You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Assessment of pulpal vitality for problematic teeth provides important information that significantly affects the patient’s complete treatment plan. Determination of pulpal health and diagnosis of dental pain that may be pulpally related can be challenging.1 Endodontic diagnosis and discovery of asymptomatic pulp-associated disease is part of the routine comprehensive examination.2 In such a case, the patient may be unaware of existing endodontic pathology that is initially diagnosed from radiographic evidence and confirmed with a clinical examination and supplemental pulp vitality testing. The other clinical situation is when the patient presents for an emergency with acute pain and other symptoms are present.2 In these circumstances, the patient may have pain due to trauma to a tooth, possible infection and swelling of the soft tissues adjacent to the tooth, an infected pulp due to caries or periodontal disease, and tooth soreness in normal function. The emergency visit requires a collection of data through the use of radiographs and a clinical examination to determine a diagnosis. Once the diagnosis is ascertained, the patient can be presented with treatment options.
When radiographic evidence, clinical evidence, or acute pain may indicate the need for endodontic treatment, the endodontic evaluation and examination should include a systematic evaluation. Radiographically, it is important to have a diagnostic image that includes the crown and apex of the root. If possible, the image should have little if any overlap with the adjacent teeth, although sometimes multiple images must be taken in order to visualize all critical areas of the tooth. The tooth may be restoration-free with or without caries, have existing restorations, or have a restoration with existing endodontic treatment. Combinations of clinical conditions may be present. The clinician also should evaluate the face for symmetry, swelling, and discoloration. Evidence of variations from normal can provide important diagnostic clues. An intraoral examination of the soft tissue adjacent to the tooth provides critical information in determining not only the diagnosis but also treatment options. Look for swelling, changes in tissue tone and color, and evidence of a fistula or sinus tract. Evaluate the tooth for infection and drainage of pus.
Clinical testing of suspected teeth is important. Also, the interpretation of the data collected from clinical testing and the radiographic evidence will shape the treatment decision. Various clinical tests can be performed to help make an endodontic diagnosis and are divided into two specific categories—evaluation of the supporting periodontal structures and assessment of pulp vitality. When collecting data, the clinician should use a control tooth to gauge what is normal.2
Pulp Vitality Testing
A critical part of an endodontic examination and evaluation is an assessment of pulpal vitality. Even in the presence of obvious radiographic evidence of periapical pathology, pulp vitality testing is important in determining the treatment. The ideal pulp test would be simple, objective, standardized, and reproducible. This test should be inexpensive to perform and should not cause pain or injury.3 Pulpal vitality tests include electric pulp tests (EPTs) and the thermal tests of cold and heat.4 These indirect pulpal vitality tests assess a stimulus-response reaction in the patient and are used because the pulpal tissue cannot be assessed directly by histologic means.
Specific clinical circumstances can present problems in assessing pulp vitality. Traumatized teeth can permanently lose sensory function but maintain an intact vascular system.5,6 Also, teeth that are immature or in active orthodontic treatment may provide for unreliable pulp vitality testing.7,8
Electric Pulp Test
The EPT is based on the stimulation of pulpal sensory nerve fibers causing a perceived sensation.9 The two types of sensory fibers in the pulp are myelinated (A) and unmyelinated (C). Myelinated A sensory nerve fibers are responsible for innervating dentin; 90% of A fibers are delta. C sensory nerve fibers innervate the body of the pulp.9 EPT uses a low-intensity controlled electric stimulation that can induce non-painful (pre-pain) sensations of the A-delta fibers.10 Increasing the electric stimulus to higher levels of electric current can elicit pain. Correct use of an EPT should invoke only a prepain response. Applying a low-intensity electrical stimulation with an EPT relies on a patient’s subjective evaluation and comments to the clinician. This can lead to both false-positive and false-negative results. When the patient’s response is indeterminate, the test should be repeated; in some cases the order of testing the teeth should be changed to determine the patient’s reliability.
EPT is technique-sensitive.11 To get an adequate result, the tooth must be clean and dry; the anatomic location should have no restoration, orthodontic band or brackets, or arch wire; and an adequate stimulus should be applied having contact between the tooth probe and tooth for a completed electrical circuit. Even with these challenges, the EPT is safe, valuable, and effective.12,13
Evaluation with Percussion and Palpation
Endodontic evaluation also includes the use of percussion and palpation to assess the supporting tooth structures. Percussion is the use of a hard, rigid instrument, typically a mirror handle, for tapping on the occlusal surface of posterior teeth or the incisal edge of anterior teeth. The directional force with this tapping should follow the long axis of the tooth being tested and facial surface. Before percussing a tooth, this author evaluates tooth sensitivity during excursive tooth movements and in maximum intercuspation. He also evaluates tooth fremitus (maxillary teeth) and tooth mobility. For teeth with sensitivity in occlusion, it is valuable to use thin film articulating ribbon (Accufilm 2 [Parkell, Inc]; Artifoil [Pulpdent], Exacta Film [Whip Mix Corporation]) to mark the occlusion to determine excessive occlusal forces. Teeth that are extremely sensitive to pressure, such as to a clinician’s fingers, should be percussed more gently than a tooth that, from a preliminary evaluation, appears to have a normal response. Any differences to percussion between the control tooth and suspected tooth should be noted. Also, the clinician should rule out a vertical or horizontal tooth fracture by having the patient bite on a bite stick (Figure 1).
