You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
According to Khan and Omar,1 "Teledentistry (TD) can be defined as "the remote provision of dental care, advice, or treatment through the medium of information technology, rather than through direct personal contact with any patient(s) involved." It is a field whose roots lie in telemedicine. Telehealth is a broader term that includes telemedicine and TD. According to the website glossary of the American Telemedicine Association, now known as ATA, telehealth "is often used to encompass a broader definition of remote healthcare that does not always involve clinical services. Videoconferencing, transmission of still images, e-health including patient portals, remote monitoring of vital signs, continuing medical education and nursing call centers are all considered part of telemedicine and telehealth."2
The initial TD concept was developed as part of the blueprint for dental informatics drafted at a 1989 conference in Baltimore, funded by the Westinghouse Electronic Systems Group.3 The United States (US) Army's Total Dental Access (TDA) project in 1994 was considered to be at the forefront of the birth of TD. A traditional Plain Old Telephone System (POTS) was utilized with two different communication methods, real time, and store and forward.3 In 1995, Rocca and colleagues conducted a pilot study in Haiti to connect a general dentist with a dental specialist in Washington DC, via a satellite link.4 The following year, an integrated services digital network (ISDN) - based TD was tested by the Department of Defense to establish a medical network in Bosnia to connect Army field dentists with dentists at five regional military medical centers in the US (Washington, Texas, California, District of Columbia, and Hawaii). Using commercially available technology, dentists transmitted radiographs, color images and full motion videos to remote field hospitals for diagnostic support. The main TD hub was at the Landstuhl Regional Medical center in Germany, where the data was integrated into the Internet and the commercial ISDN gateway link to the world.4 In 1997, ISDN-based TD was tested in Belgium, Italy and Germany; subsequently, additional studies were conducted in the UK, Japan and Taiwan.5
Teledentistry has been used in several parts of the US, to increase access to care and provide screenings and referrals for vulnerable and underserved populations in locations such as school and preschool settings, nursing homes and rural clinics.6,7 It is also used in education for health professionals and continuing education.3 Systematic reviews of the literature have demonstrated favorable results regarding diagnostic accuracy between TD and other assessment methods for the detection of early childhood caries in preschool children.8,9 A randomized clinical trial compared TD to conventional screening and referral methods for new patients seeking orthodontic treatment.10 There was moderate agreement, kappa = 0.46, between the two methods in patients being accepted for orthodontic treatment.10
The diagnostic efficacy of TD in oral diagnosis was demonstrated by comparing the TD diagnosis of oral lesions among nursing home residents with the reference standard diagnosis obtained from a clinical exam.11 Teledentistry is also being used by dentists for consultations and referrals with dental specialists12,13and specialist supervision. One example is orthodontic treatment performed by general dentists but supervised remotely by orthodontists.14 In Brazil, a cloud-based telediagnosis program, EstomatoNet, has been used for specialists to advise primary care dentists and physicians about their patients' oral mucosal lesions and whether referrals to specialists are recommended. This program greatly reduced the need for face-to-face consultation, an advantage where there are few specialists and long waiting and travel times for patients.15 While a number of studies have evaluated the clinical aspects of TD, few studies have evaluated its economic impact or cost-effectiveness.16
In 2019, 2.4 million North Carolinians, almost a fourth of the population, resided in 175 dental health professional shortage areas located throughout the state.17,18 Many of these counties are largely rural, creating a need for reaching people with limited access to dental care who could potentially benefit from TD. In contrast, one study of telemedicine utilization in an insured population found that telemedicine is frequently used in urban areas where convenience may be the driving factor rather than limited access to care.19 Thus, TD benefits both those who need better access to dental care as well as the larger population who have access but also seek convenience.
Teledentistry models vary, but they typically employ several team members to support data collection, analysis, and provision of care. Dental hygienists are well positioned to facilitate screening, counseling, and referral in support of TD initiatives. Depending on state practice acts and additional training, some may provide preventive and therapeutic measures as well. The utilization of dental hygienists is essential in establishing a team focused on prevention and education, in addition to the identification of dental disease and treatment needs.
