You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Compassion is central to patient care and is considered to be an essential component of the role of a healthcare professional.1 Compassion requires the provider to be intentional about getting to know a patient and their needs in order to take action to minimize pain and discomfort.2 Compassion satisfaction (CS) is defined as pleasure derived from being able to do one's job well. Doing one's job well can contribute to a healthcare professionals' positive feelings towards one's job allowing for compassion competence.1Compassion competence is the ability to understand, identify, and limit patients' difficulties that can also contribute to the emotions of a health care professional.3,4
Studies have shown that over time compassion can diminish, allowing for an increase in compassion fatigue and burnout in health care professionals, including physicians, nurses, and midwives, just to name a few.5-7 Negative emotions like cumulative work-related stress, depression, anxiety, and anger can play a critical role in compassion competence and can greatly affect the healthcare provider, leading to compassion fatigue.5,6 This type of fatigue occurs in healthcare providers when they are no longer able to feel empathy and meet the emotional burden or needs of their patients.2,8 Compassion fatigue has been referred to as the ‘cost of caring' and occurs when the provider is not able to adequately engage in self-care to refresh or refuel.9 The risk factors for compassion fatigue include anxiety, excessive empathy, fewer years of experience, less education, and job-related factors.5,10
When compassion fatigue is not resolved, it can progress to burnout and impact the ability of the healthcare professional to provide compassionate care to patients.4,8 Compassion fatigue may lead to healthcare professionals leaving their careers early, ahead of retirement, due to burnout.11 To diminish clinical burnout, it is important to understand the factors leading to compassion fatigue and implement prevention and management strategies such as mindfulness.11,12
Most of the research related to the concept of compassion and compassion fatigue is in nursing with very little literature in the dental profession.1,2,5,8,11,13,14 However, one study related to South Korean dental hygienists was conducted using the Professional Quality of Life (ProQoL) instrument. Results from the Han and Kim study showed compassion fatigue had a positive correlation with burnout whereas compassion satisfaction and social support was negatively correlated with burnout.15 The stressors identified by Han and Kim were caused not only by the workplace itself, but also due to the interpersonal relationships in the workplace.15 This included pressure, conflict, and competition between colleagues which lead to conflicts with patients.15 While there could have been misinterpretation of the results due to the translation of the original study, the findings were consistent with the nursing literature.5,8,11,13,14 Bercasio et al. used the Maslach Burnout Inventory to explore burnout in California DHs and found about a third of participants had high levels of emotional exhaustion which is a component of compassion fatigue in the ProQOL framework.5,16,17 Patel et al. used the Oldenburg Burnout Inventory and also found emotional exhaustion was associated with burnout among clinical DHs.18 In addition, Malcolm et al. found emotional demands was a predictor of burnout in clinical DHs.19
Given the centrality of compassion to dental hygiene care and paucity of research to explore compassion satisfaction, compassion fatigue, and burnout in clinical dental hygienists within the United States (US), more research is needed. The purpose of this study was to examine the relationship between compassion satisfaction (CS), compassion fatigue (CF), burnout (BO), demographics and work characteristics, such as thoughts of leaving the dental profession among clinical DHs in the US.
Methods
This study was granted exempt status by the MCPHS University Institutional Review Board (IRB) within accordance of revised Common Rule at 45 CFR 46.104 d (2)(ii) and was assigned protocol number IRB041120B. A cross-sectional survey research design was used with a non-probability sample of DHs. Participants were recruited from dental hygiene social media groups. Dental hygienists providing patient care in the US with a minimum of one year of clinical experience were eligible to participate. Respondents were excluded if they did not hold an active dental hygiene license, were not providing clinical patient care, had less than one year of clinical experience, and/or did not reside in the US.
A power analysis was conducted using G*Power for the most conservative prepared statistical test (one-way ANOVA, two-tailed, four groups) with a medium effect size (f=0.25), α=.05, and 80% power, recommended a minimum sample size of n=180. After adjusting for an expected attrition of 30%, the final recommended sample size was n=257.
