You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Dental hygienists play an important role in oral health promotion and disease prevention by serving in a multitude of roles that include the provision of patient care in a variety of clinical settings including direct access care, public health clinics, and dental service organizations (DSO). Dental service organizations are growing in popularity as they provide administrative services to dental practices that are operated by dentists. This type of business model support allows dentists to focus on patient care without worrying about administrative and practice management duties.
Considering the emerging associations between oral and systemic health along with more Americans retaining their teeth for a lifetime, there has been an increasing demand for preventive oral health care.1,2 Dental hygienists are positioned to help meet the 11% growth projection of the Bureau of Labor (2018 - 28), more than double the average 5% growth for all careers in the United States(US).3 While growth for dental hygiene is greater than many other careers, there has been little research conducted to evaluate issues affecting the longevity of dental hygienists, such as job satisfaction (JS), burnout (BO), and intention to leave (ITL).4-6 However, these factors have been shown to be of significant concern in other health care professions, especially in nursing, particularly with longer hours and increases in workloads.7-9 It is important to understand whether longer hours and increased workloads will have a similar effect on dental hygienists as demands in the profession increase.
Literature reveals JS, BO, and ITL influence each another and have similar results.7,10,11 One common finding suggests that autonomy over the health care provider's work and respon-sibilities impacted their JS, BO, and ITL.4,9,10,12 Another common finding was the impact of empowerment on clinicians' attitudes toward their jobs and work performance.8-10,12,13 Autonomy and empowerment were associated with higher JS, which appeared to have the greatest impact on decreasing BO and ITL.9,11,14-16
Several other factors have been shown to influence JS, BO and ITL. Strong leadership and support from management were identified as important factors for clinicians to perform their duties proficiently, and decreased BO and ITL.5,10,11,16 Health care providers also should also have a good work-life balance, without excessively long working hours, to prevent BO and have JS.5,14,15,17 In addition, having adequate staffing to meet the job demand played a key role in JS in order to prevent BO and turnover.9,11,14,16
As the dental hygiene profession grows to help meet the increased demand for preventive care, it is important to understand and explore factors affecting the dental hygiene profession in regard to JS, BO, and ITL. There is a gap in the literature examining the specific career longevity implications for dental hygienists. The purpose of this study was to investigate job satisfaction, burnout, and intention to leave an employment position among dental hygienists and explore the current trends and influencing factors.
Methods
The MCPHS University's Institutional Review Board gave this study exempt status; protocol number IRB121018B. A cross-sectional survey research design was used with a convenience sample of dental hygienists in clinical practice. The web-based survey was administered via SurveyMonkey® (San Mateo, CA). Participants were recruited from Facebook, a popular social media site and widely used in the US. The dental hygiene Facebook groups were identified by using search terms such as dental hygiene, dental hygienist, RDH, and dentistry. Facebook groups with dental hygiene membership of at least 7000 followers were chosen for participant recruitment.
Sample population
The target population for the study was registered dental hygienists who were actively providing patient care in the US. Dental hygienists who had practiced for less than one year or who were no longer actively providing patient care were excluded from the sample. These criteria ensured that the participants would have appropriate amount of experience to provide their perspectives and evaluate the variables. A power analysis was conducted using G*Power. For chi-square test of independence, analysis recommends 133 participants to achieve 80% power to detect a medium effect size using alpha=.05 and five degrees of freedom.
Instrument
Three validated surveys were combined into one instrument for a total of 58 items. The final instrument consisted of Job Satisfaction Survey (36 items); Oldenburg Burnout Inventory (16 items); Turnover Intention Scale (6 items). Each item used a Likert scale to measure the responses and the scales varied from 4- to 6-point scales. Reverse scoring on select items was used to minimize response bias.
