You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
According to a survey of the American Academy of Cosmetic Dentistry, an overwhelming majority (99.7%) of US adults believe that an attractive smile is a significant social asset, with "whiteness of teeth" ranking among the top attributes of an esthetically pleasing smile.1 The high value placed on dental esthetics, together with the general public's heightened awareness of and desire for cosmetic dental procedures, has in recent decades led to an increasing demand for teeth-whitening treatments. To address this need, the dental industry has flooded the market with a wide variety of teeth-whitening products-including over-the-counter toothpastes, gels, strips, and trays, as well as products and treatments administered by dental professionals, such as take-home trays and in-office systems-targeting both consumers and clinicians. The process of chemically bleaching the teeth continues to have appeal for most patients because it is minimally invasive and more affordable than other cosmetic alternatives, such as direct adhesive restorations or porcelain laminate veneers.
Most dental whitening products contain either hydrogen peroxide or carbamide peroxide gel as the primary agent, which is applied directly to the teeth. Carbamide peroxide, also known as urea peroxide, was first described with great enthusiasm in the medical literature more than 100 years ago, when it was used for its disinfectant properties and remarkable therapeutic ability to promote wound healing.2 In 1957, a 10% carbamide peroxide concentration was first made available as an over-the-counter oral antiseptic aqueous solution called "Gly-Oxide" (personal communications with Prestige Consumer Healthcare Inc., Tarrytown, NY; August 2022). The oral health benefits and safety of this 10% formulation have been demonstrated in the treatment of candidiasis/thrush in infants,3 the prevention of caries in elderly adults suffering from xerostomia,4 and the prevention of caries in children when it is applied daily throughout orthodontic therapy.5In 1968, Dr. Bill Klusmeier, an orthodontist, noticed that his patients who utilized Gly-Oxide in their retainers at night exhibited marked improvements to their gingival health and also experienced a lightening effect on their overall tooth shade.6,7 This discovery provided the impetus for the development of an easier-to-apply, slow-release 10% carbamide peroxide gel, and the initial publication of take-home tooth whitening protocols.8 Today, in-office and at-home bleaching products are a multi-billion dollar industry, and represent the most popular treatments available to improve oral esthetics.
While the overwhelming focus of marketing for bleaching products centers around enhancing dental esthetics, it is noteworthy that whitening of the teeth represents a formerly off-label use and an unintended byproduct of the original indications for hydrogen peroxide and carbamide peroxide-namely, antisepsis and oral hygiene. A variety of different products are available for at-home use of 10% carbamide peroxide (eg, Pola Night, SDI; Opalescence™ 10%, Ultradent; and Philips® Zoom NiteWhite 10% carbamide peroxide, Koninklijke Philips N.V.). In this article, we examine the use of 10% carbamide peroxide across a broad spectrum of dental specialties and a variety of clinical scenarios (including teeth whitening and oral hygiene in pediatric and orthodontic patients, whitening of a nonvital tooth, reduction of bioburden around endosseous implants, and after oral surgery), highlighting its diverse applications in unexpected contexts that leverage the benefits of 10% carbamide peroxide bleaching agents, both as a means of augmenting dental esthetics and as an important adjunct to oral hygiene practices.
PEDIATRIC DENTISTRY
Vital teeth bleaching for adolescent patients, with or without orthodontic appliances, has not been detailed in the literature as extensively as it has been for adults. Common reservations that practitioners have regarding teeth-bleaching procedures for children include the rationale for bleaching, the most appropriate age to begin teeth-whitening treatment, and safety concerns.