Another test of the supporting tissues is palpation. Using gloved fingers, apply firm pressure on the gingival tissues and alveolus over the tooth apex. This test helps indicate the extension of any periapical inflammation. A positive response to palpation (discomfort and pain) indicates periapical inflammation.2,14
Selection of an Electric Pulp Testing Device
EPTs are chosen based on the clinician’s personal preference. Some prefer to use a device that provides digital readout with control over the increased rate of mild current flow. Other clinicians desire complete control using an analog unit with a finger-operated control over the mild electric current applied to the tooth. Both types of EPTs perform the needed testing to gather key clinical information to make a diagnosis. Unlike other manufacturers, Parkell offers both a digital (Digitest) and analog (Gentle Pulse) EPT device for assessment of pulp vitality. Another example of a digital electric pulp-testing device is the Vitality Scanner (Kerr Corporation). A clinician can choose the device, or the decision can be based on the patient’s symptoms and dental history. The use of an EPT device is contraindicated in patients wearing pacemakers. For these patients, it is advisable to use thermal testing only. In the author’s practice, he uses both devices depending on the patient’s symptoms and dental history with pulp vitality testing. It is the clinician’s goal to provide an EPT that will avail an accurate assessment to aid in determining a diagnosis, while helping to reduce anxiety and stress in the patient.
The Digitest (Figure 2) is a handheld, ergonomically designed instrument that has been designed using integrated circuitry that generates a complex, pulsed waveform. A weak, controlled current repeats several times a second. This waveform allows for a more controlled assessment of large-diameter nerve fibers (A delta fibers) within the odontoblastic processes so the patient perceives the stimuli below the pain threshold. The gradual controlled, gradual increase in the electrical stimulation is restricted by the microprocessor in order to prevent any jump in stimulus that can trigger a painful response. A patient will report a mild sensation for a vital tooth with a significant time lag before a patient experiences discomfort. The device is powered by a standard, user-replacable, preinstalled 9-volt battery. Unlike other EPT devices, the practitioner has several methods for grounding the unit to complete the electric circuit. The patient can either touch the handle of the Digitest instrument with a finger. Or the circuit can be completed using a ground wire with a lip-shaped hanger attached to the instrument so it can be placed gently, cradled on the patient’s lip. The device also has two different lengths of autoclavable EPT tooth probes (Figure 3). Both the lip-grounding wire and EPT probes can be sterilized in a conventional steam autoclave. The Digitest device should not be autoclaved but should be cleaned with a cloth or paper towel dampened with a surface disinfectant.
Using a Digital EPT Device
When using any pulp tester, the battery must be functioning. If the battery needs replacement in the Digitest instrument, the digital readout will fail to display red numbers or small red decimal points will appear when the unit is on.
Selecting the teeth to test is done after reviewing the patient’s dental history of a given tooth, evaluating and examining the tooth in question, and viewing the diagnostic radiographs. Typically, one tooth that according to the findings from the examination and radiographic evidence has normal pulp vitality is used as the control. The EPT device should be readied for testing by attaching the grounding wire and inserting either the long or short probe (long probe for more posterior molars, short probe for teeth more anterior). In some cases, the practitioner may want the patient to ground the EPT device by placing a finger on the metal cover of the instrument. The Digitest device offers three controlled rates of current increase: fast, medium, and slow. The three-position stimulus rate-adjustment slide switch is adjacent to the start button. The author prefers using the medium setting for most clinical circumstances. However, for the anxious patient, the author will employ the slow rate.
