You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
INTRODUCTION
Orthodontics is the specialty of dentistry focused on the diagnosis and treatment of dental and associated facial anomalies. The results of orthodontic treatment can be dramatic, with gorgeous smiles, improved dental health, and an enhanced quality of life for many people of all ages. Orthodontic problems, which can result from genetic and environmental factors, must be diagnosed before treatment begins. Proper diagnosis involves taking photographs, x-rays, and dental impressions, which enable the dental team to make informative decisions about the form of treatment necessary. Treatment typically lasts from 6 to 30 months, depending on age, and the severity of the orthodontic problem. This course will cover the fundamental basics of orthodontics.
ORTHODONTICS SPECIALTY
Orthodontics is the dental specialty that deals with the diagnosis, prevention, and treatment of malocclusion and other irregularities of the teeth, jaws, and face. While many people consider orthodontic abnormalities as strictly esthetic issues, the fact remains that most malocclusions and other irregularities pose a serious health threat to the patient. Uncorrected malocclusions can lead to future problems such as tooth decay, periodontal disease, temporomandibular joint disorders, and degeneration of the TMJ. Other emotional problems may occur in the individual with severe orthodontic malocclusions when social interactions are compromised due to the abnormality. Malocclusion and dentofacial deformities result due to disturbances in normal development. Factors that may influence such deformities or malocclusions include those that are developmental, genetic, environmental, or functional in nature. In most individuals, it is a combination of two or more of these factors that lead to their orthodontic irregularities.
Causative Factors
Developmental Factors
These are disturbances that occur to the dentition as teeth are being formed. Some of the most common developmental disturbances influencing malocclusion are: congenitally missing teeth, malformed teeth, supernumerary teeth, impaction, and ectopic eruption (the tooth erupts away from normal position.)
Genetic Factors
These are inherited traits that influence the development of teeth and jaws. It is likely that issues of congenitally missing teeth, abnormally small jaws, abnormally large teeth, and other such abnormalities are hereditary and these traits can be found in other family members of the individual.
Environmental Factors
These are injuries or traumatic disturbances that lead to the development of malocclusions. Prenatally, fetal molding may influence the irregular development of the jaws when an arm or leg of the fetus is pressed against the mandible. Trauma during birth may also injure the jaws to the extent of permanently affecting their growth and development. Other traumas affecting orthodontic development can occur to teeth throughout life: the permanent tooth buds can become damaged when an injury occurs to the primary teeth; teeth may shift from their normal position as a result of premature loss of primary teeth; rampant caries; or direct injury to the permanent tooth may cause shifting of the adjacent dentition.
Functional Factors
These factors affecting tooth position and occlusion are the result of habits attained by the individual. Sucking habits that involve the thumb, fingers, lip or tongue may influence development of the jaws and dentition if the habit extends into the period of mixed dentition. Tongue thrusting during swallowing is another functional habit that is usually learned as an infant as the baby begins to nurse. This habit will remain with the individual indefinitely unless functional intervention occurs. The tongue is a powerful muscle that can mold the shape of the jaws and influence the positions of the teeth. Bruxism and mouth breathing are other habits that can affect the positions of the teeth and dentofacial structures.
Malaligned Teeth
Malocclusion, as discussed earlier in this text, is a primary factor in diagnosing orthodontic conditions. In addition to evaluating occlusion, specific alignment of the teeth and arches must be considered. Some of the more common malalignment problems include crowding, overjet, overbite, open bite, and crossbite.
Crowding - tooth mass discrepancies or unusually small arches may lead to the malalignment of teeth due to the lack of adequate arch space. One or more teeth may be involved when a crowning situation occurs.
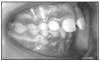
Overjet (Figure 1) -this term is used to refer to the horizontal distance between the facial surfaces of the mandibular incisors to the lingual surfaces of the maxillary incisors. An excessive overjet is commonly referred to as "buck teeth." An excessive overjet would measure 3 mm or more.