Studies report that children as young as 4 years old are aware of perceived esthetic differences in tooth shade, which could result in feelings of self-consciousness, low self-esteem, and avoidance of smiling or socializing in those with discolored teeth.9-11 It is therefore prudent to consider the emotional and psychosocial effects associated with not treating or with delaying intervention for tooth discoloration in adolescents.12,13 Safe and appropriate procedures to lighten the shade of permanent dentition may mitigate or prevent bullying and associated mental health conditions.14
Treatment should always be preceded by an individual assessment to determine whether a patient is a good candidate for teeth-whitening treatment (Figure 1). A thorough patient examination should include pretreatment radiographs to assess for caries and whether the permanent dentition is present. Once it has been determined that there are no obvious contraindications for a particular individual, vital teeth bleaching may be considered for adolescent patients ranging in age from 10 to 14 years (ie, those in whom the permanent teeth are present).15
The most frequently cited safety concerns for teeth-bleaching procedures in adolescents are gingival irritation and sensitivity.16Although it has been hypothesized that the proportionally larger pulp complexes in adolescents compared with adults increases the risk for tooth sensitivity during teeth-bleaching procedures, clinical studies have invalidated this hypothesis.17 At-home use of 10% carbamide peroxide in customized, vacuum-formed bleaching trays for at least 2 hours per day or overnight with adult supervision has consistently remained the recommended teeth-bleaching protocol for patients younger than age 18 years (Figure 2). The overnight contact (ie, for up to 10 hours) of the carbamide peroxide with the gingival tissues provides a tremendous oral hygiene benefit in this patient population.18 Beyond the compelling evidence for improved hygiene with continued use of 10% carbamide peroxide, the breakdown of 10% carbamide peroxide intraorally results in urea as a byproduct and contributes significantly to beneficial cariostatic and antibacterial effects.19,20
Concerns, however, from parents and practitioners alike regarding potential chemical burns to the delicate gingiva and oral mucosa have been raised.21 Most of the discomfort and irritation from at-home teeth-bleaching has been shown to be a result of the tray fit rather than the chemical properties of treatment.6,8Custom-fit trays have traditionally been fabricated with built-in bleaching gel reservoirs (developed by adding resin to the cast impressions) 22,23 (Figure 3) and a scalloped gingival margin (Figure 4). However, the sharp and jagged edges of this design, compared with a nonscalloped tray), may be uncomfortable to some patients, leading to reduced compliance,21 and the use of reservoirs has not demonstrated an improvement in the shade of the teeth and has also been shown to result in higher rates and intensity of gingival irritation.23
ORTHODONTICS
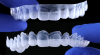
Clear aligner therapy, and to a lesser extent conventional bonded brackets and archwires, are routine orthodontic treatments for many adolescent patients. Both modalities possess potential drawbacks to optimal oral health. Aligners, for example, rely on the use of composite resin attachments, or "buttons," to aid in the movement of the teeth (Figure 5). These attachments are porous and usually possess an irregular shape, which may adversely affect the patient's oral hygiene. When used in combination with 10% carbamide peroxide gel, the aligners serve as a well-adapted custom-fit tray (Figure 6).24 For the patient younger than age 18 years, carbamide peroxide is also an ideal bleaching agent because of the antibacterial properties and beneficial cario- static effects that the urea byproduct has on gingival health scores.20 In order to achieve the maximum oral health benefits, the aligners containing the whitening gel should ideally be worn overnight or for up to 10 hours.18
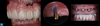
A common concern for patients who utilize teeth-bleaching products during aligner treatment is the potential for discoloration or yellowing of the tooth structure under the adhesively bonded component that was not in contact with the bleaching agent.25 However, numerous studies, as well as the author's own clinical experience, have demonstrated that the permeability of the dental hard tissues and the capillary action of peroxides allows complete penetration and diffusion of the bleaching medium under any existing resin buttons, brackets, or composite restorations (Figure 7 through Figure 9).26,27
For patients undergoing traditional ortho- dontic therapy, brackets and archwire often create food traps that have a negative impact on gingival health. Providing custom vacuum-formed whitening trays for these patients often requires making alginate impressions over the intricate dental attachments, an impractical process with inaccurate results.20 A preformed silicone mouthpiece may be a more immediate and economical solution to aid in oral hygiene around difficult-to-clean orthodontic hardware, as well as provides a vehicle for teeth whitening.
