You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Balanced occlusion has been proposed to promote the stability and retention of complete dentures.1 The objective of this concept is to maintain occlusal contacts not only in centric occlusion but also through the functional ranges of mandibular movements. This dynamic functionality of denture occlusion has been described as the interrelationship of five factors, the so-called Hanau quint, named for researcher Rudolph L. Hanau: condylar guidance (CG), incisal guidance (IG), orientation of occlusal plane (OP), compensating curve (CC), and cuspal incline (CI) (Figure 1).1-3
The CG is a measure of an angle formed by the condylar pathway down the articular eminence of the mandibular fossa of the temporal bone and the Frankfort horizontal plane.4-6 The angle of the condylar pathway is usually recorded with the mandible guided approximately 6 mm in protrusion, and is transferred to an articulator to program the mechanical equivalents of condylar elements.5
The IG is determined by the interincisal relationship of maxillary and mandibular anterior teeth.7,8 This functional relation of the anterior teeth can vary with the degree of vertical and horizontal overlaps, and is usually determined with wax trial dentures placed in the mouth. For esthetics, the vertical overlap is increased to display the incisors and mimic the relation of natural dentition. The increased IG, however, may alter the masticatory muscle activities and restrict the functional range of mandibular movements.8
The OP is an imaginary plane relating to the heights of anterior and posterior teeth.9 This plane is usually aligned to the ala-tragus line, interarch relation of the ridge, and retromolar pad, the lateral border of the tongue, and the commissure of the mouth.10 This plane may display a parallelism to the ridge of the denture foundation or an inclination toward the anterior or posterior direction. An ideal OP may display a relatively flat and parallel surface to the ridge of an edentulous arch.11 The flat surface of the OP, however, may display a mismatch when the condyle glides down the articular eminence in protrusion. The posterior teeth disclude from occlusion demonstrating an interocclusal gap between maxillary and mandibular teeth and creating the so-called "Christensen phenomenon."2,3
Commercially available artificial teeth demonstrate a wide range of CIs with different occlusal morphologies.11,12 In general, the teeth are classified as nonanatomic, semi-anatomic, and anatomic depending on the cuspal morphology. Nonanatomic teeth do not display a distinct cuspal morphology; anatomic teeth present a higher CI. However, the value of the CI is altered when the teeth are arranged on a compensating curve (CC) created in the OP.13 For example, a 30-degree artificial tooth can display either 20-degree or 40-degree CIs when the tooth is set on a 10-degree curve as a reference to the OP.
This article describes a formula introduced to quantify a balanced occlusion within the context of the Hanau quint and discusses the limitations of the formula that are due to individual variabilities of mandibular movements. A MEDLINE/PubMed search for keywords (Hanau quint, condylar guidance, incisal guidance, occlusal plane, compensating curve, cuspal incline) was supplemented with a hand search to identify relevant peer-reviewed articles published in English up to 2019.
Articulation in Centric Relation
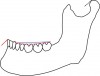
The maxillary and mandibular teeth are arranged to support the lower facial height and match with the centric relation of the condyle.14,15 When the teeth are in occlusion, the condyle ideally should be in the most stable position of the articular eminence (Figure 2 and Figure 3).15 This centric position of the condyle also should be in harmony with the neuromuscular complex of the masticatory system. This position is reproducible and recordable, and is well received as a treatment position for the fabrication of complete dentures.15
The occlusal morphology of artificial teeth should demonstrate spillways for an efficient masticatory function.11 The artificial teeth are placed to optimize the force direction under occlusal functions and enhance the esthetics of the lower facial profile. The posterior teeth are arranged to provide centric stops to keep the occlusal vertical dimension and direct the occlusal forces in vertical direction.12 The anterior teeth should not occlude and should demonstrate a freedom in centric relation of the mandible.15,16 The teeth can be arranged on a flat or curved OP to match with the arc of mandibular closure.
Anatomically, teeth demonstrate a distinct cuspal morphology for the establishment of cusp-to-fossa relations.12,17 An occlusal interference may occur in centric relation of the mandible when the maxillary cast is mounted on an articulator by means of an arbitrary facebow or earpiece bow.18,19 According to Weinberg, occlusal error is minimized when the arbitrary transverse horizontal axis is located within a 5-mm radius from the true hinge axis.20,21 However, the occlusal error can be pronounced when the occlusal vertical dimension is altered on the articulator. Because of close proximity to the transverse horizontal axis, the posterior teeth can display a greater degree of occlusal error. The anterior teeth are influenced far less than the posterior teeth when the arbitrary location displays a discrepancy from the true axis of rotation.18
The casts should be mounted on an articulator that can mimic the opening and closing motion of the mandible and allow the transfer of the facebow record. 20,21 The vertical condylar axis should be long enough to position the OP as a reference to the hinge axis. When mounted on an articulator displaying a short condylar axis, the arc of closure of the mandibular cast will be more acute than the arc of mandibular closure. A deflective occlusal contact can occur on the CI of posterior teeth, demonstrating an open bite in the anterior region.