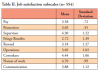
There were nine sub-scales on the job satisfaction items including: pay, promotion, supervision, fringe benefits, contingent rewards, operating procedures, coworkers, nature of work, and communication. The sub-scale Cronbach alpha ranged from 0.60 to .082 with an overall internal consistency of 0.91. The Job Satisfaction Survey had good reliability based on the test-retest correlation with a Cronbach alpha coefficient above 0.70 or an internal consistency above 0.80.18 Validation of the instrument showed a test-retest correlation of 0.71.18 The Oldenburg Burnout Inventory has been shown to have good reliability in assessing burnout.19,20 Internal consistency for the sub-scales was shown to be 0.73 to 0.87 for exhaustion and 0.81 to 0.83 for disengagement.19,20 The Turnover Intention Scale also demonstrated good reliability and validity.21 Previous studies showed a test-retest correlation of 0.895 to 0.913.22,23 Since this study intended to measure dental hygienists with working experience of at least one year, there is the possibility of loss of some reliability, as the instrument was reported to have the most reliability when completed within the first 6 months of employment. 24
Procedure
After gaining permission from the Facebook page administrators, an invitation to participate in the research was posted on the group pages with a link to web-based survey platform. Participants were required to read and agree to the informed consent document in order to access the survey. The survey was estimated to take 15 to complete. A follow up invitation was posted one week after the initial invitation to participate. No participation incentives were provided.
Statistical Analysis
Descriptive analysis was used for the data collected using the Likert scale for items and to evaluate normality and linearity. Mean, median, and frequency were used for the continuous variables to simplify the large amount of data. Using the frequency distribution, the data was categorized or used as individual values. Standard deviation was used as a measure for variance to help estimate the amount of dispersion of data. Internal consistency was measured by using Cronbach's alpha of 0.7 and the covariance was also measured between two variables. Multiple variable regression was used to help predict the dependent values of an independent variable based on two or more variable values. The interval estimate used was 95% confidence interval (95% CI). In addition, the probable value (pvalue) was set to 0.05. The last analysis used was the chi-squared test (χ²) to understand the likelihood the observed distribution was due to chance. The data was analyzed using SPSS 23 (IBM, Armonk, NY).
Results
A total of 723 individuals opened the survey link; and the completion rate was 77% (n=554). Most participants were employed in private practice (87%) and worked more than 3-4 days a week (89%). A little less than half of participants (41%) had been practicing for fewer than 10 years. Demographic information is shown in Table I.
Coding of the Job Satisfaction Survey was arranged so higher values indicated higher job satisfaction. Each subscale was calculated by averaging responses after reverse coding was completed. Participants job satisfaction averaged slightly above the neutral response for supervisors (M=4.30, SD=1.22), coworkers (M=4.44, SD=1.06), and the nature of the work (M=4.70, SD=1.11). Provision of fringe benefits (M=2.72, SD=1.39) was the only response to fall below the neutral response point. Over 68% disagreed with the statement "we receive benefits as good as most other organizations" and 77% agreeing with the statement "there are benefits we do not have which we should have". The nine subscales showed excellent reliability (α=0.83). The nine subscales were combined into a total job satisfaction scale by averaging all items into a single score (M=3.80, SD=0.70). The averages and standard deviations for all Job Satisfaction Survey subscales are displayed in Table II.