ENDODONTICS
Discoloration of the permanent maxillary anterior dentition poses a significant esthetic and cosmetic concern for many individuals, with the maxillary central incisors being the most commonly affected teeth.28 The etiology of tooth discoloration is frequently a multifactorial phenomenon and may be caused by a combination of necrosis of the pulpal tissues related to trauma, loss of vitality, incomplete extirpation of the pulp horns, and various restorative materials/procedures.29-32
For clinical situations involving a nonvital and discolored natural tooth (Figure 10), intracoronal bleaching, also known as the "walking bleach" technique, has been consistently shown to be a conservative treatment option compared with more aggressive direct/indirect restorative procedures such as composite bonding, porcelain laminate veneers, or full coverage crowns.33Additionally, for patients requesting the lightening of a single dark tooth, internal bleaching is often more cost-effective and less dependent on patient compliance than the daily use of a whitening tray. Contemporary protocols often include the use of strong oxygen-releasing chemical compounds, such as 30% to 35% hydrogen peroxide, which have been associated with adverse complications including external invasive cervical root resorption.34,35 The evaluation and outcomes of endodontic techniques utilizing a safer 10% carbamide peroxide formulation are well-documented in the literature and clinically, and have proved to be a reliable, predictable option for the internal bleaching of nonvital discolored teeth (Figure 11).36-38
When a patient presents with previously restored nonvital anterior teeth (Figure 12), the challenge to produce a satisfactory esthetic outcome becomes a collaborative effort shared between the clinician and the dental labora-tory team. The darkened stumpf and subgingival root structure may produce an unfavorable shade to any definitive translucent ceramic restoration. In addition to its usefulness in intact nonvital teeth, the walking bleach technique with 10% carbamide peroxide is a safe and effective treatment modality for teeth with denuded enamel. Treatment to achieve the desired final shade may be completed within a single in-office application; however, the decision to discontinue internal bleaching will largely depend on the ceramist's abilities and knowledge of the materials being applied to mask the final stumpf shade of the tooth preparation (Figure 13 and Figure 14). Residual oxygen from the decomposition of 10% carbamide peroxide may remain within the dental tissues for 7 to 15 days after internal bleaching.39,40 This excess oxygen has the potential to negatively impact the bond strength of the adhesive components during the cementation of the final crowns, and it is therefore recommended that at least 2 weeks elapse before final delivery of the definitive restorations (Figure 15).41
Twenty-five-year follow-up studies for patients undergoing internal bleaching have demonstrated long-term predictable color stability, with success rates of 85%.42 Failure is ultimately defined as an observable mismatch of the adjacent dentition by two or more shades,43 and while the precise mechanism for color relapse is not clearly understood, the possibility of future discoloration of the substrate and restoration must be carefully considered and discussed with the patient prior to initiating treatment.
PERIODONTICS
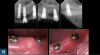
Early intervention in the management of oral biofilms is critical to avoid the breakdown of the surrounding hard and soft tissue in patients with dental implants. It is not uncommon for patients to present to the clinic with implant-supported prosthetics that are in the advanced stages of failure (Figure 16). Often these individuals experience no discomfort or functional issues, and they are not ready to have their implants removed. For the edentulous patient in this situation, the overdenture may serve as a convenient vehicle to deliver an application of 10% carbamide peroxide to the implant threads (Figure 17). Carbamide peroxide in a concentration of 10% possesses a bacterial inhibitory effect on both Streptococcus mutans and Lactobacilli when applied for 2 hours or more,44and the hydrogen that is released has been further shown to efficiently suppress the growth of Actinomyces actinomycetemcomitans.45 Although not clinically ideal, leveraging the antibacterial effects of 10% carbamide peroxide to aid in the reduction of bioburden and oral pathology around failing implants (Figure 18) may serve to provide the patient with the protracted time necessary to prepare mentally and financially for the transition towards a new prosthesis and oral situation.
