You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Adhesive dentistry began in the mid 1950s when Buonocore suggested using acid on the tooth structure surface before applying resins. A decade later, Buonocore and his colleagues suggested that resin tag formation was essential to the establishment of a strong bond to acid-etched enamel. From this foundational period of enamel-only bonding, modern adhesive dentistry evolved to employ 4th-, 5th-, 6th-, and 7th-generation systems that can also bond to dentin.
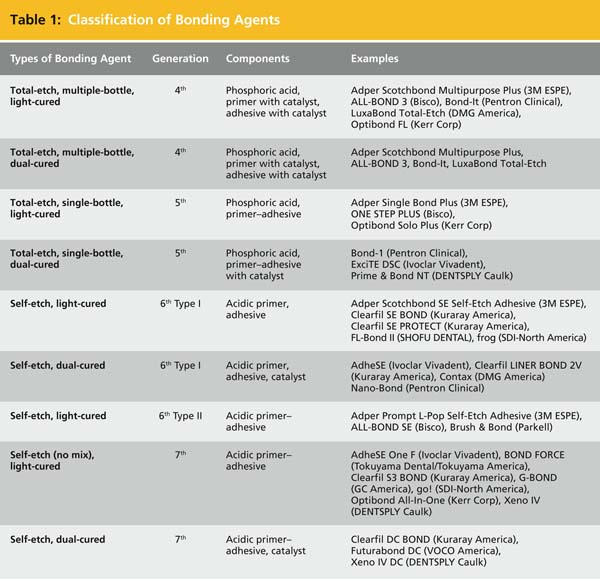
Nine types of bonding agents are included in these four generations.1-5 The first two types are in the 4th-generation systems, which were introduced in the 1990s. Both use total-etch bonding agents (with phosphoric acid as the etching component) and separate bottles for primer and adhesive. They are available with either light-cured or dual-cured setting types. There are also two product types in the 5th generation systems, which advanced to contain primer and adhesive in a single bottle. Introduced in the mid 1990s, these also use total-etch bonding agents and are available in either light-cured or dual-cured products.
The 6th-generation systems represented a major advance when they entered the market in the 2000s: these were the first self-etch products that relied on the use of an acidic primer, eliminating the need for phosphoric acid as a tooth surface etchant. With 6th-generation Type I, self-etching primer and resin adhesive are applied in separate layers and available in either light-cured or dual-cured setting products. To simplify the bonding procedure, a combined self-etch primer and adhesive was developed to create 6th-generation Type II products, which are available only in a light-cured type.
The 7th-generation systems—the newest to the market—were introduced in the mid 2000s. Using a single-bottle system, these last two types of the nine types of bonding agents require the fewest number of steps, and are available in either light-cured or dual-cured setting types (Table 1).
 |
CATEGORIES OF BONDING AGENTS
Total-Etch Bonding Agents
Fourth-generation total-etch bonding systems transformed dentistry in the early 1990s. While suitable for enamel-only bonding, they allowed more success in bonding to dentin, with dentinal bond strengths of 17 MPa to 25 MPa, encouraging many dentists to switch from amalgam to composite resin. The two components, a primer and an adhesive, are in separate bottles and must be mixed in precise ratios before being applied in separate layers after the tooth structure is etched with phosphoric acid. The light-cured products in 4th-generation systems typically require four steps, including etching, rinsing and drying, primer application, and adhesive application, while 4th-generation dual-cured products typically necessitate six steps, including etching, rinsing and drying, mixing both components with a catalyst, applying primer, and applying adhesive (Table 2). Examples of light-cured systems include Adper™ Scotchbond™ Multipurpose Plus (3M ESPE, www.3mespe.com), ALL-BOND 3™ (Bisco, www.bisco.com), Bond-It® (Pentron Clinical, www.pentron.com), LuxaBond® Total-Etch (DMG America, www.dmg-america.com), and Optibond FL (Kerr, www.kerrdental.com). Dual-cured system products include Adper Scotchbond Multipurpose Plus, ALL-BOND 3, Bond-It, and LuxaBond Total-Etch.