The centric relation of the mandible may be an area rather than a point.22,23 The condyle appears to suspend in a relaxed or habitual position, and is further braced against the medial aspect of the mandibular fossa when the mandible is guided.24 A controversy may occur with this biomechanical aspect of condylar posture. The area of centric is described as either "long centric" or "freedom in centric."22,23 In addition, the masticatory cycle demonstrates a lateral component at the terminal phase of mandibular closure, blunting the tip of the tear-drop shape of the masticatory cycle.According to Suit et al, the lateral slide can range up to 1 mm.25
Articulation in Protrusion
The posterior teeth disclude when the mandible is advanced in the frontal direction.2,3 Having both the CG and IG set at 0 degree, the "Christensen phenomenon" of posterior disclusion does not occur. No interocclusal gap is observed when the OP is flat and parallel to the Frankfort horizontal plane. According to a previous study, the average CG of edentulous patients is 36 degrees with a range of 10 degrees to 62 degrees.4 Individual variation was as high as 25 degrees between the right and left sides of the temporomandibular joint. A symmetric CG was found only in 12.5% of subjects, and dissimilarities greater than 10 degrees were observed in 21.4% of subjects.
Posterior disclusion may not occur when the OP is inclined or incorporates a CC to raise the occlusal surface of posterior teeth (Figure 4 and Figure 5).2,3,13 The posterior interocclusal gap, the so-called "Christensen distance," can be closed with a cuspal morphology rising above the OP. The balance is maintained with the angulation of the posterior teeth as described as the inclination of OP, CC, CI, or a combination of these. The greater the CG, the more acute the inclination of OP, CC, or CI should be to achieve balance in protrusion.
The articulator should be equipped with adjustable condylar elements to program the CG. The right and left condylar elements should be independent from each other to match with the asymmetric condylar pathways as reported in a previous study.4 The condylar pathway is not linear, and is arcuate because of the convexity of the incline of the articular eminence.20,21 Thus, the value of CG can be inconsistent when programming the condylar elements based on a static interocclusal record. The graphic method will indicate the entire pathway of the condylar movement and can produce the curvilinear pattern of CG.26 However, many commercially available semiadjustable articulators are limited in reproducing the graphic record of condylar pathway.
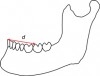
The condylar pathway is not altered by the interincisal relations of anterior teeth.17,26 The value of CG remains constant even when IG is altered for phonetics and esthetics. However, mandibular movement is influenced by the altered IG. When the IG becomes acute to meet the patient's demand, the angulation of OP, CC, CI, or a combination of these should be greater. In Swenson's formula, the sum of inclination of OP, CC, and CI is described as CI when quantifying the degree of inclination, as follows2,3:
CI = IG + d (CG-IG), where d is the fraction of distance from incisal point to each cusp in question (Figure 6).
According to this formula, the location of the tooth (d) is significant in producing the angulation of CI. The more anterior the tooth, the smaller is thevalue of d. When IG is greater than CG, premolars will demonstrate higher CI than molars. However, the last molar will display the greatest CI when IG is lower than CG.
Articulation in Lateral Excursion
The working condyle rotates along the vertical axis of the condyle, while the balancing condyle is pulled down the articular eminence.26,27 The occlusal morphology of posterior teeth is not influenced by the rotational movement of the working condyle. However, posterior disclusion occurs on the balancing side because of the downward movement of the balancing condyle. An incline should be developed to maintain the balance by matching the asymmetric cross-arch rotational movement of the mandible (Figure 7 through Figure 11).13
The working incline (sum of inclination of OP, CC, and CI) is influenced by the IG.28 When the IG is set at 0 degree, the working incline displays a flat surface. The incline is increased when the interincisal relation becomes more acute. However, the increase of the working incline is not directly proportional to the increase of the IG because of the individual rotational movements of the working condyle.28 The condyle does not demonstrate a pure rotational movement. The vertical axis of the condyle is displaced in the lateral direction with anterior, posterior, superior, or inferior movements, or a combination of these.20,21
The balancing condyle makes a circular motion in the medial direction when the working condyle rotates.26-28 This cross-arch rotational movement of the mandible may occur in two phases: immediate mandibular lateral translation (IT) and progressive mandibular lateral translation (PT). Although controversial, the working condyle cannot translate in a lateral direction unless the IT does not occur on the balancing side of the condyle. The bodily translation of the mandible is called Bennett movement,24 and Bennett angle is formed as the balancing condyle progresses further to continue the circular motion against the medial wall of the articular eminence.