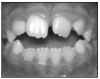
Overbite (Figure 2) - is the vertical overlap of the maxillary incisors as they extend past the incisal edges of the mandibular incisors. A measurement of 2 mm of overbite is desired for normal alignment.
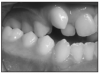
Open bite (Figure 3) - is the lack of vertical overlap of the maxillary incisors with the patient in posterior centric occlusion. The anterior teeth appear open when the patient is biting on their back teeth.
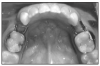
Crossbite (Figure 4) - this occurs when a maxillary tooth (or teeth) occludes lingually or end-to-end with the mandibular teeth as the patient bites in centric occlusion. In normal occlusion, the maxillary teeth will be positioned facially to the mandibular teeth.
TREATMENT OF ORTHODONTIC CONDITIONS
Orthodontics can be performed for both functional and esthetic reasons. Types of orthodontic treatment include preventive or interceptive, and corrective.
Preventive or Interceptive Orthodontics
Preventive or interceptive orthodontic treatments are performed to prevent or eliminate irregularities, or to intercede or correct problems as they develop. Various preventive or interceptive treatments include1:
• restoration of primary teeth in order to prevent premature loss
• placement of a space maintainer (described below) to save space for eruption of a permanent tooth
• correction of oral habits (such as thumb sucking and tongue thrusting) that may cause problems in the oral cavity
• observation of growth patterns and development of teeth and bones
• detection of deviations from the normal that may affect dental development
• extraction of primary teeth to allow space for and proper alignment of the permanent teeth
• extraction of primary or permanent teeth to prevent overcrowding
• correction of a crossbite through the use of a fixed or removable appliance
• correction of a jaw size discrepancy through the use of a fixed or removable appliance
Space maintainers (Figure 5) are placed when a primary tooth is lost prematurely. If a primary tooth is lost prematurely, the adjacent teeth may drift into the edentulous space, possibly preventing or altering the eruption of the permanent tooth. The space maintainer usually consists of a metal band with a wire loop soldered together. The band is cemented to one adjacent tooth and the wire loop fits in the edentulous space, providing a brace between the teeth adjacent to the edentulous space. This prevents the drifting of these teeth into the space, thus saving room for the eruption of the permanent tooth. Space maintainers may also be removable, but these are less common due to the fact that they require a higher level of patient compliance. Usually, an alginate impression is taken and the model is sent to the dental laboratory where the space maintainer is custom fabricated.
Corrective Orthodontics
Corrective orthodontics are performed to reduce or eliminate existing problems. Corrective treatments include:1
• placement of a removable appliance for correction or maintenance of orthodontic treatment
• placement of fixed appliances attached to the teeth
• orthognathic (jaw) surgery for severe cases
The general practitioner may perform limited orthodontic procedures, such as preventive and interceptive treatments, while the orthodontist will perform more complex procedures, such as corrective orthodontic treatment.
Orthodontic Records and Treatment Planning
In order to determine a diagnosis and treatment plan for the orthodontic patient, an appointment is devoted to obtaining comprehensive records. The following components of the orthodontic records are acquired during this appointment:
• complete medical and dental histories are recorded
• physical growth evaluation
• social and behavioral evaluation
• clinical examination to include an evaluation of facial esthetics; evaluation of oral health; and evaluation of jaw and occlusal function
• diagnostic records to include intraoral and extraoral photographs; radiographs and cephalometric analysis; and diagnostic models
During a subsequent appointment, the diagnosis and treatment plan will be presented, consent forms will be signed, and financial arrangements will be made. Patients will be made aware of their obligations to the treatment including cooperation in wearing prescribed appliances, keeping scheduled monthly appointments for adjustments, and maintaining acceptable oral hygiene.
