You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Neurodegenerative diseases are characterized by the loss of neurons in the brain or spinal cord. Acute neurodegeneration may result from a temporary discrete insult, such as stroke or trauma, leading to a localized loss of neurons at the site of injury. Chronic neurodegeneration may develop over a long period of time and results in the loss of a particular neuronal subtype or generalized loss of neuronal populations.
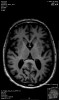
In the brain, Alzheimer’s disease and Huntington’s disease result in widespread loss of neurons (Figure 1), while Parkinson’s disease involves the specific and localized loss of dopaminergic neurons in the substantia nigra. In the brainstem and spinal cord, amyotropic lateral sclerosis and spinal muscular atrophy involve the degeneration and loss of motor neurons. While all of these conditions exhibit unique neuronal pathologies, the exact mechanisms for neuronal loss are complex, making the identification of efficacious treatments elusive.1
Gene defects play a major role in the pathogenesis of degenerative disorders of the nervous system. In fact, it has been the very knowledge gained from genetic studies that has allowed the elucidation of the molecular mechanisms underlying the etiology and pathogenesis of many neurodegenerative disorders.2
Huntington’s Chorea
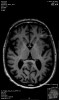
Huntington’s disease is named after George Huntington, the physician who described it as hereditary chorea in 1872. It is an incurable, adult-onset, autosomal dominant inherited disorder associated with cell loss within a specific subset of neurons in the basal ganglia and cortex.3 The most striking neuropathology in Huntington’s disease occurs within the neostriatum (Figure 2), in which gross atrophy of the caudate nucleus and putamen (Figure 3) is accompanied by selective neuronal loss and astrogliosis. Marked neuronal loss is also seen in deep layers of the cerebral cortex.4 The clinical features include a movement disorder, cognitive disorder, dementia, and behavior disorder. Patients may present with one or all disorders in varying degrees.5
The following case report describes the treatment of a patient with a neurodegenerative disease, characterized by uncontrolled movements that required general anesthesia. The report accentuates the safety of the used necessary medication.
Case Report
A 52-year-old female patient presented for dental treatments. Her chief oral complaints were recurrent swelling and pain around tooth No. 8, pain upon mastication, as well as difficulties in chewing and swallowing food. These symptoms worsened her systemic condition. She had been diagnosed with Huntington’s chorea 15 years prior.
The treatment consisted of tetrabenazine 25 mg per day and medical canabies given as cookies. Tetrabenazine is a monoamine depletor. The precise mechanism by which tetrabenazine exerts its anti-chorea effects is unknown, but it is believed to be related to being a reversible depletor of monoamines (such as dopamine, serotonin, norepinephrine, and histamine) from nerve terminals. The patient was cachectic and had progressive mental deterioration, ataxia, and gross chorea movements. Her speech was blurred but coherent.
Her physical examination revealed a regular pulse rate of 80/minute and a blood pressure of 105/70 mm. Her body weight was 50 kg (~110 lbs.), and the body mass index (BMI) was 18.3. Her plasma glucose was 77 mg/dl and urea 22 mg/dl; electrolyte values, differential blood count, and electrocardiogram (ECG) were within normal limits.
Oral Examination
Oral soft tissues—The patient’s mucosa and tongue were healthy. The salivary glands and salivary secretion showed no pathology. Regional lymph nodes were not palpable. The periodontal examination revealed gingivitis and periodontitis with shallow pockets of up to 6 mm.
Dental examination—Tooth No. 8 revealed a chronic periapical lesion and was not vital with a grade 3 mobility. Tooth No. 16 had a deep carious lesion. All teeth showed extensive attrition. Several teeth (Nos. 4, 7, 12, 13, and 30) had been extracted in the past, probably due to carious lesions and periodontal involvement. Fixed dental bridges were the first option to replace the missing teeth, as the patient’s neurological involvement, lack of coordination, and involuntary movements excluded any possible treatment using removable bridges.
Dental Treatment Plan
The treatment plan called for teeth Nos. 8 and 16 to be extracted. Two dental bridges (2-3-x-5-6-x-x-9-10-11-x-x-x-15 and 29-x-31), both temporary and porcelain-fused-to-metal, would be implemented.
Due to the patient’s extreme uncontrolled body movements, including the head, lower jaw, and tongue, and dentophobia, it was decided to perform the dental treatment under continuous administration of tetrabenazine 25 mg through the day of surgery, as well as the canabies. Antibiotic treatment with amoxicillin 500 mg 3/day was indicated only following surgery.