The arc of a circle becomes more acute when the radius of the circle is decreased.29 The intercondylar distance is fixed and cannot be altered because of the unification of working and balancing condyles by means of the mandibular body. However, the lateral translation of the mandible displaces the center of rotation located in the working condyle and consequently alters the positional relation of the balancing condyle causing an effect of a decrease in the intercondylar distance as a reference to the original center of the rotation. In fact, the gothic arch tracing made by a graphic record is more lateral when combined with a smaller intercondylar distance.29 This effect is observed when a Hanau H2 articulator is simulated to mimic the lateral rotational movement of the mandible. The working condylar ball remains in the condylar slot but the intercondylar pin slides laterally through the ball.20,21
Discussion
Occlusal balance is described through the interrelationship of the Hanau quint.1 The CG is fixed and is presented by the patient. The IG is mostly determined by the dentist to match the patient's profile. The challenge for clinicians is determining the location and inclination of the teeth located between the posterior determinant of CG and the anterior determinant of IG.
The Swenson's formula presented earlier was introduced to quantify the inclination of posterior teeth and balance the occlusion in protrusion.2,3 In this formula, the CI represents a sum of the angulation of OP, CC, and CI. For example, 30-degree CI can be produced when a 10-degree cusp tooth is combined by 10-degree orientation of OP and 10-degree CC. The CIs are uniform through the posterior teeth when IG is set to be equal to CG.20,21 However, the inclination will change gradually along the OP when the IG is set to be higher or lower than CG. The more anterior the location of the tooth, the greater is the influence of IG. Thus, premolars will display a greater inclination than molars when IG is more acute than CG.
The value of d is not constant and is a weak link in the Swenson's formula. It indicates a relative location of a tooth from IG as reference to the two end-controlling factors.2,3 When considering the individual differences of craniofacial anatomy, the d is a variable and is unknown until the location is determined as reference to the IG. Alternatively, the dcan be quantified when the CI is determined in a complete denture demonstrating a balanced occlusion. According to Christensen, the average value of d can be approximated as follows: 0.5 for third molar, 0.4 for second molar, 0.3 for first molar, and 0.2 for premolars.2,3 This formula appears to produce good estimates for protrusive balance.28
An excessive inclination of OP may cause harm with regard to force direction and compromise function and esthetics.30 The OP is presented somewhat by the patient based on anatomic landmarks and functional relations with other masticatory structures. A curve can be incorporated into the OP to have an effect of inclination.31 This approach follows the geometric concept of a sphere crossing through the axis of the condyle and incisal point. This method, which is conceived based on anthromorphometric observation, is useful for designing a curved OP for balance. However, the optimal degree of CC is yet to be determined for balanced occlusion.
A cuspal morphology may rise above the OP to fill the interocclusal gap created by the posterior disclusion. According to Christensen, a cusp may demonstrate a height to compensate for the insufficient inclination of OP.2,3 In fact, balance refers to the inclination of a cusp and does not necessarily consider the height. The CI describes the angulation of posterior teeth, and cusp height determines the range of tooth contact occurring during excursive movements of the mandible.20,21 The CI starts at the occlusal contact in centric occlusion and serves as a guide for the opposing cusp to glide without breaking the balance. The taller the height of a cusp, the greater is the range of the balance. However, the functional range of mandibular movements rarely reaches the scope of the border movements.25
The lateral balance is important because of a high frequency of lateral movements of the mandible. The teeth are usually arranged to display a curve in the mediolateral direction. This mediolateral CC usually involves a more apical setting of lingual cusps than buccal cusps in the mandible. When the relative heights of those cusps are inverted, a reverse CC is produced. In essence, the CC is set to raise the balancing inclination and lower the working inclination. Interestingly, the working incline is decreased as a function of increasing the balancing incline (Figure 7). This approach enables a sphere to cross the OP in a lateral direction as indicated by the CI of posterior teeth.