Instruments
The survey consisted of two sections: demographics and work characteristics (17 items) and the ProQoL20 (version 5; 30 items) for a total of 47 items. The demographic questions addressed age, gender, ethnicity, education, and geographic location. The work characteristic questions included: type of practice, days/hours worked per week, years of practice, average appointment times, possibility of leaving the field, and one open-ended question about reasons for wanting to leave the profession.
Professional Quality of Life Scale
The ProQoL20 (version 5) is a validated survey used to evaluate professionals in a variety of fields defined as ‘helper' professions about their levels of compassion satisfaction, compassion fatigue, and burnout. The instrument construct validity has been established in over 200 studies.20,21 The ProQol consists of a series of 30 questions with sub-scales that include: compassion satisfaction (α=0.88), compassion fatigue (α=0.81), and burnout (α=0.75). 20,21 Convergent and discriminant validity have also been assessed and interscale correlations are small (2 to 5%), suggesting the sub-scales measure different constructs.20 Test-retest reliability was good with small standard error.20
Each sub-scale contained 10 items scored on a five-point Likert-type scale (1=never, 2=rarely, 3-sometimes, 4=often, and 5=very often) and each sub-scale had a possible 50 points. The compassion satisfaction sub-scale scores were categorized as follows: high >42, moderate 33-41, and low <33 with an average of 37.20 Burnout sub-scale scores were categorized as: high >27, moderate 18-26, and low <18 with an average of 22.20 Compassion fatigue was categorized as: high >17, moderate 8-17, and low <8 with an average score of 13.20
Procedures
The survey was web-based and disseminated through social media groups. The social media group administrators were contacted for permission to post the survey invitation. Seven Facebook groups provided approval to post the survey invitation. Once permission was obtained, the invitation to participate was displayed on social media with the link to the electronic survey (Qualtrics; Provo, UT, USA). The survey link took the participant to the consent to participate page. If individuals did not meet study criteria and did not agree to participate, they were taken to the end of the survey. There were no incentives provided for participation. A reminder to complete the survey was posted weekly on the social media group sites. Once an adequate number of responses was obtained, the survey was closed. The survey was active for three weeks.
Analysis
The data was evaluated to identify any survey with less than 80% complete responses which were then excluded from parts or the entire analysis. Each variable was reviewed for change to report issues of non-normal distributions. Pearson's correlation coefficients were calculated to assess the relationship between continuous demographic variables and each ProQol subscale (compassion satisfaction, burnout, and compassion fatigue). Student's t-tests were calculated to determine if there was a difference in mean ProQol scores between dental hygiene degree type (associate or bachelor's), highest degree outside of dental hygiene (associate or bachelor's), and if a respondent had thought about leaving the field. For participants who had thought about leaving the field, a logistic regression was calculated with each subscale score to predict if the participant had thought about leaving (yes=1, no=0). The alpha level was set at .05 for hypothesis testing and all measures of effect size (i.e. 95% Confidence Interval, Phi Coefficient, R2, Cohen's d) were established and reported.
For the data from the open-ended question, responses were analyzed using a thematic approach to identify the most common words, phrases, or ideas from the data. While analyzing the responses, the data was continuously coded and organized categorically while being repeatedly reviewed. Codes were assigned to themes. Additionally, codes were cross checked by a second investigator to ensure trustworthiness and triangulate data to create a coherent justification for themes. In addition, respondent's words were used to illustrate the dimensions of the themes.
Results
A total of 553 individuals accessed the survey link. Twenty-six participants completed less than 80% of the survey, resulting in a completion rate of 99% (n=527). A national sample of DHs participated with an even distribution across the US, with the exception of a smaller sample from the South. Most participants identified as White (88%, n=424), female (98.9%), had a mean age 44.6 (SD=11.8) of and worked clinically in private practice (89.7%). Approximately 73% (n=347) had an entry-level associate dental hygiene degree. The mean number of hours worked per week was 30.6 (SD=8.4) and the mean days worked per week was 3.8 (SD=1.0). The mean number of years providing clinical patient care was 19.3 (SD=12.8). More than two-thirds of the participants (68.2%, n=324) reported having thought about leaving the dental profession. However, less than one-third (28.8%, n=137) reported it was extremely or very likely they would leave dental hygiene practice within the next five years. Demographic and work characteristics are shown in Table I.
