You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Digital dental technologies have undergone monumental changes since the 1980s-a time when the Apple Lisa, the Compaq, and the CD-ROM were first introduced to the general public (Figure 1). At the same time that these digital innovations were just beginning to make their mark, most dental practices had not yet been influenced by the burgeoning technologies and were still in the "age of amalgam, gold foil, and gold onlays." Brånemark was just coming on the scene with dental implants, and composite technology was in its early stages.
Where once digital dentistry comprised a difficult mixture of standalone or poorly integrated technologies, today as clinical dentists we have at our command an array of digital diagnostic and treatment tools that can be combined to fulfill the promise of technology for patient care.
As technology continues to advance, so too does the field of dentistry. In 2023, there are many technological breakthroughs that are revolutionizing the way that dental procedures are performed, making treatment more efficient, more accurate, and less invasive.1 Incorporating advanced digital technologies into dental practice yields many significant benefits:
· improved treatment planning and diagnostic outcomes
· increased efficiency
· better precision and predictability
· practices are helped to stand out in a competitive landscape
· superior diagnostic ability
· superior ability to treatment plan
· improved patient comfort and convenience
· enhanced patient compliance
· time savings
· cost savings
· consistent quality and esthetics of restorations
· control over the entire process
· patient education
As a starting point in understanding the value of a specific technology for the dental practice, as well as how to incorporate advanced technology into the practice, we must first understand: 1) how practices gather and use information,2 and 2) how practices make decisions about implementing and using technology in practice.3
Because technology is advancing so rapidly, clinicians must remain continually aware of the technology marketplace in order for their practice to keep up with the many changes. How a dental practice gathers, manages, and uses information about the technology sector-and how clinicians incorporate and master advanced digital dentistry technologies-will likely help determine the success or failure of the practice.
This article will discuss the use of digital technologies as an integral part of a daily workflow in the general dental practice, highlighting the use of the following:
· 2D digital intraoral cameras
· 2D digital radiographic imaging
· 3D cone-beam computed tomographic (CBCT) imaging
· intraoral and extraoral computer-aided design (CAD) scanners
· computer-aided manufacturing (CAM) milling devices
· 3D digital printers
· integrated imaging and implant planning software
DIAGNOSIS AND TREATMENT PLANNING
Diagnosis and treatment planning are the foundation of successful dental treatment. An accurate and correct diagnosis is necessary not only for clinicians to determine the optimal treatment plan, but also for patients to be empowered to make fully informed decisions regarding their care. In dentistry, diagnostic assessment involves evaluation of the hard and soft oral tissues, history taking (patient-reported symptoms and the medical history), imaging studies (intraoral and extra oral photographs and scans and radiographic imaging), diagnostic testing, and a myriad of other clinical data that must be gathered and evaluated. The variety of oral pathologies is extensive-ranging from cancerous lesions, oral abscesses, occlusal pathology, and traumatic oral injuries, to periodontitis, to name just a few-and diagnosis decision making can be a daunting undertaking for dental clinicians. Today, however, advanced digital technologies can be utilized to provide the practitioner with superior and accurate information for working through wide-ranging differential diagnoses.
Often the dental hygiene department is at the forefront of the examination and treatment planning process, serving as the portal through which new patients, recare patients, consultations, and emergency visits flow on a daily basis. It has been estimated that a dental practice's dental hygiene department generates 25% to 35% of gross revenue.4 Dental hygienists typically create the new patient's first impression of a practice, and have a great influence on return visits and thus on the future of the dental practice. In a typical day of a dental practice that utilizes a digital workflow, the dental hygiene department will see several new patients.
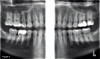
Intraoral photographs should be taken and shared with the patient during the visit to help them understand the conditions in their mouth and why treatment may be necessary (eg, an asymptomatic tooth with a large fracture that will require a crown) (Figure 2). Next, a full-mouth series of digital radiographs are taken; surprisingly, there are still patients who are unfamiliar with this technology, which yields instant access to these 2D images and utilizes software that can clarify important areas of interest (Figure 3 and Figure 4). Digital imaging is commonly used for the evaluation of dental emergencies, where a thorough and accurate diagnosis is essential for rapid treatment planning (Figure 5).