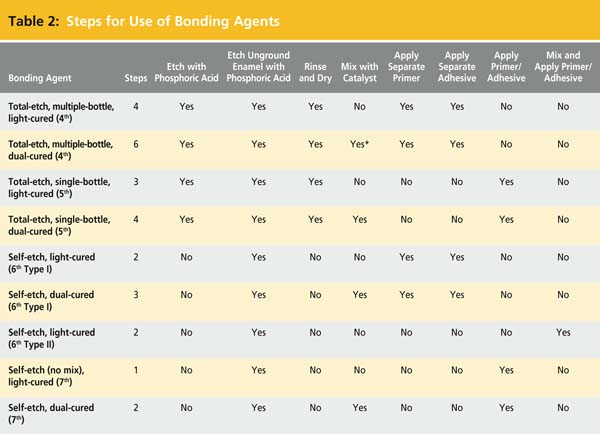 |
The number of steps and requirements for exact component measurements of 4th-generation systems can be difficult to perform chairside, increasing the risk for error. This led to the development of 5th-generation dental adhesives, characterized by single-bottle bonding agents with no mixing, minimizing the possibility for error.3 Suitable for application to uncut enamel, but with impressive dentinal bond strengths of 20 MPa to 25 MPa, these simpler systems combine the primer/adhesive monomer, which is applied in one or more layers after tooth etching with phosphoric acid. Fifth-generation light-cured systems typically require etching, rinsing and drying, and primer/adhesive application, while the dual-cured systems necessitate an additional step of mixing with a catalyst (Table 2).3 Light-cured 5th-generation bonding agents include Adper Single Bond Plus (3M ESPE), ONE STEP PLUS (Bisco), and Optibond® Solo Plus (Kerr). Dual-cured 5th-generation bonding agents include Bond-1 (Pentron Clinical), ExciTE® DSC (Ivoclar Vivadent, www.ivoclarvivadent.com), and Prime & Bond® NT™ (DENTSPLY Caulk, www.dentsply.com).
Self-Etch Bonding Agents
The first self-etch bonding agents were introduced in the 2000s as 6th-generation systems.3 With the use of an acidic primer as the tooth surface etchant, they eliminate the need for etching with phosphoric acid, as well as subsequent rinsing and drying. Without the phosphoric acid etching, postoperative sensitivity is lower than with the 4th- and 5th-generation total-etch bonding agents.1-3 However, dentinal bond strengths are sacrificed slightly, typically between 18 MPa and 23 MPa. While phosphoric acid is eliminated for dentinal bonding in 6th-generation systems, it continues to be used when bonding to uncut enamel.
The 6th-generation is classified into Type I and Type II. The first has a self-etching primer and a resin adhesive, which are applied in separate layers, while Type II combines the self-etching primer and adhesive to simplify bonding even further. This method of application creates an important difference between Type I and Type II: with Type I, the bonding surface is neutral in pH because the resin adhesive is applied over the acidic primer, while the Type II surface is acidic because the acidic primer and adhesive are applied as one component.
The light-cured 6th-generation Type I takes two steps, including application of separate primer and adhesive, while the dual-cured agents require three steps, mixing with a catalyst and applying primer and adhesive (Table 2). (However, for both of these, an additional first step of etching with phosphoric acid may be needed if bonding to uncut enamel.) Light-cured 6th-generation Type I bonding agents include Adper Scotchbond SE Self-Etch Adhesive, Clearfil™ SE BOND (Kuraray America, www.kuraraydental.com), Clearfil SE PROTECT (Kuraray America), FL-Bond II (SHOFU, www.shofu.com), and frog (SDI-North America, www.sdi.com.au). Examples of dual-cured 6th-generation Type I bonding agents are AdheSE® (Ivoclar Vivadent), Clearfil LINER BOND 2V (Kuraray America), Contax™ (DMG America), and Nano-Bond® (Pentron Clinical).
The Type II bonding agents are available with light-cured settings only and typically need only mixing and applying primer–adhesive to complete (Table 2). Examples of light-cured 6th-generation Type II bonding agents include Adper Prompt L-Pop Self-Etch Adhesive (3M ESPE), ALL-BOND SE® (Bisco), and Brush & Bond™ (Parkell, www.parkell.com).