ORAL SURGERY
When a patient undergoes a full-arch/full-mouth tooth extraction, significant changes in the oral microflora occur, including the reduction of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, and other putative periodontal pathogens below detectable threshold levels. In a large proportion of these patients, particularly those patients with a history of periodontitis,46 many bacterial species remain in the oral cavity for up to 3 months or more.47 Because of the increased risk for infection and discomfort at this postoperative stage, reduction of these pathogens becomes a priority for these patients.
Following the extraction of the terminal dentition in one or both arches, the patient will usually be given an immediate denture to wear as means of providing esthetics and function to the edentulous ridge(s). Immediate dentures also serve to maintain the position of the blood clot, control bleeding, reduce swelling, and act as a protective splint for the surgical sites from food debris and oral fluids. Common protocols often involve instructing the patient not to remove the immediate prosthesis for the initial 48 to 72 hours after surgery to control edema and then to return to the dental clinic to remove the prosthesis and to relieve any occlusal discrepancies or areas of soft tissue impingement. At this time, the patient may be given 10% carbamide peroxide to place on the ridge of the intaglio of the immediate denture for the next 3 to 4 days (for 2 to 8 hours per day) before the 1 week follow-up visit (Figure 19). Compared with other antimicrobial agents, the hydrogen peroxide produced from the slow decomposition of 10% carbamide peroxide possesses numerous advantages, including its natural occurrence in host tissue and effervescence, which can aid in mechanical wound debridement and tissue healing.48Concerns over the use of higher hydrogen peroxide concentrations (>35%) have been reported in the medical literature, noting that the ingestion of large quantities of hydrogen peroxide solution may potentially lead to the catabolism of oxygen and the formation of a gas embolism49; however, hydrogen peroxide in concentrations up to 3% and carbamide peroxide in concentrations up to 15% have been accepted by the US Food and Drug Administration as safe antiseptics for intraoral use.50Furthermore, because the daily production of hydrogen peroxide in the human liver, brain, and eyes is approximately 6.48 g in a period of 24 hours,51 whereas the amount of peroxide placed into the denture base is about 3.5 mg, the body is equipped to effectively tolerate these low doses of peroxide.52
PROSTHODONTICS
Patients often seek replacement of their existing anterior restorations for cosmetic reasons (Figure 20), and they may not always be aware of the impact that whitening their natural teeth can have on the overall esthetics of their new smile. These situations represent an excellent opportunity for the clinical team to inform their patients about the use of custom-fit trays for at-home teeth bleaching. Prior to the restorative treatment, it is important to ensure that the patient understands that the shade of their new ceramic crowns or veneers will not lighten in color if teeth-bleaching products are used after the definitive restorations have been placed. It is equally important for patients to understand that ceramic will not be affected by extrinsic stains and aging in the same way as the adjacent dentition,53 and each restoration will serve as the benchmark shade value that will alert them that their natural teeth have discolored. Consequently, some maintenance will be required in the form of periodic or ongoing teeth-bleaching treatment to maintain the uniformity of tooth shade.
In keeping with the obligation to educate patients, it is prudent that clinicians not only strive to inform patients of all their treatment options but also provide research-based responses to the most frequently asked questions regarding vital teeth bleaching. A nearly universal question among patients who decide to use teeth-whitening treatments relates to what the most effective protocols are for pain management. The discomfort that may arise during the course of treatment is the most frequently cited reason for noncompliance and discontinuation of teeth-bleaching procedures.54 Common methods used to minimize patient discomfort are the use of topical desensitizing agents applied to custom-fit trays during or after treatment. Manufacturers have added combinations of various compounds including potassium nitrate, potassium oxalate, and sodium fluoride to the composition of their bleaching gels to aid in the prevention and reduction of sensitivity during at-home teeth-bleaching.55-57 The use of these topical desensitizing agents is highly effective in mitigating sensitivity caused by exposure to bleaching agents without compromising the efficacy of the treatment and is well documented in the literature.58-60
Another question that patients often ask is, "How white should my teeth be before I stop bleaching?" Throughout the course of treatment, periodic assessment of the tooth shade should be documented as a way to objectively monitor the progress of the teeth-bleaching treatment over time (Figure 21). It has been suggested in the literature, as well as noted in the authors' own experience, that the teeth should ideally match the sclera of the eye for the most impactful results (Figure 22).61 Another common question patients have is, "Do I need to avoid colorful food and drink and/or stay on a ‘white diet' while I am bleaching my teeth?" Multiple studies suggest that coffee, red wine,62 dark fruit,63and smoking64 do not have a significant impact on the overall whitening outcome during treatment.