The teeth to be tested are cleaned and dried. To ensure adequate contact for electrical conduction between tooth, probe, and device, the author prefers to use a small amount of toothpaste on the metal tip of the probe. For best results when using an EPT, the metal tip of the toothpaste-covered probe should be placed on the middle of the facial or lingual surfaces of the tooth structure. It is advisable to not place the probe on a restorative material (metal, composite, ceramic) or touching gingival tissues. The probe should not touch a patient’s lips or cheeks. With the probe tip in position and stimulus rate set, the device is activated and started by pressing and holding the start button. Before beginning, the author provides the patient with specific instructions to raise a hand or arm when a sensation occurs. When the patient indicates a response, the start button is released and the stimulus stops immediately. The reading will be fixed on the display for 5 seconds after the button is released. The device automatically turns off. In some cases, a patient responds quicker due to anxiety. If the results appear to be inconsistent with other clinical evidence, the author will repeat the measurement. The maximum reading/stimulus on the Digitest device is 64. A reading of 64 is usually indicative that the pulp of the tooth being tested is nonvital. When a tooth has no response, the author will do a cold test of the tooth, using a cotton applicator that has been sprayed with ethyl chloride for verification. When cold testing, keep the application of cold away from the gingival tissues and only one tooth to avoid a false self-report of a sensation. A control tooth either adjacent to the tooth being tested or on the contralateral side will provide additional diagnostic information.
Using an Analog EPT Device
The Gentle-Pulse pulp vitality tester is an analog device that uses an operator-controlled dial to determine pulp vitality (Figure 4). The use of an analog EPT with an operator-controlled dial allows the clinician to customize the speed and intensity of the stimulus when compared to digital devices that provide increasing electrical stimuli that are controlled by the integrated circuitry of the device in a linear mode. Like all EPT devices, a mild electrical current is applied to the tooth being tested. The technique for pulp testing using tooth probes and electric grounding wire are the same as the Digitest. However, the Gentle-Pulse unit employs a gradual electric current rise. With the Gentle-Pulse device, the clinician controls the strength of the weak electric stimulus with the unit dial. After a thorough assessment of the tooth, the clinician can perform an EPT to collect additional information for determining pulp vitality. For the Gentle-Pulse, the control dial is turned clockwise to activate the device. The indicator light blinks continuously to show the unit is functioning. The dial should be turned slowly starting from the lowest reading until the patient indicates a stimulus. As previously described, a control tooth should be used. The number on the dial should be noted for all teeth. The number does not correspond with any clinical diagnosis other than there was a response at that level. Values of low, moderate, and high on the dial do not indicate a level of health or pathology—only that there was a response to the stimulus.
Case Reports
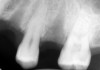
The use of EPT to assess a tooth prior to restorative or endodontic treatment depends on the clinical situation. For teeth with obvious periapical radiolucencies indicative of chronic abscess or cysts, a pulpal vitality test will confirm the diagnosis (Figure 5). In the presence of deep caries, using an EPT can confirm pulp vitality before initiating the restorative procedure (Figure 6 and Figure 7). In the case in which the radiograph demonstrates significant caries near the pulp, the EPT can provide additional information. For this patient with no history of pain in the maxillary first molar, the radiographic and clinical appearance of occlusal caries lead to the use of EPT to demonstrate lack of pulpal vitality (Figure 8). For large Class V carious lesions, the radiograph is usually not helpful in determining potential endodontic needs. Using an EPT provides a more definitive expectation of the extent of the caries relative to the pulp (Figure 9).
Use of EPT for Evaluation of Local Anesthesia
Patients expect pain-free restorative dental procedures. In some circumstances, local anesthesia may not be sufficient for pain-free tooth preparation and restoration or endodontic treatment.15,16 While for mandibular block anesthesia, the patient may have signs and symptoms of lip, gingival, and tongue anesthesia, it is not unusual for the pulp to not be profoundly numb. Reported failure rates of mandibular blocks are 15% to 45%.17-19 Clinical trials have assessed the successful use of EPT to evaluate the presence or absence of profound pulpal anesthesia.20,21 It has been reported that prolonged EPT in use conjunction with local anesthesia did not cause any histologic damage to the dental pulp.12,13 The use of EPT is safe, effective, and reliable for assessing dental anesthesia.
Conclusion
Pulp vitality testing provides important information in establishing an endodontic diagnosis. No one pulp testing assessment and evaluation technique can consistently provide a diagnosis of all pulpal conditions and pathologies. Identification of the problematic tooth, a thorough clinical examination (percussion, palpation, EPT, and thermal testing) and a review of the patient history of symptoms and radiographic evaluation will help establish a diagnosis and treatment options.