Just as 5th-generation bonding agents simplified previous systems, 7th-generation bonding agents integrated 6th-generation materials into a single-bottle system. Introduced in the mid 2000s, 7th-generation self-etching bonding agents have the fewest number of steps when bonding to dentin, providing dentinal bond strengths of 18 MPa to 25 MPa. The light-cured agents require no mixing, with the application of a primer–adhesive as the only step, while dual-cured products typically require mixing with a catalyst (Table 2). (With both light-cured and dual-cured products, an additional first step of etching with phosphoric acid is used if bonding to uncut enamel.) Examples of light-cured 7th-generation bonding agents are AdheSE One F (Ivoclar Vivadent), BOND FORCE (Tokuyama Dental/Tokuyama America, www.tokuyama-us.com), Clearfil S3 BOND (Kuraray America), G-BOND (GC America, www.gcamerica.com), go! (SDI-North America), Optibond® All-In-One (Kerr), and Xeno® IV (DENTSPLY Caulk). Dual-cured 7th generation bonding agents include Clearfil DC BOND (Kuraray America), Futurabond DC (VOCO America, www.voco.com), and Xeno IV DC (DENTSPLY Caulk).
CLINICAL APPLICATIONS
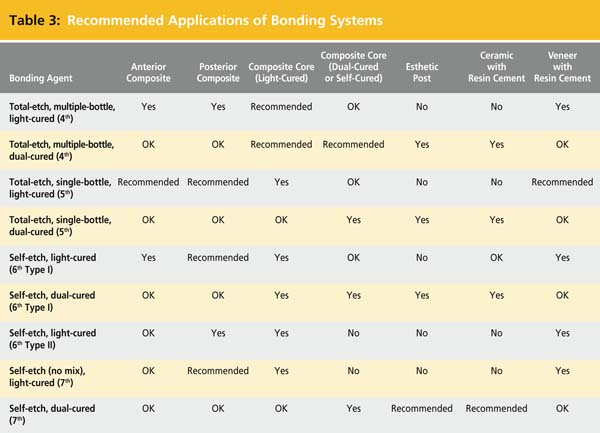
Each generation is recommended for a specific clinical application: 4th-generation systems are considered best for composite cores; 5th-generation systems are ideal for bonding of anterior and posterior composites and cementation of veneers with resin cements; 6th-generation bonding agents are recommended for bonding of posterior composites; light-cured 7th-generation bonding agents are ideal for bonding of posterior composites; and dual-cured 7th-generation bonding agents are suggested for bonding of esthetic posts and ceramic restorations with resin cement (Table 3).3
 |
COMPONENTS IN BONDING AGENTS
Etchant
To understand how an etchant works, it is important to define the smear layer, which is the layer of debris on the surface of dental tissues created by cutting a tooth. Depending on the surface preparation, the smear layer can vary in thickness, roughness, and degree of attachment to the underlying tooth structure. It must be removed, modified, or penetrated by resin to allow for bonding between the tooth and restorative material. In 4th- and 5th-generation total-etch products, the etchant used to remove the smear layer completely is phosphoric acid. In self-etch products, a primer–adhesive penetrates and re-precipitates the smear layer. Self-etching primers are acidic monomers that combine the etchant with the primer or primer–adhesive. While some acidic primers are based mainly on lower concentrations of phosphoric acid (typically 35% to 37%), some have pH levels higher than phosphoric acid.
Primer
The primer promotes good wetting of enamel and dentin.1-5 It is composed of hydrophilic monomers, usually carried in a water-soluble solvent (such as acetone, ethanol, or water) to promote good flow and penetration into hydrophilic dentin. The most extensive penetration possible is important because this influences the resulting bond strength. Self-etch bonding agents use primers that are also acidic to assist in the penetration of the smear layer; refrigeration can extend shelf life.
Adhesives
The adhesive creates the bond between enamel or dentin and resin composite restorative material or resin cement.1-5 Adhesives are mostly hydrophobic, dimethacrylate monomers that are compatible with monomers used in both the primer and the resin composite. This compatibility helps the adhesive act as the link between the hydrophilic primer and the hydrophobic resin composite. The primer–adhesives used in 7th-generation bonding agents are acidic because they must penetrate the tooth’s smear layer.
Initiator and Accelerator
Proper curing—the crosslinking of enamel or dentin and resin bonds until a solid bond is formed—is essential for providing good retention and sealing. The crosslinking reaction begins with an initiator, and an accelerator activates the initiator to promote curing at room temperature. The initiator and accelerator are required in both light- or dual-cured settings.1-5 In light-activated products, these components are typically camphorquinone and organic amine.