A final question that is ubiquitous among patients is, "How long will my tooth bleaching results last?" Studies have shown that the minimal color stability of bleached teeth can range from 1 to 3 years, and in some cases tooth shade can remain stable for 10 years or more.65 The importance of periodic maintenance needs to be encouraged, and offering complimentary bleaching gel for custom-fit trays at the 6 month to 1 year hygiene re-care appointments is an excellent motivator to have the patient return to the office.66
CONCLUSION
With the constant bombardment of advertisements, the influence of social media, and the widespread availability of non-peer-reviewed patient resource materials, many of today's dental patients have become overly aware of their dental esthetics, particularly with regard to a perceived ideal of whiter and straighter teeth. Currently the most popular cosmetic dental procedure, vital tooth bleaching has been highly accessible to patients because of its non- invasive nature and relatively low cost. However, dental bleaching agents have much wider applications, which extend beyond mere cosmetic dental enhancement. Continuous use of 10% carbamide peroxide is not only effective for teeth bleaching, but has also proved to be advantageous for oral health maintenance through its additional beneficial cariostatic and antibacterial effects. Thus, practitioners in orthodontics, endodontics, periodontics, and oral surgery can take advantage of these benefits by incorporating the use of 10% carbamide peroxide into many of their commonly utilized treatment modalities. The use of this formulation aids in the oral hygiene of patients receiving orthodontic treatment, and it is useful in the crucial early management of oral biofilms and the prevention of hard and soft tissue breakdown in patients with dental implants. The anti- bacterial effects of 10% carbamide peroxide aid in wound debridement and tissue healing in oral surgery patients. The bleaching benefits of this formulation can also be extended to endodontic patients who request the lightening of single dark nonvital tooth, through the use of internal bleaching. Finally, practitioners in these dental specialties can incorporate carbamide peroxide into their treatment plans without significant impact on the dental treatment trajectory or significant additional cost to their patients, and can indeed enhance patients' treatment outcomes overall.
About the Author
Miles R. Cone, DMD, CDT, FACP
Nuance Dental Specialists
Portland, Maine
Cornelia Cone, MA
Nuance Dental Specialists
Portland, Maine
Polly Wedge, BS
Nuance Dental Specialists
Portland, Maine
References
1. American Academy of Cosmetic Dentistry. Whitening Survey, Summer 2012. https://aacd.com/proxy/files/Publications%20and%20Resources/Whitening%20Survey_Aug12(1).pdf
2. Symmers W St.C, Kirk TS. Urea as a bactericide, and its applications in the treatment of wounds. The Lancet. 1915;186(4814):1237-1239.
3. Shipman B, Cohen E, Kaslick RS. The effect of a urea peroxide gel on plaque deposits and gingival status. J Periodontol. 1971;42(5):283-285.
4. Lazarchik DA, Haywood VB. Use of tray-applied 10 percent carbamide peroxide gels for improving oral health in patients with special needs. J Am Dent Assoc. 2010;141(6): 639-646.
5. Fogel MS, Magill JM. Use of an antiseptic agent in orthodontic hygiene. Dent Surv. 1971; 47(10):52.
6. Haywood VB. Overview and status of mouthguard bleaching. J Esthet Dent. 1991;3(5):157-161.
7. Haywood VB. History, safety and effectiveness of current bleaching techniques: applications of the nightguard vital bleaching technique. Quintessence Int. 1992;23(7):471-488.