Semiadjustable articulators have limitations in reproducing the CG. The widely used Hanau H2 articulator is incapable of distinguishing the so-called "Fischer angle," ie, the difference between the horizontal CG and the lateral CG.21,26 The former indicates the downward condylar pathway observed during protrusive movement, and the latter describes the downward pathway of the balancing condyle that occurred during lateral movement. However, the occlusal error resulting from the incapacity of accepting the Fischer angle may not be clinically significant.26
Some articulators are neither precise in reproducing the occlusal record nor capable of receiving a lateral interocclusal record.32,33 A significant difference was noted when the Hanau formula was used to set the lateral inclination of the condylar pathway. These articulators are not designed to adjust the intercondylar distance and individual motions of working condyle. According to Weinberg, occlusal error can be significant when errors are cumulative.21 However, the occlusal error of a complete denture resulting from use of a semiadjustable articulator can be minimized when combining <0.2 mm IT, <5 degrees difference in PT, <5 mm difference in intercondylar distance, <5 degrees difference in CG, and <5 degrees individual movements of working condyle.27
The positive occlusal error can be adjusted intraorally. The maxillary cast should be mounted by means of a facebow record, although the arbitrary transverse horizontal axis may not be located within a 5-mm zone from the true transverse horizontal axis.20,33 The facebow transfer procedure should also include an adequate location of the anterior reference point.34 The intercondylar distance can be measured using the facebow.29 When the distance is greater than 110 mm, the lateral condylar adjustment is set near 0 degrees during the occlusal adjustment for lateral balance. A significant variable would be Bennett movement and Bennett angle as indicated by IT and PT.35 The combination of these variables limits the application of the aforementioned Swenson's formula for determining the working and balancing inclinations.28
The centric relation is a key for the success of complete dentures.15 This position is a starting point for balanced occlusion. The cuspal morphology should not restrict the masticatory cycle of mandibular movement.25 The occlusal adjustment should be made to display a freedom in centric relation, maintain the occlusal vertical dimension, and balance the occlusion within the functional range of mandibular movements. When a balancing interference is noted, the maxillary palatal cusp is chosen as a centric stop to embrace the concept of lingual contact occlusion.12,36 The dynamic stability of complete dentures, however, is not warranted until the occlusion is balanced through the functional interrelationship of the Hanau quint.
Conclusion
Balanced occlusion obtained through the functional interrelationship of the Hanau quint can be quantified using the presented Swenson's formula. This formula was found to approximate the protrusive incline when the distance of a tooth in question was determined as a reference to IG and CG. However, when quantifying working and balancing inclines, the individual variabilities of condylar pathways and limitations of articulators commonly used to fabricate complete dentures should be considered. An occlusal error may occur requiring an intraoral adjustment. The centric relation of the mandible is critical as a starting point of balancing the occlusion. The occlusal adjustment should encompass the basic principles of complete denture design, including a freedom in centric relation of the mandible and maintenance of the occlusal vertical dimension.
About the Authors
Won-suk Oh, DDS, MS
Clinical Professor, Department of Biologic and Materials Sciences and Prosthodontics, University of Michigan School of Dentistry, Ann Arbor, Michigan
Berna Saglik, DDS, MS
Clinical Associate Professor, Department of Biologic and Materials Sciences and Prosthodontics, University of Michigan School of Dentistry, Ann Arbor, Michigan
Sun-yung Bak, DDS
Clinical Assistant Professor, Department of Biologic and Materials Sciences and Prosthodontics, University of Michigan School of Dentistry, Ann Arbor, Michigan
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
REFERENCES
1. Mack PJ. A discussion of some factors of relevance to the occlusion of complete dentures. Aust Dent J. 1989;34(2):122-129.
2. Christensen FT. Cusp angulation for complete dentures. J Prosthet Dent. 1958;8(6):910-923.
3. Christensen FT. The effect of incisal guidance on cusp angulation in prosthetic occlusion. J Prosthet Dent. 1961;11(1):48-54.
4. Zamacona JM, Otaduy E, Aranda E. Study of the sagittal condylar path in edentulous patients. J Prosthet Dent. 1992;68(2):314-317.
5. dos Santos J Jr, Nelson S, Nowlin T. Comparison of condylar guidance setting obtained from a wax record versus an extraoral tracing: a pilot study. J Prosthet Dent. 2003;89(1):54-59.
6. Hue O. The sagittal condylar paths in edentulous patients: analysis with computerized axiography. Int J Prosthodont. 2016;29(1):11-16.
7. Ogawa T, Koyano K, Suetsugu T. The influence of anterior guidance and condylar guidance on mandibular protrusive movement. J Oral Rehabil. 1997;24(4):303-309.
8. Celebić A, Alajbeg ZI, Kraljevic-Simunkovic S, Valentic-Peruzovic M. Influence of different condylar and incisal guidance ratios to the activity of anterior and posterior temporal muscle. Arch Oral Biol. 2007;52(2):142-148.
9. Celebić A, Valentić-Peruzović M, Kraljević K, Brkić H. A study of the occlusal plane orientation by intra-oral method (retromolar pad). J Oral Rehabil. 1995;22(3):233-236.