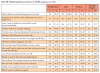
The Oldenburg Burnout Inventory contained disengagement and exhaustion subscales; higher values indicated more disengagement and exhaustion in the workplace. Both subscales were calculated using the average response for the items related to the respective scales. On average, participants fell below the neutral mid-point response for disengagement (M=2.41, SD=0.55) and exhaustion (M=2.33, SD=.54), indicating that participants did not experience disengagement or exhaustion in the workplace. Responses to each of the Oldenburg Burnout Inventory items are
One-way ANOVA and independent sample t-tests were conducted to investigate mean differences between categories of demographic variables. There were statistically significant differences in mean job promotion/job satisfaction (F(2, 554)=7.43, p=0.001) and fringe benefit satisfaction (F(2, 554)=8.55, p<0.001). Post-hoc comparisons using Tukey's HSD showed participants working less than 3 days a week had higher job promotion/job satisfaction (M=3.94, SD=0.67) than those working three to four days (M=3.68, SD=0.50, p=0.001) or those working five days or more (M=3.63, SD=.56, p=0.001). Participants employed in the working three to four and five plus days per week categories, did not have a significant difference in mean satisfaction levels (p=0.65). For fringe benefits, participants working fewer than three days a week (M=2.23, SD=1.16) had lower job satisfaction than those working three to four days a week (M=2.65, SD=1.36) and those working five days or more (M=3.05, SD=1.49, p=0.001). Participants in the three to four and five or more days per week groups did not have statistically different means (p=0.07). Participants working in a DSO setting were compared to participants in all other practice types using independent t-tests. Participants who were DSO employees indicated greater satisfaction with opportunities for promotion (M=3.70, SD=0.54) than participants employed in other settings (M=3.44, SD=0.61, p=0.02). The DSO participants were also more satisfied with their fringe benefits (M=3.98, SD=1.19) than non-DSO participants (M=2.65, SD=1.37, p<0.001). All other comparisons for demographic variables were non-significant (p>0.05).
Five separate linear regression models were calculated to determine if overall JS, disengagement, and exhaustion predict responses to the five intention and attitude questions (Table IV). The linear regression model indicated all five models were statistically significant. Job satisfaction was a significant predictor in four of the five models, except for the frequency of looking forward to another day at work. Higher JS predicted lower frustration about opportunities to achieve work related goals (p<0.05), consideration about leaving a current employer (p<0.001), and willingness to accept an equal job offer (p<0.001). Satisfaction predicted higher frequency of looking forward to another day at work. Disengagement was a significant predictor in all five models. Higher average disengagement responses predicted more frustration (p<0.001), consideration about leaving a current employer (p<0.001) and predicted a lower frequency of looking forward to another day at work (p<0.001). Exhaustion was a significant predictor in all models except for being frustrated when not given an opportunity to achieve personal work-related goals. Exhaustion followed the same predictive pattern as disengagement. Results of regression analysis including beta values are shown in Table V.
Discussion
Dental hygienists play an important role in the management of the patient's preventive oral care; however, there is little research investigating career longevity issues such as JS, BO, and ITL in the dental hygiene profession. Results from this study identified several trends influencing JS, BO, and ITL among dental hygienists. First, job satisfaction had a strong influence on intention to leave in this population, similar to research conducted among registered nurses.10,12 A second finding was that burnout, characterized by exhaustion and disengagement, also has a strong influence on ITL. Third, disengagement had a stronger influence than exhaustion on BO based on the predictors used in this study. Previous research conducted among registered nurses demonstrated that JS, BO, and lTL correlated with one another and was very similar to the findings in this study.7-9
Job satisfaction showed several key trends in the analysis. First, this research found dental hygienists who felt less frustrated were more satisfied with their work and less likely to consider leaving a job or accepting another position. While frustration was not defined in the survey it could result from multiple factors such as job demand, time pressure, stress, or feeling overloaded or overwhelmed by work. Previous research has reported these factors were also of important indicators of job satisfaction in nursing. 7,9,10,12
INSERT TABLE 5In this study, respondents were only slightly satisfied with pay and rewards. As reported in the literature for nursing and physician assistants, poor reward systems and pay can result in dissatisfied employees and increased turnover.9,25,26 The correlation to increased turnover has the potential to impact the overall patient care experience in addition to having economic implications for employers.9,27 Fringe benefits also played a significant role in JS (p<0.001) for the study participants. Although the specific benefits were not identified, some possibilities may include medical and dental insurance, educational assistance, paid vacation, paid sick time, or retirement (e.g. 401(k) retirement account). Research conducted among other health professions has indicated that health insurance and other fringe benefits have been significantly associated with job satisifaction.28,29 In this study, participants working fewer than three days a week were less satisfied with fringe benefits than participants employed four or more days. This could be related to the respondents employed more than four days a week were more likely to meet the minimum hours required to receive fringe benefits.