8. Haywood VB, Heymann HO. Nightguard vital bleaching. Quintessence Int. 1989; 20(3):173-176.
9. Marshman Z, Gibson B, Robinson PG. The impact of developmental defects of enamel on young people in the UK. Community Dent Oral Epidemiol. 2009;37(1):45-57.
10. Rodd HD, Marshman Z, Porritt J, Bradbury J, Baker SR. Oral health-related quality of life of children in relation to dental appearance and educational transition. Br Dent J. 2011;211(2):E4.
11. Lundgren PG, Wickström A, Hasselblad T, Dahllöf G. Amelogenesis imperfecta and early restorative crown therapy: an interview study with adolescents and young adults on their experiences. PLoS One. 2016;11(6): e0156879.
12. Donly KJ. The adolescent patient: special whitening challenges. Compend Contin Educ Dent. 2003;24(4A): 390-396.
13. Marty M. Time loss. JDR Clin Trans Res.2016;1(2): 108-109.
14. Arseneault L, Bowes L, Shakaar S. Bullying victimization in youths and mental health problems: ‘much ado about nothing'? Psychol Med. 2010;40(5):717-729.
15. Haywood VB, Sword RJ. Tooth bleaching questions answered. Br Dent J. 2017;223(5):369-380.
16. de Almeida LC, Costa CAS, Riehl H, dos Santos PH, Sundfeld RH, Briso ALF. Occurrence of sensitivity during at-home and in-office tooth bleaching therapies with or without use of light sources. Acta Odontol Latinoam. 2012;25(1):3-8.
17. Donly KJ, Donly AS, Baharloo L, et al. Tooth whitening in children. Compend Contin Educ Dent. 2002;23(1A): 22-28.
18. Matis BA, Gaiao U, Blackman D, Schultz FA, Eckert GJ. In vivo degradation of bleaching gel used in whitening teeth. J Am Dent Assoc. 1999;130(2):227-235.
19. Curtis JW, Dickenson GL, Downey MC, et al. Assessing the effects of 10 percent carbamide peroxide on oral soft tissues. J Am Dent Assoc.1996;127(8):1218-1223.
20. Greenwall-Cohen J, Greenwall L. Carbamide peroxide and its use in oral hygiene and health. Dent Update. 2017;44(9):863-869.
21. Greenwall-Cohen J, Greenwall L, Haywood V, Harley K. Tooth whitening for the under-18-year-old patient. Br Dent J. 2018;225(1):19-26.
22. Martini EC, Favoreto MW, Coppla FM, Loguercio AD, Reis A. Evaluation of reservoirs in bleaching trays for at-home bleaching: a split-mouth single-blind randomized controlled equivalence trial. J Appl Oral Sci. 2020;28:e20200332.
23. Kirsten GA, Freire A, de Lima AAS, Ignácio SA, Souza EM. Effect of reservoirs on gingival inflammation after home dental bleaching. Quintessence Int. 2009;40(3):195-202.
24.Lazarchik DA, Haywood VB. Use of tray-applied 10 percent carbamide peroxide gels for improving oral health in patients with special-care needs. J Am Dent Assoc. 2010;141(6):639-646.
25. Sword RJ, Haywood VB. Teeth bleaching efficacy during clear aligner orthodontic treatment. Compend Contin Educ Dent. 2020;41(5):e11-e16.
26. Bowles WH, Ugwuneri Z. Pulp chamber penetration by hydrogen peroxide following vital bleaching procedures. J Endod. 1987;13(8):375-377.
27. Cooper JS, Bokmeyer TJ, Bowles WH. Penetration of the pulp chamber to carbamide peroxide bleaching agents. J Endod. 1992;18(7):315-317.
28. Bakland L, Andreasen J. Dental traumatology: essential diagnosis and treatment planning. Endodontic Topics. 2004;7(1):14-34.
