You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Three phases of study build on each other: (1) re-examination of the display components of the anterior teeth; (2) reminder of how they relate to each other in composition; and (3) consideration of the observer’s perspective. It may be this third phase that is most critical, and yet, most often neglected. The materials, techniques, and equipment used “today” in dentistry have evolved considerably from those we used “yesterday.” Ceramic systems and porcelain technologies have given dentists and dental technologists extraordinary tools to create artistic, colorful crowns, bridges, and veneers— but sometimes they just don’t look like “teeth.”
Recently published information insists that esthetic considerations are central to the ethical practice of dentistry and that “the dentist’s work must conform to the dental profession’s standards of teeth that are properly shaped and colored within a complete dentition and balanced with gingival and facial features.”1 The same authors warn that although the expertise of the professional alone is considered sufficient to determine if an oral health need has been met, in esthetic dentistry it is the patient’s judgment that is sufficient to determine if a result is appropriate.2 Reporting on the results of a recent American Academy of Esthetic Dentistry survey, Goldstein wrote that the psychological management of the traumatized “re-treatment patient” becomes an additional obstacle for the dentist, and that in such situations “a patient may search for stereotypical esthetics which contradicts with natural forms, colors, and harmony.”3 It is therefore essential that the dentist and his or her team clearly and accurately present, fabricate, deliver, and defend, if necessary, natural dental anatomy, composition, and dentofacial harmony to fulfill the professional obligations of dental practice and patient service. This article is designed to support the dental team to this end.
Human teeth have not changed much in the past several hundred years; dentists and dental technicians should be experts in human dental morphology. Unfortunately, the lessons learned in dental anatomy classes often are forgotten when students move into the exciting arena of clinical care. Just as condensed study notes or mnemonics are used to recall larger areas of memory data, the following comparisons and juxtapositions will attempt to reawaken forgotten lessons of the individual and collective anatomy of the anterior human dentition. Maxillary and mandibular anterior teeth are complete opposites in regard to the four essential esthetic factors. How can this really be so?
According to the first comprehensive book on esthetic dentistry, “the acceptance of treatment by the patient is made considerably easier when the prosthesis accomplishes two basic esthetic needs: the portrayal of a physiologic norm, and an actual improvement in the attractiveness of the smile and thus all related facial expressions.”4 It is essential for the esthetic dentist to communicate the importance of viewing the interrelationships of teeth, visible gum tissues, lips, and facial features together with the patient during the diagnostic and treatment-planning appointments.5 Such a process levels expectations, builds rapport, and reduces the likelihood of misunderstandings later on.
It is the arena of social interaction that truly tests the restorative dental illusion. A comfortable speaking distance between two individuals can vary, but usually this distance is no less than 12 inches from the dental composition to the observer. That is, patients must be reminded that they display only as much of their dentition as their lips allow in widest smile. The “E” sound can be used to find the seam between what might be seen and what is “backstage,” behind the curtains of lips. Again, dentists need to clarify this with patients at the consultation appointment. Certain aspects of natural dental anatomy are accentuated by the observer’s perspective, while others are hidden. These critical anatomic display components must be rendered carefully and correctly. The absence of integration of any one display component of the dentogingival complex can stand out like the proverbial “sore thumb.” The dentist and dental technologist need to understand this concept and test their restorations from these views as they are being fabricated and tried in the patient’s mouth.
The four essential esthetic factors are: (1) anterior tooth width/length; (2) bilateral symmetry; (3) the incisal edge; and (4) the incisal embrasures. The information presented is based on published parameters of dental anatomy, the author’s 30 years of clinical practice, and the teachings and publications of the late Dr. Leonard Abrams. Current research indicates that concepts like “The Golden Proportion” are not scientifically valid nor visually appreciated by dentists and lay people.6-8 Research studies do favor continued reliance on symmetrical facial proportions and recognition of natural form.9,10
ANTERIOR TOOTH WIDTH/LENGTH
The average widths and lengths of maxillary anterior teeth are listed in Table 1. The average width difference between central and lateral incisors is 2 mm. Esthetically pleasing maxillary anterior dental restorations follow this important visual distinction. Width/length ratios of maxillary incisors are most pleasing at around 78%.11 Dr. Stephen J.
The first rule of opposites: play up the size differences between maxillary incisors (within the anatomic parameters stated), and play down any width/length differences between mandibular incisors (Figure 1 through Figure 6).
BILATERAL SYMMETRY
The most highly bilaterally symmetrical tooth in the human dentition is the mandibular central incisor.13(pp23-30) The incisoform mandibular canine displays much more bilateral symmetry than its maxillary namesake. Youthful, attractive maxillary incisors and canines typically are not bilaterally symmetrical in their natural states, although dentists or dental technologists may see and render them as such. An exception would be for teeth with severely worn incisal edges. Severe wear on these edges imparts more bilateral symmetry to all incisors.