ORTHODONTIC APPLIANCES
In order to treat the patient's orthodontic condition, the orthodontist will use fixed or removable appliances or a combination of both to achieve the desired results. Fixed appliances are usually referred to as braces. Other forms of fixed appliances include palatal expanders, Herbst appliances, habit control devices, and bonded lingual retainers. Removable appliances may include functional appliances which help position the jaws in the correct alignment, or retainers that stabilize the teeth after they have reached their desired positions.
Fixed Appliances
Fixed appliances, or braces, consist of a combination of bands, brackets, archwires, and auxiliaries (such as tubes or hooks) (Figure 6). These appliances are capable of moving a tooth in any of the six directions: mesially, distally, facially, lingually, apically, or occlusally.
Bands are metal components that extend the entire circumference of a tooth and are cemented usually by means of glass ionomer or zinc phosphate cement. Prior to the placement of a band, the patient generally must wear a "separator" for several days in the mesial and distal contact of the tooth receiving the band. The separator will slightly push the teeth apart so the band may be fitted around the desired tooth and slide down through the contacts. Separators selected for use may be of one of the following three types: elastomeric rings, brass wires, or stainless-steel springs.
Brackets are bonded to the facials of the teeth using resin-bonded cements. The bracket is generally bonded to anterior teeth and premolars. The bracket is welded to a bonding pad which is the means by which it is bonded to the tooth. Most brackets are constructed with four "tie wings" so that the archwire will lie horizontally through the wings.
Archwires are attached to the brackets and bands and act as guides for the dental arches. There are many types of different archwires that elicit movement of teeth in various ways. Archwires may be round, square, or rectangular and come in various metals such as stainless steel, beta titanium, or nickel titanium. The orthodontist may place additional bends or loops in the archwire in order to elicit tooth movement in a desired direction.
Ligatures tie the archwire to the bracket so that the wire can gently pull against the teeth. Generally, there are two types of ligatures: elastomeric or stainless steel. Elastomeric ligatures may consist of individual o-shaped modules (alastics) or power chains. The power chains are continuous alastics that put additional forces on teeth, pulling them together to close spaces.
Elastics are also known as "rubber bands." They are placed by the patient from one tooth to another as prescribed by the orthodontist. The purposes of elastics are to help close spaces or correct occlusal relationships.
Removable Appliances
Orthodontists use a variety of removable appliances to elicit tooth movement, correct jaw discrepancies by controlling growth, and stabilizing teeth. Patients may be prescribed certain removable appliances in conjunction with wearing fixed appliances.
Headgear is an orthopedic device used to control growth and tooth movement (Figure 7). Its components include a facebow and a traction device. The facebow contain an intraoral and extraoral component. The intraoral part of the bow fits on buccal tubes welded to the maxillary first molar bands. The extraoral part of the facebow attaches to the traction device. The traction device applies the force that guides the teeth and jaws to the desired relationship.
Functional appliances may be prescribed for young, growing patients to help correct habits while helping guide the teeth and jaws into their proper relationships. Examples of functional appliances include the Bionators and the Frankel appliances.
Retainers are appliances that are fabricated for the patient to hold the teeth in position after the fixed appliances have been removed. It is important to retain teeth in a stable position for a period of time in order to allow gingival and periodontal tissues the time to reorganize and support the new positions of the teeth. Some common types of removable retainers are the Hawley retainer (Figure 8) and the positioner.
Clear Aligners: A recently accepted concept in orthodontic treatment is the use of esthetic, removable orthodontic appliances called "aligners" (Figure 9). In conjunction with the orthodontist's diagnosis and treatment plan, 3-D computer technology is used to design and fabricate a series of custom aligners for the select orthodontic patient.
The aligner is worn by the patient for at least 22 hours per day and only removed for eating and cleaning the teeth. Teeth are moved gradually by the aligner and as the aligner becomes passive, it is replaced with the next aligner. Each subsequent aligner is designed to move teeth in a manner a little different from the previous aligner. The aligners resemble a whitening or fluoride tray but are thinner, more precise, and fabricated from a more rigid, exclusive material. The number of aligners and length of treatment vary based upon the complexity of the case.