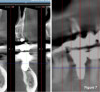
With the introduction of CBCT imaging, a higher level of visualization and accuracy is now possible (Figure 6 and Figure 7). Because CBCT allows an area of interest to be accurately viewed in three dimensions, it has fundamentally changed dental diagnosis and treatment planning since its entrance into dentistry in 2001."5,6 As demonstrated in Figure 6 and Figure 7, there is a significant difference between what can be viewed in two versus three dimensions, which accounts for CBCT's greater diagnostic precision.
In the literature, there has been ample discussion regarding the use of CBCT as a new standard of care in dental diagnostics.7,8 Today, CBCT imaging yields a great amount of diagnostic data, while it also has low radiation loads comparable to a full series of digital radiographs9 (Figure 8).
A digital dental practice routinely uses CBCT for the evaluation of a variety of dental emergencies, such as trauma (Figure 9).
CBCT is now also commonly used in dental treatment planning, having numerous applications, and is quickly becoming the standard of care for the following:
· surgical planning for impacted teeth
· diagnosis of temporomandibular joint disorders
· accurate placement of dental implants
· evaluation of the jaw, sinuses, nerve canals, and nasal cavity
· detecting, measuring, and treating jaw tumors
· determining bone structure and tooth orientation
· locating the origin of pain or pathology
· cephalometric analysis
· reconstructive surgery10
For dental implant consultations, CBCT imaging accurately shows the height and width of bone, along with the surrounding tooth structure, and allows for accurate treatment planning using various digital software tools (Figure 10). The CBCT scan is used to fabricate a surgical guide to facilitate implant placement. These surgical guides are designed using surgical guide design software and are easily fabricated, and when designed and used properly, they improve the accuracy of implant placement and increase the predictability of treatment outcomes11 (Figure 11). (See "Implant Placement" section below.)
USE OF DIGITAL TECHNOLOGIES IN DENTAL TREATMENTS
CAD/CAM
Dental practices that use digital workflows routinely employ CAD technology for restorative dentistry, including implant therapy. The scanners available today can provide intraoral imaging of quadrants and full arches for a full range of dental procedures. CAM allows practices to mill crowns and small bridges in a variety of durable materials. Additionally, 3D printers can quickly and efficiently produce provisional single- and multi-unit restorations and removable dental prostheses in the office. New materials are also emerging that promise to allow in-office printing of permanent restorations.12
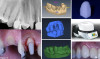
In the following case, a male patient presented for an emergency visit with a large carious lesion and reported experiencing tooth sensitivity to cold stimuli. He was adamant that his dental problem be resolved that same day. No infection was present. After a discussion of the options with the patient and with his consent, a decision was made to perform root canal therapy, use a diode laser to perform a soft tissue gingivectomy, place a direct post and core, and fabricate a lithium disilicate crown, all in a single visit. The entire treatment was completed in 3.25 hours, and the patient was satisfied with the results. In this case, using CAD/CAM, a crown was milled in-office and delivered to the patient on the same day (Figure 12). The clinical success of teeth restored with crowns designed and milled using CAD/CAM technology is well-documented.13
CAD/CAM for the fabrication of restorations is commonly performed several times daily in a digital dental practice. Restorations produced using CAD/CAM can range from simple single crowns to more advanced, multi-unit restorations. In the following case, a 45-year-old male patient presented with unesthetic anterior teeth that he expressed needed to be "immediately" restored in order for him to attend an important upcoming event. He presented with worn, malposed anterior teeth with recurrent caries on existing composites. Teeth Nos. 7 to 10 were prepared, veneers were designed and milled, and the restorations were stained, characterized, glazed, and seated. The case required only 2 hours of chairtime and 2 hours of lab time by a dental assistant (Figure 13). Monolithic laminate veneers, such as those used in this patient, can be made from any of a variety of ceramic materials using CAD/CAM; CAD/CAM-manufactured veneers have been found to be reliable under stress14and provide an excellent alternative to laboratory fabrication methods.
Implant Placement
With proper training, the digital dental practice can place and restore dental implants routinely and consistently. CBCT imaging is used for diagnosis and treatment planning for implant surgery cases. With this technology, implants are placed virtually using implant planning software.15 After having completed numerous cases following this workflow, the author finds this workflow is applicable for both the placement of single implants and for implant therapy in edentulous patients. For a single implant, the surgical guide is printed in-house with resin in a digital printer. Following implant integration, the implant is restored; the implant is scanned intraorally, and CAD/CAM can be used to fabricate a milled crown on either a stock abutment or a laboratory-fabricated custom abutment.