Professional Quality of Life
Nearly half of the participants (42.7%) indicated often or very often for the statement "I feel worn out because of my work as a helper" which is related to burnout, although a majority of participants (91.7%) responded often and very often to the statement "I get satisfaction from being able to help people" (Table II). Other findings noted with the ProQol was that participants stated, "I am happy (75.2%)," "My work makes me feel satisfied (55.7%)," and "I am happy that I chose to do this work (62.9%)," which are all related to compassion satisfaction. Other participants stated that "I feel ‘bogged down' by the system (29%)," "I feel overwhelmed because my case workload seems endless (28.2%)," and "I feel trapped by my job as a worker (11.8%)." The mean levels of compassion satisfaction versus burnout and compassion fatigue were slightly different. The mean compassion satisfaction subscale scores were 39.0 (SD=6.2), while burnout was 22.73 (SD=5.6), and compassion fatigue was 20.68 (SD=5.2). Compassion satisfaction and burnout mean subscales scores were in the moderate range, while compassion fatigue mean scores was in the high range.
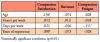
Pearson's correlation coefficients were calculated to assess the relationship between continuous demographic variables and each ProQol subscale (compassion satisfaction, burnout, and compassion fatigue). The correlation matrix for each comparison is shown in Table III. Increases in age (r=0.13) and years of experience (0.10) were positively correlated with compassion satisfaction (p<0.05). The number of days worked per week was negatively correlated with compassion fatigue (r=-0.11) (p<0.05), although these relationships are considered small by conventional analysis.22 All other correlations were non-significant (p>0.05).
Student's t-tests were calculated to determine if there was a difference in mean ProQol scores between dental hygiene degree type (associate or bachelor's), highest degree outside of dental hygiene (associate or bachelor's) and whether a DH had thought about leaving the field. Dental hygienists who have thought about leaving the field (n=324) had a lower compassion satisfaction score (M=37.6, SD=6.1, t=7.8, p<0.001), higher burnout score (M=24.3, SD=5.3, t=-9.9, p<0.001), and higher compassion fatigue (M=21.4, SD=5.2, t=-4.8, p<0.001) as compared to participants (n=151) who had not thought about leaving (M=42.1, SD=5.3; M=19.3, SD=4.6; M=19.0, SD=4.8). All significant p-values remained below 0.001 after assessing the assumption of equal variance using Levene's Test (p>0.05). Analysis showed no difference in mean subscale scores between an entry level associate degree versus a bachelor's degree in dental hygiene or for participants whose highest degree was an associate versus a bachelor's degree (p>0.05).
To determine the influence of each subscale score on leaving the dental hygiene profession, a logistic regression was calculated with each subscale score to predict if a respondent had thought about leaving (yes=1, no=0). The model predicted whether a respondent had thought about leaving the field (χ2(3)=97.2, p<0.001, Nagelkerk R=0.26). After controlling for the influence of burnout and compassion fatigue, compassion satisfaction was a significant predictor of thinking about leaving the profession (W=4.2, p=0.04). The model predicted for each unit increase in the compassion satisfaction score, an individual is 5% (Exp(β)=0.95) less likely to say they have thought about leaving the field. After controlling for compassion satisfaction and compassion fatigue, burnout predicted thinking about leaving the field (W=24.8, p<0.001). A one-unit increase in burnout predicted a 1.2 times increase in the likelihood a respondent had thought about leaving the field. After controlling for compassion satisfaction and burnout, compassion fatigue was not a significant predictor of thinking about leaving the dental hygiene profession (W=0.01, p=0.6).