Participants employed by a DSO were more satisfied with opportunities for promotion (p=0.02) and fringe benefits (p<0.001) than non-DSO participants, similar to findings reported from a survey of dentists.30 Dental service organizations contract with dental practices to provide management support with non-clinical operations. In the DSO corporate structure, dental hygienists have opportunities to explore careers outside of clinical practice including mentoring, education, practice management, or career opportunities with the corporate office. Furthermore, these non-clinical positions can be offered as promotions that include pay raises, bonuses, or incentives. Fringe benefits are also more common in the DSO employment model.
Operations or organizational structure was also an area where respondents reported only slight satisfaction in the Job Satisfaction Survey. Organizational structure may include formalization of policies and procedures; participation in decision-making; and opportunities for growth. Operations in a dental practice include, but are not limited, the workforce or staffing, work hours/shifts, and work-life balance, all important aspects of preventing burnout and increasing job satisfaction. Research has shown that an organizational structure with good management, support staff, and leadership can also lead to higher job satisfaction in health care settings.10, 12
In any health care environment, communication is critical among team members as a lack in communication can lead to frustration, job dissatisfaction, impact retention, and ultimately impact patient care.14 When effective teamwork and communication is utilized, it can help with workflow, reduce errors, and increase productivity.31 Results from this showed only slight satisfaction with communication, which is an area that requires further exploration as it was inconsistent with findings in other health professions such as nursing.14
Regression models indicated disengagement was related to frustration with personal work-related goals (p<0.001), considering leaving a job (p<0.001), likelihood of accepting another job (p<0.001), satisfaction of personal needs (p<0.05), and looking forward to another day at work (p<0.001). Employers understanding the goals and needs of the individual dental hygienist and offering opportunities for growth could address some of these predictors for disengagement. A possible way to overcome disengagement may include supporting the dental hygienist's autonomy in decisions related to providing quality preventive care and fully utilizing the scope of practice allowed in the state, such as administering local anesthetics; administering nitrous oxide; and placing and finishing restorations.4,8,31 In addition, a majority of states (42) allow for the delivery of dental hygiene care in alternative practice settings.32 A dental practice could consider engaging appropriately qualified dental hygienists to go to these settings to provide preventive care as personalized outreach for their practice.32 Allowing for dental hygienists to practice to the full-extent of their education and license can lead to greater engagement and retention.
When examined exclusively, exhaustion appeared to add to the indicators of considering leaving a job (p<0.05), the job satisfying personal needs (p<0.05) and looking forward to another day at work (p<0.05). Understanding the causes of mental and physical fatigue are key factors for identifying ways to prevent and/or manage BO. A previous study reported that 29% of the dental hygienists experienced BO due to factors including difficult or demanding patients, work-life balance, and long hours.5 Burnout may also be a result of factors such as accelerated dental hygiene schedules, shorter patient appointment times, inadequate lunch breaks, or lack of staff support.
There were limitations to this study. Use of a non-probability sample from targeted social media groups, limits generalizability. Many surveys were not completed, which may have been due to the length of the survey. Self-report bias may have also influenced the participant responses. Another concern was possible misinterpretation of survey terminology, such as confusion in interpretation of the question or rating for the Likert scale. As the majority of the participants worked in private practice, limiting the understanding of other types of employment settings. Future research should investigate the factors with the greatest impact in preventing burnout and improving job satisfaction and include a wider range of practice settings. Based on the findings from this study, further research on the DSO employment setting and career longevity are warranted. Given that this research was completed prior to the COVID-19 pandemic, changes in job satisfaction, burnout, and intention to leave among clinical dental hygienists are unknown and need further investigation.