In the case shown in Figure 14, CBCT allowed for implant selection and planning, and the CBCT surgical guide enabled execution of flapless surgery and placement of the implant. Practices with software capability can image scan bodies and design and mill in-office, in contrast to dental practices that utilize a conventional workflow (Figure 15).
Orthodonticsand Prosthodontics
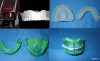
Digital treatment planning for malocclusion and fabrication of occlusal guards and orthodontic aligners are additional routine capabilities of a digital dental practice. The practice may adopt an in-office process that combines both analog and digital technologies in the workflow. The practice may fabricate the occlusal guards or aligner in-house or may choose to send the intraoral scans to a laboratory for the fabrication process17,18(Figure 16).
Digital denture fabricationhas a simplified workflow that allows for variations depending on the practice's needs and abilities. At its simplest, digital fabrication of a denture involves obtaining a CBCT scan of an existing denture, and with software and a printer, creating a resin denture duplicate, which is then used as an impression and bite tray for conventional processing (Figure 17). For fabrication of a denture that is not a duplicate denture, a more involved approach is necessary that includes obtaining intraoral scans of the arches and bite registration, software design, tooth selection virtually or physically, and in-office printing (or laboratory fabrication) of the denture19 (Figure 18).
OVERCOMING BARRIERS TO ADOPTION OF DIGITAL TECHNOLOGIES
Dental practitioners' acceptance of digital technologies is influenced by many factors. Practitioners who are fully educated on the benefits are more likely to incorporate digital dentistry into their practice; however, for some dental practices, adopting digital technologies can be problematic. Three common obstacles to utilizing digital workflows are 1) lack of perceived need for advanced dental technology; 2) the learning curve needed to use the digital tools; and 3) the high cost of investing in the technologies.
As we have shown, the benefits of digital technology in dentistry are easily acknowledged. Learning curves can be managed by appropriate education and training; the practitioners themselves must devote the time necessary to mastering the new technologies, and they must be disciplined and willing to learn. Objections about the costs involved need to be considered in terms of ROI. Although the initial investment may be costly, in the long run incorporation of advanced technology will positively impact a practice's bottom line.20 Incorporating digital technology into the dental practice is not a question of feeling compelled to do a procedure from beginning to end completely digitally.An example of this is the previously described approach to denture fabrication which combines both digital and traditional techniques. Digital dentistry technology allows substantial cost savings and many avenues for achieving optimal results, from a workflow that utilizes both in-office scanning and lab fabrication to a complete in-office digital workflow21(Figure 19 and Figure 20).
CONCLUSION
In the past, while standalone digital technologies held great potential for revolutionizing dentistry, they could be challenging to incorporate into everyday dental practice. Today, digital dentistry has become fully accessible to general dental practices, as integrated digital workflows have evolved to ensure seamless processes. Digital technologies can now be implemented in general dental practices as an integral part of a daily workflow, and as such are instrumental in new patient visits, recare visits, consultations, and emergency care. Digital dentistry offers greater diagnostic accuracy and improved treatment planning and has helped ensure increased efficiency and predictability for many dental treatments, including implant placement. Changes continue to occur rapidly occurring with digital technology, with robotics and artificial intelligence poised to act as disrupters in clinical dentistry.22-24For the practitioner who is motivated to stay up-to-date on technologic advances, digital dentistry can be fully integrated into daily general dental practice, providing numerous enhancements to patient care and practice profitability.
References
1. Top 5 Technological Innovations in Dentistry in 2023. Dentistry Today. https://www.dentistrytoday.com/top-5-technological-innovations-in-dentistry-in-2023/. Published March 30, 2023. Accessed June 16, 2023.
2. Gates B, Hemingway C. Business @ the Speed of Thought: Succeeding in the Digital Economy. Penguin Books; 2000.
3. Sloan AP Jr. My Years With General Motors. New York, NY: Doubleday & Co.; 1964.
4. Watterson DG. The successful hygiene department: understanding the numbers. Dental Economics website. http://www.dentaleconomics.com/articles/print/volume-105/issue-7/practice/the-successful-hygiene-department-understanding-the-numbers.html. Published July 15, 2015. Accessed June 16, 2023.