Anesthesia
In the operating room an intravenous (IV) line was established. Vital signs were monitored with a 5-electrode ECG, blood pressure monitor, capnograph, nerve stimulator, and pulse oximeter. The initial values were as follows: blood pressure, 105/70; pulse rate, 80/min; O2 saturation, 99%; end-tidal (Et) CO2, 32%. During the general anesthesia, vital signs were stable: blood pressure, 110/50 – 95/40; arterial oxygen saturation (SaO2), 96% to 99%; EtCO2, 31% to 33%.
Local infiltration anesthesia with lidocaine 2% and adrenaline 1:100,000 was added prior to dental extractions. The patient was preoxygenated with 100% O2, and the induction of anesthesia was achieved with propofol 100 mg IV and Esmerone (rocuronium) 40 mg IV. Nasal intubation was performed with a 7-mm cuffed endotracheal tube.
Anesthesia was maintained with fentanyl 0.05 to 0.12 mg/kg/min IV and isoflurane <0.4% in a mixture of O2 50% in air without nitrous oxide for 4 hours.
Dental Treatments Under General Anesthesia
The abutment teeth underwent crown preparations with a chamfer finishing line. Impressions were preformed with polyvinyl siloxane (PVS) materials. Acrylic temporary bridges with metal reinforcement were prepared ahead of time and adapted at the end of the procedure. Bite registration was done with PVS material in spite of the difficulty of obtaining the correct intermaxillary relation during anesthesia.
Reversal of the effect of the muscle relaxant was obtained with myostigmine 2.5 mg IV and atropine 0.5 mg. The patient was extubated and woke up immediately following the interruption of the fentanyl and isoflurane, breathing spontaneously and speaking coherently.
The next stages of prosthetic dental treatments were continued in the regular hospital dental clinic without any relaxants or tranquilizers. However, it is important to note that the patient was regularly using medical canabies. During the try-in of the bridges (Figure 4) the patient was very cooperative and, most significantly, had almost no involuntary movements.
As a follow-up, the patient was guided to a strict oral hygiene and periodontal dental hygienist treatment regimen (Figure 5).
Discussion
Clinical experience with the management of dental treatments under general anesthesia in Huntington’s chorea is too limited to propose specific drugs or techniques. Reported anesthesia experience in patients with Huntington’s disease is largely anecdotal and consists of a small number of case reports and letters to the editors.6-16
Although there are no specific contraindications to using intravenous or inhaled anesthetics, delayed awakening and generalized tonic spasms have been reported after administration of thiopental.10 In the present case, the authors avoided its use and replaced it with propofol without any side effects. Propofol is a commonly used general anesthesia induction agent.11 It can be a valuable tool to achieve deep sedation or general anesthesia and provides rapid onset and recovery.12 A normal response with rapid recovery with propofol has been reported in the literature in patients with Huntington’s disease.17-19 It has been suggested that these patients could be sensitive to the effects of non-depolarizing muscle relaxants, although the reported response to atracurium has been normal.18-20
Interestingly, the incidence of decreased pseudocholinesterase activity is substantially higher in Huntington’s disease patients than in the normal population.7 This may explain the single report of prolonged muscle relaxant response to succinylcholine. In the present case, the authors decided not to use it for safety reasons. The use of sevoflurane and mivacurium for general anesthesia in patients suffering from Huntington’s disease seems to be effective and safe18 as previously shown.
The authors used glycopyrrolate and not atropine in this case preoperatively, because central anticholinergic effects may exacerbate choreiform movements. Patients with Huntington’s disease are at higher risk of intraoperative complications, including pulmonary aspiration,6,19 and exaggerated sedation when using midazolam.13
The primary goal in general anesthesia for these patients is to provide airway protection and a rapid and safe recovery. The recently introduced inhalational agent sevoflurane could eliminate the problem of prolonged recovery because of its favorable pharmacokinetic profile.21 The authors instead used isoflurane, which provided similar results but was less costly. Prolonged apnea induced by suxamethonium was averted by using rocuronium with a rapid sequence induction.22
Factors of considerable concern to the dentist-anesthesiologist team treating patients with Huntington’s disease should include: (1) how to treat these frail elderly people who are incapable of cooperation; (2) how to relate and plan treatments for patients suffering from malnutrition; and (3) how to treat patients with an increased risk for aspiration at regular dental setups. Possible exaggerated response to sodium thiopental and succinylcholine used in classic anesthesia protocol should be taken into consideration. Other concerns regarding anesthetic management are determined by the level of physiologic and psychologic debilitation in the individual patient.