Conclusion
Results from this study suggest that there is overall job satisfaction amongst dental hygienists in clinical practice with the exception of the lack of fringe benefits and opportunities for promotion in the job setting. Overall satisfaction with employment and burnout were shown to be influencers for leaving a clinical dental hygiene position. Findings suggest that employers should explore ways to support dental hygienists in meeting their work-related goals for continued growth and career longevity. A proactive approach in addressing factors impacting burnout and dental hygienists' intent to leave their positions may ultimately contribute to improved patient care and positive oral health outcomes.
Badal M. Patel, RDH, MS is a graduate of the Master of Science in Dental Hygiene program; Linda D. Boyd, RDH, RD, EdD is a professor and the Associate Dean of Graduate Studies; Jared Vineyard, PhD is an adjunct faculty member; Lisa LaSpina, RDH, DHSc is an associate professor; all at the Forsyth School of Dental Hygiene, MCPHS University, Boston, MA, USA.
Corresponding author: Linda D. Boyd, RDH, RD, EdD; linda.boyd@mcphs.edu
References
1. Seitz MW, Listl S, Bartols A, et al. Current knowledge on correlations between highly prevalent dental conditions and chronic diseases: An umbrella review. Prev Chronic Dis. 2019 Sep 26;16:E132.
2. Dye B, Thornton-Evans G, Li X, Iafolla T. Dental caries and tooth loss in adults in the United States, 2011-2012. NCHS Data Brief. 2015 May(197):197.
3. Bureau of Labor Statistics, U.S. Department of Labor. Occupational Outlook Handbook, Dental Hygienists [Internet]. Washington (DC): U.S. Department of Labor; 2021 [updated 2021 Feb18; cited 2019 Oct 24]. Available from: https://www.bls.gov/ooh/healthcare/dental-hygienists.htm#tab-6.
4. Turner S, Ross MK, Ibbetson RJ. Job satisfaction among dually qualified dental hygienist-therapists in UK primary care: a structural model. Br Dent J. 2011 Feb 26;210(4):E5.
5. Gorter RC. Work stress and burnout among dental hygienists. Int J Dent Hyg. 2005 May;3(2):88-92.
6. Gibbons DE, Corrigan M, Newton JT. A national survey of dental hygienists: working patterns and job satisfaction. Br Dent J. 2001 Feb 24;190(4):207-10.
7. Adriaenssens J, de Gucht V, Maes S. The impact of traumatic events on emergency room nurses: findings from a questionnaire survey. Int J Nurs Stud. 2012 Nov;49(11):1411-22.
8. Cicolini G, Comparcini D, Simonetti V. Workplace empowerment and nurses' job satisfaction: a systematic literature review. J Nurs Manag. 2014 Oct;22(7):855-71.The Journal of Dental Hygiene 35 Vol. 95 • No. 2 • April 2021
9. Halter M, Boiko O, Pelone F, et al. The determinants and consequences of adult nursing staff turnover: a systematic review of systematic reviews. BMC Health Serv Res. 2017 Dec 15;17(1):824.
10. Saber DA. Frontline registered nurse job satisfaction and predictors over three decades: a meta-analysis from 1980 to 2009. Nurs Outlook. 2014 Nov-Dec;62(6):402-14.
11. Daouk-Oyry L, Anouze AL, Otaki F, et al. The JOINT model of nurse absenteeism and turnover: a systematic review. Int J Nurs Stud. 2014 Jan;51(1):93-110.
12. Squires JE, Hoben M, Linklater S, et al. Job satisfaction among care aides in residential long-term care: a systematic review of contributing factors, both individual and organizational. Nurs Res Pract. 2015;2015:157924.
13. Li H, Shi Y, Li Y, et al. Relationship between nurse psychological empowerment and job satisfaction: A systematic review and meta-analysis. J Adv Nurs. 2018 Jun;74(6):1264-77.