To assess whether ProQol subscale scores were related to responses to the item regarding the likelihood of leaving the field in the next five years, response options were first recoded from extremely unlikely=1, unlikely=2, somewhat likely=3, likely=4, and extremely likely=5, into a new variable with two categories (1-2=unlikely [n=222]; 3-5=likely [n=253]). Three t-tests were calculated with the groups as dependent variables and each ProQol subscale score as a dependent variable. There was a difference in mean compassion satisfaction scores (t(473)=3.1, p=0.002), burnout (t(473)=-3.5, p<0.001), and compassion fatigue (t(473)=-2.1, p=0.04). The unlikely to leave category had a higher mean compassion satisfaction score (M=39.9, SD=6.0, p=0.002) than the likely to leave (M=38.2, SD=6.2) group. Those in the unlikely group had a lower mean burnout score (M=21.8, SD=5.3, p<0.001) than the likely (M=23.6, SD=5.7) group, and a lower mean compassion fatigue score (M=20.2, SD=5.4, p=0.04) compared to the likely (M=21.3, SD=5.0) group.
A Cohen's d was calculated for each t-test to determine the magnitude of effect. For compassion satisfaction (d=0.3) and burnout (d=0.3) Cohen's d indicated a medium effect size. The difference between likely and unlikely groups resulted in a small effect size (d=0.2).
Themes
A thematic analysis was conducted for responses to the open-ended question "What is your reason for wanting to leave the dental hygiene profession?" Four themes arose from the responses including: 1) stress, 2) physical demands, 3) negative work environment, and 4) production over patient care. Two-thirds (66%, n=349) of the participants responded to the open-ended question.
Theme 1: Stress
A common theme reported by participants related to signs of occupational stress. One participant illustrated their experience stating: "There is a lot of pressure to complete a lot of tasks with each patient along with caring confidently for the patient and doing home care and getting a room turned around between patients. There is [sic] honestly just too many tasks getting piled up into that one hour and sometimes it feels my license could be at risk because it is hard to meet all of the tasks. My level of stress is super high because I am trying to squeeze every second out of every hour, every day while I'm at work trying to make sure my patients get quality care." "#1 COVID-19, #2 job stress / body stress, and #3 possible retirement before I am ready due to COVID."
Theme 2: Physical Demands
Another theme that emerged as a reason for wanting to leave the field was related to physical demands of dental hygiene practice. Examples of quotes illustrating this theme included "Physical demands on my body. Back pain, hand/ finger pain, arthritis, etc." as well as "hand, shoulder, neck, and back pain."
Theme 3: Negative Work Environment
A negative work environment was also a theme from the respondents. Dental hygienists reported lack of respect by office staff or dentists: Sample quotes for this theme included "… profession not respected by dentist as a collaborating oral health care professional" and "Dentist unappreciative. No respect." A toxic environment was also described by respondents such as "Offices keeping toxic employees who create an environment that it's not easy to change any policy or procedure without major blowback."
Theme 4: Production over Patient Care
The final theme that emerged from open-ended comments was related to production being considered more important than patient care. Examples of this theme included "Push for production over patients' actual needs" and "Change from patient-centered to production centered."