Typically, teeth with more dentin overlying the pulp will have higher EPT readings, eg, posterior teeth and teeth for older adults will have higher readings than anterior teeth. In the case of electric pulp testing, a maximum setting can be indicative of a nonvital tooth. However, other factors must be considered. Similar differences in results will be noted with thermal testing of teeth (usually cold testing). False positives are possible with EPT. Conduction of the current to gingival tissues can provide for a false positive.1 Higher readings may be observed with traumatized teeth and in older patients.1,7 Teeth with localized necrosis of pulp tissue can conduct electrical current; teeth with the presence of caries extending into the pulp chamber or that have been traumatized, can have vital and nonvital pulp tissues that will provide equivocal information on pulp vitality.1,23 Also, the mild electrical current can be conducted to adjacent teeth due to the presence of adjacent proximal contacting metallic restorations or the presence of metallic orthodontic appliances. This may lead to a false positive.1,24 For making a diagnosis, it is important to evaluate the patient’s behavior and responses when testing control teeth. The indirect nature of pulpal vitality testing using EPTs has been proven to be safe, effective, and valid for determining an endodontic diagnosis.22
About the Author
Howard E. Strassler, DMD, FADM, FAGD
Professor, Division of Operative Dentistry
Department of Endodontics, Prosthodontics and Operative Dentistry
University of Maryland Dental School
Baltimore, Maryland
References
1. Rowe AH, Pitt Ford TR. The assessment of pulpal vitality. Int Endod J. 1990;23(2):77-83.
2. Holland GR, Walton RE. Diagnosis and treatment planning. In: Torabinejad M, Walton RE, eds. Endodontics: Principles and Practice. 4th ed. 2002:68-93.
3. Chambers IG. The role and methods of pulp testing in oral diagnosis: a review. Int Endod J. 1982;15(1):1-15.
4. Petersson K, Söderström C, Kiani-Anaraki M, et al. Evaluation of the ability of thermal and electrical tests to register pulp vitality. Endod Dent Traumatol. 1999;15(3)127-131.
5. Pileggi R, Dumsha TC, Myslinksi NR. The reliability of electric pulp test after concussion injury. Endod Dent Traumatol. 1996;12(1):16-19.
6. Waikakul A. Kasetsuwan J, Punwutikorn J. Response of autotransplanted teeth to electric pulp testing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(2):249-255.
7. Gopikrishna V, Pradeep G, Venkateshbabu N. Assessment of pulp vitality: a review. Int J Paediatr Dent. 2009;19(1):3-15.
8. Hall CJ, Freer TJ. The effects of early orthodontic force application on pulp responses. Aust Dent J. 1998;43(5):359-361.
9. Lin J, Chandler NP. Electric pulp testing: a review. Int Endod J. 2008;41(5):365-374.
10. Olgart L. Excitation of intradental sensory units by pharmacological agents. Acta Physiol Scand. 1974;92(1):48-55.
11. Cooley RL, Barkmeier WW. An alternative to electric pulp testing. Quintessence Int Dent Dig. 1977; 8:23-25.
12. Mumford JM. Pain perception threshold on stimulating human teeth and the histological condition of the pulp. Br Dent J. 1967;123(9):427-433.
13. McDaniel KF, Rowe NH, Charbeneau GT. Tissue response to an electric pulp tester. J Prosthet Dent. 1973;29(1):84-87.
14. Hyman JJ, Cohen ME. The predictive value of endodontic diagnostic tests. Oral Surg Oral Med Oral Pathol. 1984;58(3):343-346.
15. Lai TN, Lin CP, Kok SH, et al. Evaluation of mandibular block using a standardized method. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(4):462-468.
16. Goldberg S, Reader A, Drum M, et al. Comparison of the anesthetic efficacy of the conventional inferior alveolar, Gow-Gages and Vazirani-Akinosi techniques. J Endod. 2008;34(11):1306-1311.
17. Malamed SF. Handbook of Local Anesthesia. St. Louis, MO: Mosby; 2004:227-253.
18. Cohen HP, Cha BY, Spångberg LS. Endodontic anesthesia in mandibular molars: a clinical study. J Endod. 1993;19(7):370-373.
19. Potocnik I, Bajrović F. Failure of inferior alveolar nerve block in endodontics. Endod Dent Traumatol. 1999;15(6):247-251.
20. Goodman A, Reader A, Nusstein J, et al. Anesthetic efficacy of lidocaine/meperidine for inferior alveolar nerve blocks. Anesth Prog. 2006; 53(4):131-139.
21. Certosima OJ, Archer RD. A clinical evaluation of the electric pulp tester as an indicator of local anesthesia. Oper Dent. 1996;21(1):25-30.
22. Weisleder R, Yamauchi S, Caplan DJ, et al. The validity of pulp testing: a clinical study. J Am Dent Assoc. 2009;140(8):1013-1017.
23. Drummer PM, Hicks R, Huws D. Clinical signs and symptoms of pulp disease. Int Endod J. 1980;13(1):27-35.
24. Myers JW. Demonstration of a possible source of error with an electric pulp tester. J Endod. 1998;24(3):199-200.