Conclusion
The authors described the management of a patient with Huntington’s disease who neglected her oral health due to objective difficulties of treatment. General anesthesia with a proper choice of drugs as described in this case seems to be a safe approach in patients with this malady and other neurodegenerative disorders. The elimination of nocive oral foci and the increase in chewing abilities significantly improved the patient’s general condition.
Discolsure
The authors had no disclosures to report.
About the Authors
Irena Haimov-Kaldess, DMD
Resident
The Dental Branch
Assaf-Harofeh Medical Center
Beer–Yaakov, Israel
Doron Haim, DMD, MPA
Associate Professor
Faculty of Dental Medicine
University of Medicine and Pharmacy
Iasi, Romania
Director
The Dental Branch
Assaf-Harofeh Medical Center
Beer–Yaakov, Israel
Adi Garfunkel, DMD
Professor of Oral Medicine
Former Dean and Hospital Oral Medicine Head
Faculty of Dental Medicine
Hadassah Hebrew University
Jerusalem, Israel
Academic Director
The Dental Branch
Assaf-Harofeh Medical Center
Beer–Yaakov, Israel
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
References
1. Dorsey ER, Constantinescu R, Thompson JP, et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology. 2007;68(5):384-386.
2. Bertram L, Tanzi RE. The genetic epidemiology of neurodegenerative disease. J Clin Invest. 2005;115(6):1449-1457.
3. Huntington G. On chorea. Med Surg Report. 1872;26:317-321.
4. Vonsattel JP, DiFiglia M. Huntington disease. J Neuropathol Exp Neurol. 1998;57(5):369-384.
5. Nucifora FC Jr, Sasaki M, Peters MF, et al. Interference by huntingtin and atrophin-1 with cbp-mediated transcription leading to cellular toxicity. Science. 2001;291(5512):2423-2428.
6. Stoelting RK, Dierdorf SF, McCammon RL. Anesthesia and Co-existing Disease. New York, NY: Churchill Livingstone; 1988:307.
7. Farina J, Rauscher LA. Anaesthesia and Huntington’s chorea. A report of two cases. Br J Anaesth. 1977;49(11):1167-1168.
8. Gualandi W, Bonfanti G. A case of prolonged apnea in Huntington’s chorea. Acta Anaesthesiol. 1968;19(suppl 6):235-238.
9. Costarino A, Gross JB. Patients with Huntington’s chorea may respond normally to succinylcholine. Anesthesiology. 1985;63(5):570.
10. Davies DD. Abnormal response to anaesthesia in a case of Huntington’s chorea. Br J Anaesth. 1966;38(6):490-491.
11. Propofol (Diprivan®). US Dept of Justice. Drug Enforcement Administration. Office of Diversion Control. Drug & Chemical Evaluation Section. January 2013. http://www.deadiversion.usdoj.gov/drug_chem_info/propofol.pdf#search=propofol. Accessed November 10, 2015.
12. Wischmeyer PE, Johnson BR, Wilson JE, et al. A survey of propofol abuse in academic anesthesia programs. Anesth Analg. 2007;105(4):1066-1071.
13. Rodrigo MR. Huntington’s chorea: midazolam, a suitable induction agent? Br J Anaesth. 1987;59(3):388-389.
14. Kaufman MA, Erb T. Propofol for patients with Huntington’s chorea? Anaesthesia. 1990;45(10):889-890.
15. Johnson MK, Heggie NM. Huntington’s chorea. A role for the newer anaesthetic agents. Br J Anaesth. 1985;57(2):235-236.
16. Fernandez IG, Sanchez MP, Ugalde AJ, Hernandez CM. Spinal anaesthesia in a patient with Huntington’s chorea. Anaesthesia. 1997;52(4):391.
17. Gaubatz CL, Wehner RJ. Anesthetic considerations for the patient with Huntington’s disease. AANA J. 1992;60(1):41-44.
18. Soar J, Matheson KH. A safe anaesthetic in Huntington’s disease? Anaesthesia. 1993;48(8):743-744.
19. MacPherson P, Harper I, MacDonald I. Propofol and remifentanil total intravenous anaesthesia for a patient with Huntington disease. J Clin Anesth. 2004;16(7):537-538.
20. Lamont AM. Brief report: anaesthesia and Huntington’s chorea. Anaesth Intensive Care. 1979;7(2):189-190.
21. Nagele P, Hammerle AF. Sevoflurane and mivacurium in a patient with Huntington’s chorea. Br J Anaesth. 2000;85(2):320-321.
22. Kulemeka G, Mendonca C. Huntington’s chorea: use of rocuronium. Anaesthesia. 2001;56(10):1019.