Discussion
The purpose of this study was to examine compassion satisfaction, compassion fatigue, and burnout among clinical DHs and their relationship to demographics and work characteristics. Levels of compassion satisfaction, compassion fatigue, and burnout in DHs and selected demographic and work characteristic variables were shown to be staticallyv significant. In addition, when comparing the ProQoL general quartile cut-points to this study's findings, study participants had a compassion satisfaction (CS) and burnout (BO) score near the 75th percentile range (CS 42 [ProQoL] vs. 44 [study sample] and BO (27 [ProQoL] vs. 26 [study sample]).16 However, participants in this study had a higher 75th quartile for compassion fatigue score at 24 vs. the ProQoL cut-off which was 17.16 This comparison suggests a higher level of compassion fatigue in DHs when compared to other helper professions. This is an unexpected finding and needs further investigation because despite the study sample compassion fatigue score being above the 75th quartile, the standard deviation was less than one SD at 0.43. In addition to further research, the finding regarding compassion satisfaction suggests the importance of self-care to prevent and manage compassion fatigue. Employers could support clinical DHs by offering employee wellness programs.5 In addition, integrating self-care strategies into the entry-level education programs could also serve to support DH students in developing habits that would serve them well once they begin clinical practice.5,23
In the 2016 study by Wu et al., oncology nurses had the following mean ProQoL scores of compassion satisfaction 42.37, compassion fatigue 22.65, and burnout 22.66,14 which were similar to the mean scores of this study. The Han and Kim study found the mean burnout, compassion fatigue, and compassion satisfaction for a sample of Korean DHs trended higher than the values for this study's population.15 These findings suggested the US sample had higher compassion satisfaction, lower compassion fatigue, and lower levels of burnout than the Korean sample of DHs.15
When exploring relationships between outcome variables (compassion satisfaction, compassion fatigue, and burnout) and demographic/work characteristics, the study findings showed greater age to result in higher compassion satisfaction and those working more days per week had lower compassion fatigue.15 It is unknown why compassion fatigue would be lower when working more days per week. Potentially these individuals were more integrated into the office team with more effective teamwork for support, which might reduce stress. The findings related to age and compassion satisfaction in this study were slightly different than those of Han and Kim, who found a significant association between younger age and earlier in their career with burnout, but not compassion fatigue.15 However, the Korean study found years of experience resulted in higher compassion satisfaction,15 which is consistent with this study's findings. Other literature in nursing reported inconsistent findings regarding age and relationship to compassion satisfaction. In some studies, there was no relationship, while in others the findings show lower compassion satisfaction with increased age.24,25 With age comes maturity, confidence, and resilience, which may relate to compassion satisfaction. However, findings from this study may also result from those with higher compassion satisfaction self-selecting to remain in clinical practice whereas those with lower compassion satisfaction experienced burnout and have left clinical practice.
Despite the importance of compassion as it relates to dental hygiene care, there is little reported in the literature related to dental hygiene, with the majority of research related to nursing.1,3-8,11,13,14 Patients have reported that they feel they receive the highest quality of care when their clinician shows compassion.8 Although there is limited literature evaluating the three constructs of the ProQoL in dental professionals, studies have been reported in the literature using the Maslach Burnout Inventory and Oldenburg Burnout Inventory to assess burnout in dentists and dental hygienists.16,18,26-28 Similar to the findings in this study, previous research with dentists and DHs suggests that increases in age result in decreases in burnout. 16,18,26-28 In addition, participants in this study reported higher levels of compassion fatigue (e.g. emotional exhaustion and high workload) which is consistent with other literature suggesting emotional exhaustion and emotional demands along with workload were predictors of burnout for both dentists and DHs.16,18,19,26-28
To expand on the ProQoL findings, participants in this study who had thought about leaving the field were given the opportunity to respond to the open-ended question "What is your reasoning for wanting to leave the dental hygiene profession?" The majority of participants stated that they are burned out or felt under appreciated by staff, management, and dentists. Some stated that they felt extreme pressure to complete multiple tasks while trying to provide the best patient care. These are consistent with the findings of Han and Kim who found DHs negative emotions regarding their workplace can greatly affect overall feelings about their job, thus impacting the quality of patient care.15
The value of using the ProQoL is that it allows for data sharing; raw data from this study will be added to the database from other professions. This not only allows for dental hygiene to be represented in the database, but also allows for the data to become part of the ProQoL general quartile cut points and means along with other health professions.
Further studies on compassion, compassion satisfaction, compassion fatigue, and burnout are needed to explore these concepts in more depth in the dental hygiene profession. In addition, research is needed to identify effective strategies to minimize compassion fatigue to prevent burnout and retain qualified dental hygiene professionals. In addition, given the differences in findings for mean compassion satisfaction, compassion fatigue, and burnout in Korean DHs, further research is needed to explore differences in dental hygiene clinical practice and the issues facing DHs in other countries.