The second rule of opposites: emphasize bilateral symmetry in fabricating mandibular anterior teeth, and knowingly de-emphasize bilateral symmetry in the maxillary anterior composition (Figure 7).
THE INCISAL EDGE
The average maxillary central incisor emerges from its alveolus at 28° from the vertical plane, the lateral incisor at 26°, and the maxillary canine at 16°.13(p227) In all three teeth the coronal profile from middle third to incisal edge curves back in a lingual direction so that the incisal edge becomes invisible to the “social interaction” observer. Incisal edge display in a maxillary anterior restoration is unnatural and unattractive.
The mandibular central incisor emerges from its alveolus at 22° from vertical, the lateral incisor at 23°, and the canine at 12°.13(p228) All three teeth have the potential to function against the lingual inclines of the maxillary anterior teeth in horizontal glide movements of the mandible. In the “normal” occlusion and most therapeutic occlusal concepts, this contact results in a functional outer aspect similar to that of posterior teeth. This functional pattern defines the mandibular anterior incisal edge into a directly visible part of these teeth.13(p238) Should functional wear/attrition continue, the appearance of the mandibular anterior incisal edge may change in outline form, but it remains a constant to the observer. The display of mandibular anterior incisal edges during speech and other functional activity is an essential component of the functionally oriented, observer’s perspective, which Abrams termed “the view.”12
The third rule of opposites: in the attractive, anatomically normal anterior dental composition, the maxillary incisal edge is never on display, while the mandibular anterior incisal edge must always be seen (Figure 8 through Figure 10).
THE INCISAL EMBRASURES
The mandibular incisors characteristically erupt with a series of three small mamelon. Typically the mamelon yield to attrition very early in their functional lives and disappear. From that point on, the widest part of the mandibular incisor is its incisal edge.12 Therefore, there can be no incisal embrasures on the labial aspect of these teeth. The irregularities and individualities one sees in compositions of mandibular incisors are manifestations of lingual, not labial anatomy (Figure 11 through Figure 13). This is a natural anatomic relationship that commonly is violated when mandibular anterior dental restorations are fabricated. The result is often the unattractive “picket fence” appearance (Figure 14 and Figure 15).
Restorations that respect correct anatomic principles are simpler to make and better harmonize with the natural dentition (Figure 16 through Figure 19). The youthful human maxillary anterior dentition displays incisal embrasures on the labial aspect of all teeth. These embrasures are defined by the most incisal extent of the proximal contact point and deepen gingivally from the midline posteriorly. So, the gingival incisal embrasure between the central incisors is more incisally located than the incisal embrasure between a central and a lateral, which is more incisal than the incisal embrasure between a lateral and a canine, etc (Figure 20).
This relationship mirrors the heights of the adjacent cementoenamel junctions and alveolar crestal positions in health.13(pp252-254) The presence of severe incisal wear often distorts this relationship such that all adjacent incisal embrasures appear at an equal level. The dentist and dental technologist must decide, therefore, if they are seeking a more aged or a more youthful appearance when designing the incisal embrasure positions of the maxillary anterior dental composition (Figure 21 through Figure 24).
The fourth rule of opposites: no incisal embrasures on the labial aspect of mandibular incisors; consistent and varying incisal embrasures as a natural display component of maxillary incisor teeth.
CONCLUSION
Often dentists and dental technologists tend to follow the same formulae when shaping and composing maxillary and mandibular anterior teeth. This article has argued that, in anatomic fact, maxillary and mandibular incisors show some key opposite characteristics when displayed in naturally esthetic compositions. Visual and morphological evidence was presented for four areas of consideration: (1) anterior tooth widths and lengths; (2) bilateral symmetry; (3) incisal edges; and (4) incisal embrasures.
ACKNOWLEDGMENT
Special appreciation to Dr. Arnold S. Weisgold for his guidance and encouragement to publish this work.
REFERENCES
1. Patthoff D, Ozar D. Esthetics and ethical care—a look at the central values of dental practice. AGD Impact. 2007;35(7):40-43.
2. Patthoff D, Ozar D. Need vs. desire—professional judgment in esthetics. AGD Impact. 2007;35(8):32-35.
3. Goldstein RE. Attitudes and problems faced by both patients and dentists in esthetic dentistry today: an AAED membership survey. J Esthet Restor Dent. 2007;19(3):164-170.
4. Goldstein RE. Esthetics in Dentistry.
5. Goldstein RE. Change Your Smile.
6.