Orthodontic Instruments
The orthodontic specialty utilizes a variety of specialized instruments to facilitate the treatment of the patient and to adjust the appliances:
Orthodontic scaler: aids in removal of excess cement or bonding material and removal of elastomeric rings.
Ligature director: guides the elastic or wire ligature around the bracket.
Band plugger: has a round serrated end to help seat a molar band.
Band seater (or bite stick): consists of a molded plastic handle with a triangular stainless-steel serrated working area (Figure 10). This is used to aid in seating a molar mand.
Bracket placement tweezers: long-tipped reverse action tweezers with fine serrated beaks. They are used to carry and place the bonded bracket to the tooth.
Bird-beak pliers: are useful in forming and bending wires for either fixed or removable appliances (Figure 11).
Contouring pliers: aid in fitting bands for fixed or removable appliances.
Weingart utility pliers: have finely serrated narrow beaks, allowing accessibility to all areas. They are used for placing archwires (Figure 12).
Three-prong pliers: are used primarily in closing and adjusting of clasps (Figure 13).
Posterior band removing pliers: remove bands without placing stress on the tooth or providing discomfort to the patient (Figure 14).
Pin-and-ligature cutter: cuts the ligature wire once it has to be ligated around the bracket (Figure 15).
Howe (110) pliers: have a flat, rounded, serrated tip that allows placement and removal or creation of adjustment bends in the archwire (Figure 16).
Wire bending pliers: are used for holding and bending and adjusting arch wires to create movement.
Ligature tying pliers: have finely serrated narrow beaks to allow ease in ligature tying.
Distal-end cutting plier: cuts and holds the distal end of the archwire intraorally so as not to drop a small piece of wire into the oral cavity (Figure 17).
Mosquito hemostat: used to hold elastic ligature modules as they are being tied to the wings of the bonded bracket (Figure 18).
Oral Hygiene for the Orthodontic Patient
Immaculate oral hygiene is necessary for the orthodontic patient in fixed appliances. Food and debris will have many places to attach and hide, making the patient more susceptible to caries and periodontal disease. The patient will be given a special orthodontic toothbrush and be shown how to brush around the appliances to remove plaque and food debris. The tooth is contoured to fit around the appliances with extra-long bristle along the outside rows of the brush. The patient should be shown how to utilize the floss threader and emphasis should be given to daily flossing as well as brushing. During orthodontic treatment, the interproximal areas will be more susceptible to plaque buildup and the interdental papillae will be prone to inflammation.
The patient should be advised to alter their diet by avoiding foods that would stick to the appliances or be so hard as to damage them. Foods normally eaten by biting into them, such as apples, corn, ribs, and sandwiches, should be cut and small bites should be placed in the back of the mouth for chewing.
Fluoride rinses are an important part of the home care during orthodontic treatment. Fluoride helps promote the remineralization of damaged enamel incurred due to exposure to excessive acid from plaque hiding in the appliances.
Updated Technology
The orthodontic specialty has embraced modern day dental technology and many now incorporate imaging systems and 3D printing into their daily workflow. Although many offices still use alginate for diagnostic study models of their patient's teeth, many have incorporated digital technology into the initial data gathering with intraoral photography, digital scanning in lieu of messy alginate impressions and the use of 3D printing for the fabrication of appliances in house.
With digital impressioning, patients have a more comfortable, quicker, and more impressive appointment experience. Scanned images can be seen almost immediately on the computer screen. 3D printing is used in the fabrication of clear patient aligners, bite splints as well as retainers for patient use.
REFERENCES
1. Bird, Doni, and Robinson, Debbie. Torres and Ehrlich Modern Dental Assisting. 8th ed., St. Louis: Elsevier Saunders 2005.