This study had limitations. A non-probability sample was used, limiting the generalizability of the findings. Although social media has advantages including access to a national sample, quick and cost-free delivery of the survey invitation to specific target groups, limitations include limiting access to members of the social media groups, creating selection bias, and the inability to calculate a response rate.29 In addition, the survey research design has limitations related to possible self- report, self-selection, and recall bias. Although the ProQoL instrument has been used in a number of helping professions, it is unknown what compassion fatigue may look like in dental hygiene practice, since some of the secondary trauma items may not fit with the experiences of dental hygienists. Inconsistent word choice related to leaving the dental hygiene profession (e.g., leaving the field, leaving the dental field, leaving the dental hygiene field) may have resulted in misinterpretation of some questions. An inherent limitation of quantitative research is the inability to investigate other causes of compassion satisfaction, compassion fatigue, and burnout in-depth within dental hygiene. However, the open- ended question study allowed for some added depth. A unique situation for this study was also that at the time the survey was implemented, dental hygienists were just beginning to return to work after the initial closure of dental practices due to the coronavirus (COVID-19) pandemic which may have impacted their responses. The many unknowns of a COVID-19 infection, loss of family, friends, and possibly colleagues and patients along with continuing changes to infection control guidelines created additional anxiety.
Conclusion
Findings from this study suggest DHs have high levels of compassion fatigue as compared to nurses and other health professionals. In addition, a significant number of DHs have thought about leaving the profession and nearly one-third planned to leave the dental field within the next five years. Results from this study point to the urgency of identifying strategies to help clinical DHs manage compassion fatigue, including the promotion of supportive work environments with a common patient-centered philosophy, healthy interpersonal relationships with colleagues, and attention to self-care.
Amanda Knutt, RDH, CST, MSDH is a graduate of the master's degree program; Linda D. Boyd, RDH, RD, EdD is a professor and the Associate Dean of Graduate Studies; Jaymi-Lyn Adams, RDH, MS is an assistant professor; Jared Vineyard, PhD is a member of the adjunct faculty; all in the Forsyth School of Dental Hygiene, MCPHS University, Boston, MA, USA.
References
1. Sinclair S, Norris JM, McConnell SJ, et al. Compassion: a scoping review of the healthcare literature. BMC Palliat Care. 2016 Jan 19;15:6.
2. Sinclair S, Hack TF, Raffin-Bouchal S, et al. What are healthcare providers' understandings and experiences of compassion? The healthcare compassion model: a grounded theory study of healthcare providers in Canada. BMJ Open. 2018 Mar 14;8(3):e019701.
3. Lee Y, Seomun G. Compassion competence in nurses. Adv Nurs Sci. 2016 Jun;39(2):E54-66.
4. Lee Y, Seomun G. Role of compassion competence among clinical nurses in professional quality of life. Int Nurs Rev. 2016 Sep;63(3):381-7.
5. Sinclair S, Raffin-Bouchal S, Venturato L, et al. Compassion fatigue: a meta-narrative review of the healthcare literature. Int J Nurs Stud. 2017 Apr;69:9-24.
6. Sorenson C, Bolick B, Wright K, Hamilton R. Understanding compassion fatigue in healthcare providers: a review of current literature. J Nurs Scholarsh. 2016 Sep;48(5):456-65.
7. Sorenson C, Bolick B, Wright K, Hamilton R. An evolutionary concept analysis of compassion fatigue. J Nurs Scholarsh. 2017 Sep;49(5):557-63.
8. Coetzee SK, Klopper HC. Compassion fatigue within nursing practice: a concept analysis. Nurs Health Sci. 2010 Jun;12(2):235-43.
9. Sinclair S, Kondejewski J, Raffin-Bouchal S, et al. Can self-compassion promote healthcare provider well- being and compassionate care to others? Results of a systematic review. Appl Psychol Health Well-Being. 2017 Jul;9(2):168-206.
