. Avrampou M, Mericske-Stern R, Blatz MB, Katsoulis J. Virtual implant planning in the edentulous maxilla: criteria for decision making of prosthesis design. Clin Oral Implants Res. 2013;24(suppl A100):152-159.
12. Chaimattayompol N, Arbree NS. Assessing the space limitation inside a complete denture for implant attachments. J Prosthet Dent. 2003;89(1):82-85.
13. Sadowsky SJ. Treatment considerations for maxillary implant overdentures: a systematic review. J Prosthet Dent. 2007;97(6):340-348.
14. Carpentieri J, Drago C. Treatment of edentulous and partially edentulous maxillae: clinical guidelines. J Implant Reconstr Dent. 2011;3(1):7-17.
15. Kendrick S, Wong D. Vertical and horizontal dimensions of implant dentistry: numbers every dentist should know. Inside Dentistry. 2009; 5(7):32-38.
16. Biomet 3i Restorative Manual. Palm Beach Gardens, FL: Biomet 3i. http://www.zimmerbiomet.co.il/filesystem/INSTRM_REV+E_Restorative+Manual_Final_SECURED.pdf. Accessed January 20, 2021.
17. Ahuja S, Cagna DR. Classification and management of restorative space in edentulous implant overdenture patients. J Prosthet Dent. 2011;105(5):332-337.
18. Lee CK, Agar JR. Surgical and prosthetic planning for a two-implant-retained mandibular overdenture: a clinical report. J Prosthet Dent. 2006; 95(2):102-105.
19. The glossary of prosthodontic terms: ninth edition. J Prosthet Dent. 2017;117(5S):e1-e105.
20. Massad JJ, Connelly ME, Rudd KD, Cagna DR. Occlusal device for diagnostic evaluation of maxillomandibular relationships in edentulous patients: a clinical technique. J Prosthet Dent. 2004;91(6):586-590.
21. Hansen CA. Diagnostically restoring a reduced occlusal vertical dimension without permanently altering the existing dentures. J Prosthet Dent. 1985;54(5):671-673.
22. Jeganathan S, Payne JA. Common faults in complete dentures: a review. Quintessence Int. 1993;24(7):483-487.
23. Martone AL. Effects of complete dentures on facial esthetics. J Prosthet Dent. 1964;14(2):231-255.
24. Tallgren A. The reduction in face height of edentulous and partially edentulous subjects during long-term denture wear. A longitudinal roentgenographic cephalometric study. Acta Odontol Scand. 1966;24(2):195-239.
25. Bidra AS, Zapata G, Agar JR, et al. Differences in lip support with and without labial flanges in a maxillary edentulous population. Part 1: Objective analysis. J Prosthodont. 2018;27(1):10-16.
26. Bidra AS, Touloumi F, Wu R. Differences in lip support with and without labial flanges in a maxillary edentulous population. Part 4: Patient-centered analysis. J Prosthodont. 2018;27(1):29-34.