Filler
Fillers are submicron glass particles and nanofillers ranging from 0.5% to 40% by weight,1-5 which help to control handling. In addition, fillers may improve bonding strength and increase film thickness of the adhesive layer, which creates more of a buffer and reduces the risk of postoperative sensitivity.
Solvent
The most commonly used solvents are acetone, ethanol, and water. The solvent affects the evaporation rate:1-5 acetone evaporates quickly and requires the shortest drying time; ethanol evaporates more slowly and requires moderate drying time; and water evaporates very slowly and needs the longest drying time. The extent of dryness (promoted by the amount of air applied to the teeth with a three-way syringe) strongly influences the resultant bond strength. A somewhat moist dentin surface is needed for optimal bonding, with over-wet or over-dry conditions weakening bonds: over-wet conditions could result in water remaining in the adhesive layer, while over-drying could cause reduced penetration of adhesive, collapse of the dentin fiber network, and shrinkage of collagen fibers. One recently introduced product—Bond-1® SF Solvent Free SE Adhesive (Pentron Clinical)—is solvent-free, reportedly eliminating common technique-sensitive issues, such as under-drying or over-drying.6
Other Ingredients
Fluoride, desensitizers, and antimicrobial ingredients are also used in the process of adhesive bonding.1-5 Whether these ingredients affect bonding has not yet been demonstrated clinically.
MECHANISMS OF BONDING
Total-Etch Systems
In 4th- and 5th-generation bonding agents, application of phosphoric acid, followed by rinsing, completely removes the smear layer and plugs.1,2 The 4th-generation separate primer and adhesive or the 5th-generation primer–adhesive combination fills in the dentinal tubules and interacts with collagen fibers to form a hybrid layer.
Self-Etch Systems
Sixth- and 7th-generation bonding agents use the smear layer as a bonding substrate.3-5 The 6th-generation acidic primer or the 7th-generation primer–adhesive combination demineralizes the smear layer and the top layer of the underlying dentin surface.7 They also infiltrate collagen fibers and copolymerize, minimizing voids and potential leakage. Because the etched surface is not rinsed, the demineralized smear layer is incorporated into the hybrid layer, which is typically thicker than the hybrid layer formed with 4th- and 5th-generation systems, ranging from 0.5 μm to 5 μm.7 This somewhat thicker hybrid layer works as a buffer to minimize postoperative sensitivity.
MINIMIZING TECHNIQUE SENSITIVITY
Variations in tooth structure and contaminants can reduce the strength of bonding agents. Managing these variables minimizes technique sensitivity.
Tooth Structure
It has been established that tooth structure variations can affect adhesive bond strength. For example, in vitro bond strengths to carious tooth structure are generally lower than to noncarious tooth structure, while in vitro bond strengths to primary tooth structure are generally lower than to permanent tooth structure.8,9 Bond strengths to deep dentin can be 50% lower than bond strengths to superficial dentin.10 Application of additional layers of resin may be necessary to obtain a glossy surface and increase bond strength. Dentin prepared with an Erbium: YAG laser has no smear layer,11 and etching with phosphoric acid is not necessary. Application of self-etch bonding agents might require several layers to obtain a glossy surface.
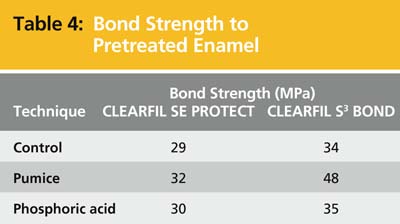
With uncut enamel, two techniques could be used to remove the enamel pellicle and prepare it for bonding: the pumice technique and the pre-etch method. Pumice can be used on uncut enamel to improve the bond strength by 3 MPa to 14 MPa, depending on the bonding product used (Table 4).12 In the pre-etch technique, phosphoric acid is applied to enamel before tooth preparation. This approach eliminates the need to etch uncut enamel and avoids possible contamination of dentin with phosphoric acid. Both techniques are effective on unrestored teeth, as well as on teeth with old amalgams that need replacement.