7. Rosenstiel SF, Ward DH, Rashid RG. Dentists’ preferences of anterior tooth proportion—a web-based study. J Prosthodont. 2000;9(3):123-136.
8. Hasanreisoglu U, Berksun S,
9. Naini FB, Moss JP, Gill DS. The enigma of facial beauty: esthetics, proportions, deformity, and controversy. Am J Orthod Dentofacial Orthop. 2006;130(3):277-282.
10. Gomes VL, Goncalves LC, Do Prado CJ, et al. Correlation between facial measurements and the mesiodistal width of the maxillary anterior teeth. J Esthet Restor Dent. 2006;18(4):196-205.
11.
12. Abrams L, Presser FD. “The view” and the canine connection: an atlas of mandibular anterior tooth esthetics. J Esthet Dent. 1998;10(3):104-120.
13. Kraus BS,
14. Greenberg J. The metal band—acrylic provisional restoration featuring ultra thin stainless steel bands. Compend Contin Educ Dent. 1981;2(1):7-11.
About the Author:
Joseph R. Greenberg, DMD: Clinical Professor of Restorative Dentistry, The Kornberg School of Dentistry, Temple University; Clinical Professor of Periodontics, The University of Pennsylvania, School of Dental Medicine, Philadelphia, Pennsylvania
| Figure 1 The patient presented with two missing mandibular central incisors, after completing orthodontic treatment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|  Figure 19 Smile view of the provisional restorations. Figure 19 Smile view of the provisional restorations. |
|
|
|  Figure 22 Figure 22 |
|  Figure 24 Figure 24 |

 Figure 2 The resin-bonded restoration for this patient used one pontic. This visual effect was successful because of the basic similarities in width and length of the mandibular anterior group of teeth. It is not one tooth that appears to be two—it is five teeth that appear as six (dental laboratory technology by daVinci Dental Studios,
Figure 2 The resin-bonded restoration for this patient used one pontic. This visual effect was successful because of the basic similarities in width and length of the mandibular anterior group of teeth. It is not one tooth that appears to be two—it is five teeth that appear as six (dental laboratory technology by daVinci Dental Studios,  Figure 3 The patient presented with a failing, full-coverage fixed dental prosthesis from the maxillary right canine to the maxillary left canine. The width of the lateral incisors was very similar to the adjacent central incisors. The overall effect was unnatural. There were also considerable gingival margin height disparities.
Figure 3 The patient presented with a failing, full-coverage fixed dental prosthesis from the maxillary right canine to the maxillary left canine. The width of the lateral incisors was very similar to the adjacent central incisors. The overall effect was unnatural. There were also considerable gingival margin height disparities. Figure 4 The patient’s full smile showed a lip aperture that limits the esthetic display to the coronal aspects of these teeth, and therefore, the treatment plan focused on correcting the width–length discrepancies of the crowns, not the gingival margin height disparities nor the issues of root exposure.
Figure 4 The patient’s full smile showed a lip aperture that limits the esthetic display to the coronal aspects of these teeth, and therefore, the treatment plan focused on correcting the width–length discrepancies of the crowns, not the gingival margin height disparities nor the issues of root exposure. Figure 5 The treatment included expansion of each central incisor pontic and reduction in width of the lateral incisor crowns so that natural appearing width–length proportions (1.5 mm to 2 mm width differences) could be re-established.
Figure 5 The treatment included expansion of each central incisor pontic and reduction in width of the lateral incisor crowns so that natural appearing width–length proportions (1.5 mm to 2 mm width differences) could be re-established. Figure 6 Postoperative smile view (dental laboratory technology by Jonathan Lee, Dental Ceramic Arts,
Figure 6 Postoperative smile view (dental laboratory technology by Jonathan Lee, Dental Ceramic Arts,  Figure 7 The bilateral symmetry of the mandibular central incisor (reprinted with permission. Kraus et al13).
Figure 7 The bilateral symmetry of the mandibular central incisor (reprinted with permission. Kraus et al13).
 Figure 9 Diagram of a simulated observer’s perspective on the maxillary and mandibular anterior teeth.
Figure 9 Diagram of a simulated observer’s perspective on the maxillary and mandibular anterior teeth. Figure 10 Diagram illustrating the natural appearance of the mandibular anterior incisal edges from the observer’s perspective.
Figure 10 Diagram illustrating the natural appearance of the mandibular anterior incisal edges from the observer’s perspective. Figure 11 Diagrammatic representation of an anatomically correct incisal embrasure configuration for six mandibular anterior teeth. Note that this is a “lab bench” view (teeth positioned vertically upright) not a functional view.