10. Abendroth M, Flannery J. Predicting the risk of compassion fatigue: a study of hospice nurses. J Hosp Palliat Nurs. 2006 Nov;8(6):346-56.
11. van Mol MMC, Kompanje EJO, Benoit DD, et al. The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: a systematic review. PloS One. 2015 Aug;10(8):e0136955.
12. Maley M. Combatting compassion fatigue with mindfulness. J Dr Nurs Pract. 2018;11(1):52-8.
13. Salmond E, Ames M, Kamienski M, et al. Experiences of compassion fatigue in direct care nurses: a qualitative systematic review protocol. JBI Database System Rev Implement Rep. 2017 Jul;15(7):1805-11.
14. Wu S, Singh-Carlson S, Odell A, et al. Compassion fatigue, burnout, and compassion satisfaction among oncology nurses in the United States and Canada. Oncol Nurs Forum. 2016 Jul 01;43(4):E161-9.
15. Han Y-K, Kim H-H. The relationship among burnout, compassion fatigue, compassion satisfaction and social support of clinical dental hygienists. J Dent Hyg Sci. 2014 Jun;14(2):256-63.
16. Bercasio LV, Rowe DJ, Yansane AI. Factors associated with burnout among dental hygienists in California. J Dent Hyg. Winter 2020;94(6):40-8.
17. Kim Y, Lee E, Lee H. Association between workplace bullying and burnout, professional quality of life, and turnover intention among clinical nurses. PLoS One. 2019 Dec 20;14(12):e0226506.
18. Patel BM, Boyd LD, Vineyard J, LaSpina L. Job satisfaction, burnout, and intention to leave among dental hygienists in clinical practice. J Dent Hyg. 2021 Apr;95(2):28-35.
19. Malcolm N, Boyd L, Giblin-Scanlon L, Vineyard J. Occupational stressors of dental hygienists in the United States. Work. 2020;65(3):517-24.
20. Stamm BH. The ProQoL manual: the professional quality of life: compassion satisfaction, burnout & compassion fatigue/secondary trauma scales [Internet]. Idaho State University, Institute of Rural Health; 2020 [cited June 30, 2020]. Available from:
21. Stamm BH. The concise ProQoL manual, 2nd Ed [Internet]. Idaho State University, Institute of Rural Health; 2021 [cited February 28, 2021]. Available from: https://proqol.org/uploads/ProQOLManual.pdf
22. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, New York: Routledge;1988. 567 p.
23. Krasniqi L, Boyd LD, Giblin-Scanlon L, Vineyard J. Self-care practices of dental hygiene students. J Dent Hyg. 2021 Feb;95(1):76-83.
24. Ruiz-Fernández MD, Pérez-García E, Ortega-Galán ÁM. Quality of life in nursing professionals: burnout, fatigue, and compassion satisfaction. Int J Environ Res Public Health. 2020 Feb 15;17(4):1253.
25. Zhang YY, Zhang C, Han XR, Li W, Wang YL. Determinants of compassion satisfaction, compassion fatigue and burn out in nursing: A correlative meta-analysis. Medicine. 2018 Jun;97(26):e11086.
26. Jeung DY, Lee HO, Chung WG, et al. Association of emotional labor, self-efficacy, and Type A personality with burnout in Korean dental hygienists. J Korean Med Sci. 2017 Sep;32(9):1423-30.
27. Calvo JM, Kwatra J, Yansane A, et al. Burnout and work engagement among US dentists. J Patient Saf. 2021 Aug 1;17(5):398-404.
28. Singh P, Aulak DS, Mangat SS, Aulak MS. Systematic review: factors contributing to burnout in dentistry. Occup Med. 2016 Jan;66(1):27-31.
29. Khatri C, Chapman SJ, Glasbey J, et al. Social media and internet driven study recruitment: evaluating a new model for promoting collaborator engagement and participation. PLoS One. 2015 Mar 16;10(3):e0118899.