5. Lark MR. Cone beam technology: a brief technical overview. Dental Economics website. https://www.dentaleconomics.com/science-tech/diagnostic-imaging-and-cbct/article/16387498/cone-beam-technology-a-brief-technical-overview. Published August 1, 2008. Accessed June 16, 2023.
6. Hatcher DC. Operational principles for cone-beam computed tomography. J Am Dent Assoc. 2010;141(Suppl 3):3S-6S.
7. Peters CI, Peters OA. CBCT: the new standard of care? American Association of Endodontists website. https://www.aae.org/specialty/cbct-new-standard-care/. Published April 3, 2018. Accessed June 16, 2023.
8. Dentistry, the law, and CBCT. Dental Economics website. https://www.dentaleconomics.com/science-tech/article/16388106/dentistry-the-law-and-cbct. Published October 26, 2016. Accessed June 16,2023.
9. Ludlow JA, Timothy R, Walker CK, et al. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac Radiol. 2015;44(1):20140197.
10. Dental Cone Beam CT. Radiology Info.org website. https://www.radiologyinfo.org/en/info/dentalconect. Updated April 15, 2022. Accessed June 16, 2023.
11. Trobough KP, Garrett PW. Surgical guide techniques for dental implant placement. Decisions in Dentistry. https://decisionsindentistry.com/article/surgical-guide-techniques-for-dental-implant-placement/. Published July 24, 2018. Accessed June 16, 2023.
12. Chi J. Digital impressions and in-office CAD/CAM: a review of best practices and what's to come. Compend Contin Educ Dent. 2021;42(3):140-141.
13. Brandt S, Winter A, Lauer H, Kollmar F, Portscher-Kim S-J, Romanos GE. IPS e.max for all-ceramic restorations: clinical survival and success rates of full-coverage crowns and fixed partial dentures. Materials (Basel). 2019;12(3):462.
14. Romanini-Junior JC, Hirata R, Bonfante EA, et al. Monolithic CAD/CAM laminate veneers: reliability and failure modes. Dent Mater. 2020;36(6):724-732.
15. Alqallaf H, Su F-Y, Goel A, Lin W-S. Utilizing a digital workflow for implant treatment planning. Decisions in Dentistry. https://decisionsindentistry.com/article/utilizing-digital-workflow-implant-treatment/. Published May 14, 2021. Accessed June 16, 2023.
16. Storelli S, Palandrani G, Amorfini L. A digital workflow for computer-guided implant surgery integrating CBCT, model scanning, and CAD/CAM for a complete edentulism implant-supported prosthesis: a technique procedure. Int J Comput Dent. 2020;23(3):269-279.
17. Scherer M. Working with KeySplint Soft 3D printed occlusal guards. LearnDentistry™ website. https://learndentistry.com/3d-printed-occlusal-guards/. Accessed June 16, 2023.
18. Tozlu M, Özdemir F. In-house aligners: why we should fabricate aligners in our clinics? Turk J Orthod.2021;34(3):199-201.
19. Lee H-J, Jeon J, Moon HS, Oh KC. Digital workflow to fabricate complete dentures for edentulous patients using a reversing and superimposing technique. Appl Sci. 2021;11(13):5786.
20. Advanced dental technology: don't get left behind. Dental Economics website. https://www.dentaleconomics.com/practice/article/16391066/advanced-dental-technology-dont-get-left-behind. Published September 1, 2006. Accessed June 16, 2023.
21. Rosen A. Leveraging technology for productivity and best outcomes. Dentistry Today. https://www.dentistrytoday.com/leveraging-technology-for-productivity-and-best-outcomes/. Published April 1, 2015. Accessed June 16, 2023.
22. Ahmad P, Alam MK, Aldajani A, et al. Dental robotics: a disruptive technology. Sensors.2021;21(10):3308.
23. Agrawal P, Nikhade P. Artificial intelligence in dentistry: past, present, and future. Cureus. 2022;14(7):e27405.
24. Nguyen T, Larrivée N, Lee A, Bilaniuk O, Durand R. Use of artificial intelligence in dentistry: current clinical trends and research advances. J Can Den Assoc. 2021;87:L7.