 |
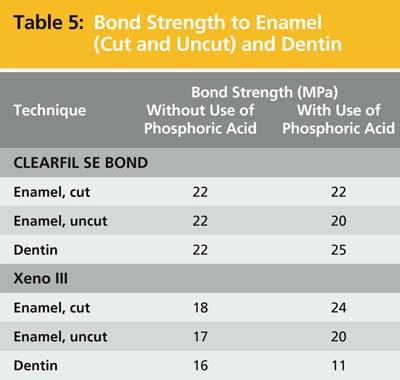
Most manufacturers of self-etching bonding agents recommend the use of phosphoric acid to etch uncut enamel before application of the self-etching primer or self-etching adhesive. Even so, there may be only a small improvement of up to 3 MPa in bond strength—or even a slight decrease in strength (Table 5). If the phosphoric acid also etches dentin, the bond strength of the self-etching adhesive to dentin may be reduced, especially with 6th-generation Type II and 7th-generation bonding agents. This reduction may occur if the self-etching adhesive fails to penetrate completely the additional demineralized dentin produced by the phosphoric acid etch. To prevent this, apply extra coats of bonding agent to obtain a shiny surface as needed.
 |
Contaminants
Many common contaminants of the tooth surface can weaken adhesive bonds. The first is water, so overly wet dentin must dry before application of the bonding agent. Saliva, blood, and plasma are other tooth surface contaminants, with blood being more detrimental to bond strength than saliva.13-16 To prevent weak bonding, rinse contaminated areas with water (and dry sufficiently) or re-etch before bonding.
Residual oxygen from home or office bleaching can also lower bond strength to dentin.1,2 Wait 1 week after bleaching before performing a bonding procedure. (Note that the color of bleached teeth may rebound during this time as the teeth rehydrate.)
Various desensitizers have also been found to lower in vitro dentinal bond strengths by more than 50%.17 In this case, opt for noneugenol temporary cements for provisional restorations, because eugenol-based materials can lower bond strength to dentin.13,14 If a eugenol-based material must be used, the tooth should be pumiced before bonding.
Residual chemicals from hemostatic agents containing ferric sulfate, aluminum chloride, or other chemicals can lower bond strength to dentin.18 To improve bond strength, rinse contaminated areas for at least 10 sec with water and dry sufficiently before bonding. Areas contaminated with ferric sulfate should be re-etched with phosphoric acid before bonding. Remineralizing agents such as CPP-ACP and NovaMin® (NovaMin Technologies, www.novamin.com) may provide stronger bonding.
BONDING TIPS
Ceramic Crowns, Inlays, and Onlays
For maximum bonding success, verify that the bonding agent is compatible with the resin cement used. Use dual-cured adhesives with opaque ceramic restorations, especially if they will only be cured once, after the restoration is placed. Light-cured adhesives can be used with opaque ceramic restorations if they are cured before the restoration is placed; however, this could create a thicker adhesive/cement layer and affect fit. Bonding agents with acetone should be used soon after dispensing.1-5
Core Materials/Fiber-Reinforced Esthetic Posts
Choosing the correct curing method is important for strong bonding of esthetic posts. Dual-cured activators are available with some 5th-generation bonding agents and should be used with self- and dual-cured resin core materials.9 Sixth-generation Type I bonding agents are generally compatible with self-cured composite cores or resin cements. The tooth is primed, the adhesive is applied, and then the composite core is placed. Sixth-generation Type II and 7th-generation bonding agents are generally not compatible with self-cured composite cores or resin cements, because the acidity of the bonding agent can interfere with the setting of the composite. Light-cured bonding agents may be difficult to activate properly for cementation of esthetic posts; in this case, the use of dual-cured bonding agents is recommended.
Posterior Composites
Controlling the evaporation of solvent is key to strong bonding of posterior composites. Most bonding agents should be used within 3 min of dispensing to minimize the effect of solvent evaporation. Carefully follow instructions on application time and the use of air to thin the adhesive and evaporate the solvent. With less volatile solvents, such as water and ethanol, more air is needed to evaporate the solvent. Another concern is that some bonding agents etch the surface of the metal matrix band, making removal difficult: this etching can be prevented by placing a separating agent (wax) on the surface of the metal band.
Veneers
The appropriate curing technique to use for optimal bonding depends on the thickness of veneers. For veneers less than 1 mm thick, a one-step light-curing technique—in which one applies the bonding agent, followed by the resin cement, the veneer, and then the light cure—is recommended.19 For veneers more than 1 mm thick, use a two-step light-curing technique, applying the bonding agent and light cure, then applying the resin cement, veneer, and light cure again. Instructions for some resin cements (such as RelyX™ Veneer [3M ESPE]) recommend the additional application of the bonding agent to the veneer without separate light curing before cementation.