14. Chan ZC, Tam WS, Lung MK, et al. A systematic literature review of nurse shortage and the intention to leave. J Nurs Manag. 2013 May;21(4):605-13.
15. Elbarazi I, Loney T, Yousef S, Elias A. Prevalence of and factors associated with burnout among health care professionals in Arab countries: a systematic review. BMC Health Serv Res. 2017 Jul 17;17(1):491.
16. Lartey S, Cummings G, Profetto-McGrath J. Inter-ventions that promote retention of experienced registered nurses in health care settings: a systematic review. J Nurs Manag. 2014 Nov;22(8):1027-41.
17. Calvo JM, Kwatra J, Yansane A, et al. Burnout and work engagement among US dentists. J Patient Saf. 2017 Jun 30. Online ahead of print.
18. van Saane N, Sluiter JK, Verbeek JH, Frings-Dresen MH. Reliability and validity of instruments measuring job satisfaction--a systematic review. Occup Med. 2003 May;53(3):191-200.
19. Demerouti E, Bakker AB, Vardakou I, Kantas A. The convergent validity of two burnout instruments: A multitrait-multimethod analysis. Eur J Psychol Assess. 2003;19(1):12-23.
20. Reis D, Xanthopoulou D, Tsaousis I. Measuring job and academic burnout with the Oldenburg Burnout Inventory (OLBI): factorial invariance across samples and countries. Burnout Res. 2015;2(1):8-
21. Du Plooy J, Roodt G. Work engagement, burnout and related constructs as predictors of turnover intentions. SA J Ind Psychol. 2010;36(1):1-13.
22. Jacobs EJ. The development of a predictive model of turnover intentions of professional nurses [doctoral thesis]. [Johannesburg (South Africa)]: University of Johannesburg; 2007. 459 p.
23. Martin A, Roodt G. Perceptions of organisational commitment, job satisfaction and turnover intentions in a post-merger South African tertiary institution. SA J Ind Psychol. 2008;34(1):23-31.
24. Bothma FC, Roodt G. Work-based identity and work engagement as potential antecedents of task performance and turnover intention: Unravelling a complex relationship. SA J Ind Psychol. 2012;38(1):27-44.
25. Palmer SP. Nurse retention and satisfaction in Ecuador: implications for nursing administration. J Nurs Manag. 2014 Jan;22(1):89-96.
26. Hooker RS, Kuilman L, Everett CM. Physician assistant job satisfaction: A narrative review of empirical research. J Physician Assist Educ. 2015 Dec;26(4):176-86.
27. Reddy A, Pollack CE, Asch DA, et al. The effect of primary care provider turnover on patient xxperience of care and ambulatory quality of care. JAMA Intern Med. 2015 Jul;175(7):1157-62.
28. Ofei-Dodoo S, Long MC, Bretches M, et al. Work engagement, job satisfaction, and turnover intentions among family medicine residency program managers. Int J Med Educ. 2020 Feb 28;11:47-53.
29. Yoon S, Khan MM. The effect of organizational values, work-related compensation, and benefits on job satisfaction of home health aides. Home Health Care Manag Pract. 2020 May; 32(2): 95-104.
30. Lo Sasso AT, Starkel RL, Warren MN, et al. Practice settings and dentists' job satisfaction. J Am Dent Assoc. 2015 Aug;146(8):600-9.
31. Oral Health Workforce Research Center. Variation in dental hygiene scope of practice by state [Internet]. Rensselaer (NY): Center for Health Workforce Studies; 2019 [cited 2019 October 25]. Available from: http://www.oralhealthworkforce.org/resources/variation-in-dental-hygiene-scope-of-practice-by-state/.
32. ADHA. Direct access[Internet] Chicago ( IL): American Dental Hygienists' Association; 2018 [cited 2019 October 25]. Available from: https://www.adha.org/direct-access.