Figure 11 Diagrammatic representation of an anatomically correct incisal embrasure configuration for six mandibular anterior teeth. Note that this is a “lab bench” view (teeth positioned vertically upright) not a functional view. Figure 12 The patient demonstrates the functionally oriented, observer’s perspective known as “the view.” The apparent separations and irregularities are a function of lingual, not labial anatomy.
Figure 12 The patient demonstrates the functionally oriented, observer’s perspective known as “the view.” The apparent separations and irregularities are a function of lingual, not labial anatomy. Figure 13 The patient in Figure 12 has tipped her head back until all lingual anatomical components become hidden from sight, thus proving the absence of incisal embrasures on the labial aspect.
Figure 13 The patient in Figure 12 has tipped her head back until all lingual anatomical components become hidden from sight, thus proving the absence of incisal embrasures on the labial aspect. Figure 14 and Figure 15 A mandibular anterior dental restoration with an incorrectly placed incisal embrasure between the left central and lateral incisors, known as the “picket fence” appearance. A retracted view of the same patient reveals a two-unit, fixed, implant-supported restoration fabricated with great skill in many other aspects.
Figure 14 and Figure 15 A mandibular anterior dental restoration with an incorrectly placed incisal embrasure between the left central and lateral incisors, known as the “picket fence” appearance. A retracted view of the same patient reveals a two-unit, fixed, implant-supported restoration fabricated with great skill in many other aspects. Figure 15
Figure 15 Figure 16 The patient presented with mandibular left central and lateral incisors with compromised root support in the region of the cementoenamel junction. The treatment plan was for splinted dental crowns.
Figure 16 The patient presented with mandibular left central and lateral incisors with compromised root support in the region of the cementoenamel junction. The treatment plan was for splinted dental crowns. Figure 17 The final preparations.
Figure 17 The final preparations. Figure 18 The block-carved steel band/acrylic provisional restorations.14 These restorations were carved easily, creating bilaterally symmetrical forms of equal width. No gingival embrasure was made on the labial aspect. Special attention to detail was given to the incisal edges, so they would match the adjacent teeth.
Figure 18 The block-carved steel band/acrylic provisional restorations.14 These restorations were carved easily, creating bilaterally symmetrical forms of equal width. No gingival embrasure was made on the labial aspect. Special attention to detail was given to the incisal edges, so they would match the adjacent teeth.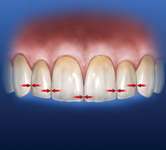 Figure 20 Diagram illustrating the natural anatomical position and progression of incisal embrasures on youthful, intact maxillary anterior teeth.
Figure 20 Diagram illustrating the natural anatomical position and progression of incisal embrasures on youthful, intact maxillary anterior teeth. Figure 21 and Figure 22 Full smile view and retracted view of a patient whose maxillary dentition displays a reverse incisal embrasure pattern and a concave, unattractive incisal edge line. The treatment plan was to place a new crown for the right lateral incisor, porcelain laminate veneers for the right canine and other incisors, and a porcelain laminate veneer to cover an existing porcelain-fused-to-metal abutment crown for the left canine.
Figure 21 and Figure 22 Full smile view and retracted view of a patient whose maxillary dentition displays a reverse incisal embrasure pattern and a concave, unattractive incisal edge line. The treatment plan was to place a new crown for the right lateral incisor, porcelain laminate veneers for the right canine and other incisors, and a porcelain laminate veneer to cover an existing porcelain-fused-to-metal abutment crown for the left canine. Figure 23 and Figure 24 The final restorations were designed to recreate an embrasure form and flow as diagrammed in Figure 20. A convex incisal edge line was created (dental laboratory technology by Shin at Tanaka Dental,
Figure 23 and Figure 24 The final restorations were designed to recreate an embrasure form and flow as diagrammed in Figure 20. A convex incisal edge line was created (dental laboratory technology by Shin at Tanaka Dental,
| Cervicoincisal Length of Root (mm) | Mesiodistal Mesiodistal Length of Crown (mm) | Crown Diameter (mm) | Cervical Diameter (mm) | |
| Central Incisor | 10.5 | 13 | 8.5 | 7 |
| Lateral Incisor | 9 | 13 | 6.5 | 5 |
| Canine | 10 | 17 | 7.5 | 5.5 |
Wheeler RC. Wheeler’s Dental Anatomy, Physiology, and Occlusion. 6th ed.
| Cervicoincisal Length of Root (mm) | Mesiodistal Mesiodistal Length of Crown (mm) | Crown Diameter (mm) | Cervical Diameter (mm) | |
| Central Incisor | 9 | 12.5 | 5 | 3.5 |
| Lateral Incisor | 9.5 | 14 | 5.5 | 4 |
| Canine | 11 | 16 | 7 | 5.5 |
| First Premolar | 8.5 | 14 | 7 | 5 |