29. Ranka M, Dhaliwal H, Albadri S, Brown C. Trauma to the primary dentition and its sequelae. Dent Update. 2013;40(7):534-542.
30. Hattab F, Qudeimat M, Al-Rimawi HS. Dental discoloration: an overview. J Esthet Dent. 1999;11(6):291-310.
31. Krastl G, Allgayer N, Lenherr P, Filippi A, Taneja P, Weiger R. Tooth discoloration induced by endodontic materials: a literature review. Dent Traumatol. 2013;29(1): 2-7.
32. Mohebbi P, Tour Savadkouhi S. Tooth discoloration induced by calcium-silicate based materials: a literature review. Minerva Stomatol. 2016;65(6):378-384.
33. Attin T, Paqué F, Ajam F, Lennon ÁM. Review of the current status of tooth whitening with the walking bleach technique. Int Endod J. 2003;36(5):313-329.
34. Camps J, de Franceschi H, Idir F, Roland C, About I. Time-course diffusion of hydrogen peroxide through human dentin: clinical significance for young tooth internal bleaching. J Endod. 2007;33(4):455-459.
35. Rotstein I, Zalkind M, Mor C, Tarabeah A, Friedman S. In vitro efficacy of sodium perborate preparations used for intracoronal bleaching of discolored non-vital teeth. Endod Dent Traumatol. 1991;7(4):177-180.
36. Vachon C, Vanek P, Friedman S. Internal bleaching with 10% carbamide peroxide in vitro. Pract Periodontics Aesthet Dent. 1998;10(9):1145-1148.
37. Leonard RH, Sharma A, Haywood VB. Use of different concentrations of carbamide peroxide for bleaching teeth: an in vitro study. Quintessence Int. 1998;29(8):503-507.
38. Perrine GA, Reichl RB, Baisden MK, Hondrum SO. Comparison of 10% carbamide peroxide and sodium perborate for intracoronal bleaching. Gen Dent. 2000;48(3):264-270.
39. Briso AL, Rahal V, Sundfeld RH, dos Santos PH, Alexandre RS. Effect of sodium ascorbate on dentin bonding after two bleaching techniques. Oper Dent. 2014;39(2):195-203.
40. Cavalli V, de Carvalho RM, Giannini M. Influence of carbamide peroxide-based bleaching agents on the bond strength of resin-enamel/dentin interfaces. Braz Oral Res. 2005;19(1):23-29.
41. Shinohara MS, Peris AR, Pimenta LAF, Ambrosano GMB. Shear bond strength evaluation of composite resin on enamel and dentin after nonvital bleaching. J Esthet Restor Dent. 2005;17(1):22-29.
42. Amato A, Caggiano M, Pantaleo G, Amato M. In- office and walking bleach dental treatments on endodontically-treated teeth: 25 years follow-up. Minerva Stomatol. 2018;67(6):225-230.
43. Amato M, Carratù P, Spagnuolo G, Borelli B, Sorrentino R. In-office walking bleach treatment of non-vital teeth with 10% carbamide peroxide: a 21-year retrospective evaluation. International Dentistry - African Edition. 2012;2(6):32-38.
44. Bentley CD, Leonard RH, Crawford JJ. Effect of whitening agents containing carbamide peroxide on carcinogenic bacteria. J Esthet Dent. 2000;12(1):33-37.
45. Quirynen M, Teughels W, De Soete M, van Steenberghe D. Topical antiseptics and antibiotics in the initial therapy of chronic adult periodontitis: microbiological aspects. Periodontol 2000. 2002;28:72-90.
46. Quirynen M, Van Assche N. Microbial changes after full-mouth tooth extraction, followed by 2-stage implant placement. J Clin Periodontol. 2011;38(6):581-589.
47. de Waal YCM, Winkel EG, Raangs GC, van der Vusse ML, Rossen JWA, van Winkelhoff AJ. Changes in oral microflora after full-mouth tooth extraction: a prospective cohort study. J Clin Periodontol. 2014;41(10):981-989.