2. Finkbeiner, Betty Ladley, and Johnson, Claudia Sullens. Mosby's Comprehensive Dental Assisting: A Clinical Approach. St. Louis: Mosby, 1995.
3. Phinney, Donna J., and Haldstead, Judy H. Delmar's Dental Assisting: A Comprehensive Approach. 2nd ed.; Clifton Park, New York. Delmar 2004.
4. Phinney, Donna J. Dental Assisting: A Comprehensive Approach. 5th ed., Boston, Massachusetts. Cengage Learning 2017.
ABOUT THE AUTHORS
The original author of #613 General Chairside Assisting: A Review for a National General Chairside Examwas:
Antoinette P. Metivier, BS, was an assistant professor in the Dental Assisting Department at the New Hampshire Institute in Concord, NH where she taught dental radiology. She attended the North Carolina's Dental Radiology Institute for Dental Educators and developed and presented radiology review courses for the New Hampshire Dental Assistants Association.
The course was later completely revised by:
Kimberly Bland, CDA, EDDA, MS, has served as ADAA's Fifth District Trustee, national Secretary, national Vice President, national President Elect and twice as ADAA President (2007-2008; 2014-2016). She has held several offices in both the local and state ADAA organizations, having been President of the Florida Dental Assistants Association for three terms and is past president of the Sara-Mana Dental Assistants Society of Florida. She was a founding member of the Professional Dental Assistants Educational Foundation (PDAEF) and continues to remain active with national activities.
Ms. Bland is a member of the Florida Board of Dentistry Dental Assisting Council and has held offices in the Florida Allied Dental Educators Association and as Florida Region V Post-Secondary Advisor of the Florida Health Occupation Students of America (HOSA). Kimberly is a graduate of the University of South Florida, where she majored in Industrial Technical Education. Earlier, she earned her Dental Assisting Certificate at Manatee Technical Institute where she is now the dental assisting program director.
The dental specialties section was removed from the original #613 General Chairside Assisting: A Review for a National General Chairside Examas a standalone course and was reviewed and developed by:
Natalie Kaweckyj, LDA, RF, CDA, CDPMA, COA, COMSA, CPFDA, CRFDA, MADAA, BA -_began her dental assisting career over 28 years ago after graduating from the CODA accredited program ConCorde Career Institute. She spent twelve years working in a private practice where she worked clinically nine years and administratively the remaining three. She then moved onto teaching dental assisting and eventually became director of that program. Overlapping with teaching, Natalie began her tenure with Children's Dental Services in 2007 in management and currently serves as clinical coordinator responsible for the day to day operations at over 600 locations where services are provided throughout Minnesota. Natalie enjoys the challenges of the public health sector and is gratified in serving those that are underserved, especially in a hospital setting under general anesthesia. With over a decade of restorative functions experience under her belt, she enjoys working with professionals new to dentistry as her love for teaching comes into play with the utilization of clinicians to the full scope of their licenses. The clinic keeps Natalie busy with billing management when not at the hospital. Natalie also graduated with a BA in Biology and Psychology from Metropolitan State University in 2005.
Ms. Kaweckyj served two terms as ADAA President (2017-2018; 2010-2011). She remains active on several councils, and served as a President of the Professional Dental Assistants Educational Foundation (PDAEF). She served as a three-term president for MnDAA and remains as the state business secretary. Natalie has been recognized with several ADAA awards, was one of the first ADAA Fellows in 1999 and became the first ADAA Master in 2004. She has published numerous continuing education courses, over 250 articles and lectures on a variety of dental subjects locally, nationally and internationally. Organized dentistry gave Natalie the insight that you can make a difference as a dental professional, and she was instrumental in seeing licensure for dental assistants come to fruition in MN in 2009 as well as several expanded functions. Her dream would be to see mandatory credentialing become a reality in all states for protection of the public and maintaining integrity of the dental assisting profession.