10. Oh WS, Alshhrani W, Saglik B, Hansen C. The commissure line of the mouth for orienting the occlusal plane. Int J Prosthodont. 2015;28(3):243-245.
11. Engelmeier RL. The development of nonanatomic denture occlusion: Part IV. J Prosthodont. 2019;28(1):e159-e171.
12. Engelmeier RL, Phoenix RD. The development of lingualized occlusion. J Prosthodont. 2019;28(1):e118-e131.
13. Scott WR. Application of "cusp writer" findings to practical and theoretical occlusal problems. Part II. J Prosthet Dent. 1976;35(3):332-340.
14. Forrester SE, Allen SJ, Presswood RG, et al. Neuromuscular function in healthy occlusion. J Oral Rehabil. 2010;37(9):663-669.
15. Wiens JP, Goldstein GR, Andrawis M, et al. Defining centric relation. J Prosthet Dent. 2018;120(1):114-122.
16. Dawson PE. A classification system for occlusions that relates maximal intercuspation to the position and condition of the temporomandibular joints. J Prosthet Dent. 1996;75(1):60-66.
17. Weinberg LA. Incisal and condylar guidance in relation to cuspal inclination in lateral excursions. J Prosthet Dent. 1959;9(5):851-862.
18. Zuckerman GR. The geometry of the arbitrary hinge axis as it relates to the occlusion. J Prosthet Dent. 1982;48(6):725-733.
19. Morneburg TR, Pröschel PA. Impact of arbitrary and mean transfer of dental casts to the articulator on centric occlusal errors. Clin Oral Investig. 2011;15(3):427-434.
20. Weinberg LA. An evaluation of basic articulators and their concepts. Part I. Basic concepts. J Prosthet Dent. 1963;13(4):622-644.
21. Weinberg LA. An evaluation of basic articulators and their concepts. Part II. Arbitrary, positional, semi adjustable articulators. J Prosthet Dent. 1963;13(4):645-663.
22. Schuyler CH. Freedom in centric. Dent Clin North Am. 1969;13(3):681-686.
23. Ramfjord SP, Ash MM. Reflections on the Michigan occlusal splint. J Oral Rehabil. 1994;21(5):491-500.
24. Levinson E. The nature of the side-shift in lateral mandibular movement and its implications in clinical practice. J Prosthet Dent. 1984;52(1):91-98.
25. Suit SR, Gibbs CH, Benz ST. Study of gliding tooth contacts during mastication. J Periodontol. 1976;47(6):331-334.
26. Hobo S. Formula for adjusting the horizontal condylar path of the semiadjustable articulator with interocclusal records. Part I: Correlation between the immediate side shift, the progressive side shift, and the Bennett angle. J Prosthet Dent. 1986;55(4):422-426.
27. Price RB, Kolling JN, Clayton JA. Effects of changes in articulator settings on generated occlusal tracings. Part II: Immediate side shift, intercondylar distance, and rear and top wall settings. J Prosthet Dent. 1991;65(3):377-382.
28. Lang BR, Thompson RM. The cusp angles of artificial mandibular first molars. J Prosthet Dent. 1972;28(1):26-35.
29. Taylor TD, Huber LR, Aquilino SA. Analysis of the lateral condylar adjustment of nonarcon semiadjustable articulators. J Prosthet Dent. 1985;54(1):140-143.
30. Ogawa T, Koyano K, Suetsugu T. Characteristics of masticatory movement in relation to inclination of occlusal plane. J Oral Rehabil. 1997;24(9):652-657.
31. Craddock HL, Lynch CD, Franklin P, et al. A study of the proximity of the Broadrick ideal occlusal curve to the existing occlusal curve in dentate patients. J Oral Rehabil. 2005;32(12):895-900.
32. Javid NS, Porter MR. The importance of the Hanau formula in construction of complete dentures. J Prosthet Dent. 1975;34(4):397-404.
33. Lee W, Lim YJ, Kim MJ, Kwon HB. Occlusal consequence of using average condylar guidance settings: an in vitro study. J Prosthet Dent. 2017;117(4):532-538.
34. Lauciello FR, Appelbaum M. Anatomic comparison to arbitrary reference notch on Hanau articulators. J Prosthet Dent. 1978;40(6):676-681.
35. Taylor TD, Bidra AS, Nazarova E, Wiens JP. Clinical significance of immediate mandibular lateral translation: a systematic review. J Prosthet Dent. 2016;115(4):412-418.
36. Goodkind RJ. A practical approach to balancing complete denture occlusions. J Prosthet Dent. 1971;26(1):85-92.