CONCLUSION
The choice of an adhesive system depends on the clinical application: 4th-generation systems are recommended for bonding of composite cores; 5th-generation systems are best for bonding of anterior and posterior composites and cementation of veneers with resin cements; 6th-generation systems are suggested for bonding of posterior composites; light-cured 7th-generation systems are advised for bonding of posterior composites; and dual-cured 7th-generation bonding systems are recommended for bonding of esthetic posts and ceramic restorations with resin cement.
Bonding to enamel and dentin can be challenging because different tooth substrates and contaminants cause bonding agents to be technique sensitive and result in decreases in bond strength of as much as 50%. However, understanding the characteristics of bonding agent components and how to manage possible pitfalls in bonding can produce better results. As bonding agents improve, the dentist will also experience less technique sensitivity, while obtaining excellent bond strengths to enamel and dentin.
DISCLOSURE
The authors have a financial interest in Dental Consultants, Inc., and are editors of The Dental Advisor. They have received grant or research support from 3M ESPE, Kuraray America, and GC America.
REFERENCES
1. Powers JM, Sakaguchi R, eds. Craig’s Restorative Dental Materials. 12th ed. St. Louis, MO: Mosby Elsevier; 2006.
2. Powers JM, Wataha JC, eds. Dental Materials–Properties and Manipulation. 9th ed. St. Louis, MO: Mosby Elsevier; 2008.
3. Farah JW, Powers JM, eds. Bonding agents—2008. Dental Advisor. 2008;25(5):1-9.
4. Farah JW, Powers JM, eds. 7th-generation bonding agents. Dental Advisor. 2009;26(6):1-6.
5. Powers JM, O’Keefe KL. Update on seventh-generation bonding agents. Inside Dentistry. 2009;5(2):52-56.
6. Farah JW, Powers JM. Innovations in prevention: fluoride varnish and calcium phosphates. Dental Advisor. 2010;27(2):12.
7. Pinzon LM, Reis A, Saiz E, et al. Interfacial structure and nanomechanical properties of self-etch adhesive systems over-time [abstract]. J Dent Res. 2007;86(spec iss A):116.
8. Xie J, Flaitz CM, Hicks MJ, Powers JM. Bond strength of composite to sound and artificial carious dentin. Am J Dent. 1996;9(1):31-33.
9. Agostini FG, Kaaden C, Powers JM. Bond strength of self-etching primers to enamel and dentin of primary teeth. Pediatr Dent. 2001;23(6):481-486.
10. O’Keefe KL, Powers JM. Adhesion of resin composite core materials to dentin. Int J Prosthodont. 2001;14(5):451-456.
11. Trajtenberg CP, Pereira PNR, Powers JM. Resin bond strength and micromorphology of human teeth prepared with an Erbium: YAG laser. Trans Academy of Dental Materials. 2001;15:171.
12. O’Keefe KL, Uceda-Gomez N, Pinzon LM, Powers JM. Bond strength of self-etching adhesives to pre-treated enamel. Dental Advisor Research Report. 2005;(2):1.
13. Powers JM, Finger WJ, Xie J. Bonding of composite resin to contaminated human enamel and dentin. J Prosthodont. 1995;4(1):28-32.
14. Xie J, Powers JM, McGuckin RS. In vitro bond strength of two adhesives to enamel and dentin under normal and contaminated conditions. Dent Mater. 1993;9(5):295-299.
15. Pinzon LM, O’Keefe KL, Powers JM. Bond strength of composite with self-etching adhesives to blood-contaminated dentin [abstract]. J Dent Res. 2003;82(spec iss A):570.
16. Pinzon LM, O’Keefe KL, Powers JM. Adhesion of composite with self-etching primer to saliva-contaminated moist and dry dentin. Trans Academy of Dental Materials. 2002;16:336.
17. Li D, O’Keefe KL, Powers JM. Effect of dentin desensitizers on bond strength on deep dentin [abstract]. J Dent Res. 2000;79(spec iss A):509.
18. O’Keefe KL, Pinzon LM, Powers JM. Effect of astringent contamination on bond strength of self-etching adhesives to dentin [abstract]. J Dent Res. 2003;82(spec iss A):25.
19. Steffer MR, O’Keefe KL, Powers JM. Bonding porcelain veneers with light-cured adhesives [abstract]. J Dent Res. 2005;85(spec iss A):1824.