48. Lu M, Hansen EN. Hydrogen peroxide wound irrigation in orthopaedic surgery. J Bone Jt Infect. 2017;2(1): 3-9.
49. Sung J, Cossarini F, Palaiodimos L, Benson B, Meholli M. Extra oxygen leads to bubble trouble: portal vein gas embolism from 3% hydrogen peroxide ingestion. Cureus. 2018;10(2):e2136.
50. FDA Department of Health and Human Services. Oral health care drug products for over-the counter human use; antigingivitis/antiplaque drug products; establishment of a monograph. Fed Regist. 2003;68(103):32231-32287.
51. FDA (Food and Drug Administration). Hydrogen peroxide: proposed affirmation of GRAS status as a direct human food ingredient with specific limitations. Fed Regist. 1983;(48):52323-53333.
52. Li Y. The safety of peroxide-containing at-home tooth whiteners. Compend Contin Educ Dent. 2003;24(4A):384-389.
53.Haywood VB, Goldstein RE. Stains and discolorations. In: Goldstein RE, ed. Esthetics in Dentistry. 2nd ed. BC Decker; 2002:38.
54. Rahal V, Azevedo FA, De Oliveira Gallinari M, et al. Avaliação sensorial quantitativa da sensibilidade dentária com o uso de um dessensibilizante. Dental Press. 2014; 11(2):108-117.
55. Haywood VB, Caughman WF, Frazier KB, Myers ML. Tray delivery of potassium nitrate fluoride to reduce bleaching sensitivity. Quintessence Int. 2001; 32(2):105-109.
56. Jorgensen MG, Carroll WB. Incidence of tooth sensitivity after home whitening treatment. J Am Dent Assoc. 2002;133(8):1076-1082.
57. Chen H-P, Chang C-H, Liu J-K, Chuang S-F, Yang J-Y. Effect of fluoride containing bleaching agents on enamel surface properties. J Dent. 2008;36(9):718-725.
58. Armênio RV, Fitarelli F, Armênio MF, Demarco FF, Reis A, Loguercio AD. The effect of fluoride gel use on bleaching sensitivity: a double-blind randomized controlled clinical trial. J Am Dent Assoc. 2008;139(5):592-597.
59. Bernardon JK, Martins MV, Rauber GB, Junior SM, Baratieri LN. Clinical evaluation of different desensitizing agents in home-bleaching gels. J Prosthet Dent. 2016;115(6):692-696.
60.Godoy CE, Consani S, Guimarães AT, Laurindo BM, Mendonça MJ, Camilotti V. Effect of two desensitizing agents applied previous to in-office bleaching on the degree of whitening and dentin sensitivity: a randomized, controlled, double-blind clinical trial. Am J Dent. 2021;34(2):70-74.
61. Mrazek B. "Don't bleach until you see the white of their eyes". Compend Contin Educ Dent. 2004;25(6): 472, 474, discussion 476.
62. Côrtes G, Pini NP, Lima DANL, et al. Influence of coffee and red wine on tooth color during and after bleaching. Acta Odontol Scand. 2013;71(6):1475-1480.
63. Matis BA, Wang G, Matis JI, Cook NB, Eckert GJ. White diet: is it necessary during tooth whitening? Oper Dent. 2015;40(3):235-240.
64. de Gues JL, Bersezio C, Urrutia J, et al. Effectiveness of and tooth sensitivity with at-home bleaching in smokers. J Am Dent Assoc. 2015;146(4):233-240.
65. Haywood VB, Leonard RH, Nelson CF, Brunson WD. Effectiveness, side effects and long-term status of nightguard vital bleaching. J Am Dent Assoc.1994; 125(9):1219-1226.
66. Strassler HE. Vital tooth bleaching: An update. Mdental Continuing Education Course. The Baltimore College of Dental Surgery, University of Maryland Dental School. Fall 2006;1-12. Available at: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.520.7025&rep=rep1&type=pdf