Although TD has been in existence for over 30 years, it is relatively new in North Carolina (NC). The current environment for TD is more restrictive than many other states due to current state legislative regulations and policies. In order to learn more about TD and share ideation, a task force held the first statewide summit in October 2018. Participants included individuals holding positions with the ability to overcome current challenges and advance TD, if desired. The goals of the Summit included increasing participants' knowledge and understanding of TD, reimbursement and regulatory policies, information technology options, benefits, challenges and solutions. The purpose of this study was to compare participants' pre- and post-Summit self-reported knowledge and attitudes toward TD, the potential role of dental hygienists, and to determine priorities for overcoming barriers to implementation.
Methods
The study was reviewed by the University of North Carolina at Chapel Hill (UNC) Office of Human Research Ethics and determined exempt (Study #18-2039). A planning committee and professional facilitator led the planning and implementation of the Summit. The individuals invited to the Summit (n=77) included experts in telemedicine, information technology, oral health and related policy, leaders in dental education, advocacy, business, organized dentistry and dental hygiene, representatives from health insurers, foundations and legislators and selected UNC students (8 dental students, 1 dental hygiene student, and 1 dental hygiene master's student). The Summit consisted of oral presentations describing the use of telemedicine and UNC's Health Care's 24/7 Virtual Urgent Care Center in NC,20 a video TD demonstration, and the role of TD in California in the provision of the Virtual Dental Home System of Care in community sites.21 Six afternoon breakout groups were held with the following topics: 1) private practice, 2) community, 3) education, 4) information technology, 5) policies, and 6) finance/reimbursement. Participants were asked to address key questions in each of their domains and share highlights of each group's discussion.
The survey questions were developed by a subset of the planning group. Pilot-testing was conducted with 3 individuals who were invited but had indicated, prior to the pilot-testing, that they were unable to attend the event. Pre-Summit surveys were distributed via e-mail using online software (Qualtrics®; Provo, UT) to the individuals who indicated that they planned to attend the Summit (n=77). Post-surveys were sent to the Summit attendees (n=67). The e-mail described the survey and confidentiality process; consent was indicated by clicking the survey link. The initial pre-Summit survey mailing was sent twice, ten and four days before the event. Post-Summit survey e-mails were sent two and four weeks following the event. No names were recorded on the surveys. To maintain confidentiality and permit matching of individual pre- and post-Summit surveys, the initial five questions on the surveys were used for each respondent to create a unique ID (i.e., what is the first letter of your favorite color). Questions regarding participants' professional roles were only asked on the pre-Summit survey.
Respondents evaluated the format and content of the program in the post-Summit survey. The surveys consisted of questions asking participants to rate the extent of their overall knowledge about TD, and extent of their current knowledge of NC telemedicine policies for Medicaid reimbursement (a joint state and federal funded program that assists low-income families with healthcare, including basic dental services), each on a scale of 1 (no knowledge) to 7 (very knowledgeable. Responses were grouped from 1-4 and 5-7 to create a derived binary variable for analysis.
Participants were asked to rank the extent to which TD should be developed in NC, and the extent to which dental hygienists should have a role in the delivery of services through TD in NC ranging from 1 (not at all) to 5 (a great deal). Responses 1-3 and 4-5 were grouped. Three sets of questions and response options asked: "What issues do you think TD can address in NC?", "In what ways do you think TD could be used in NC?", and "There are many challenges for implementing and delivering TD services in NC. Which one do you think should be addressed first?"
Statistical analysis
The analytical dataset was limited to information from respondents with pre- and post-survey ID matches. The analysis included descriptive statistics for each variable, comparison of frequency distributions for categorical variables, and exact McNemar's matched pair test to compare pre- and post-Summit proportions of the participants' responses to the surveys. Multi-level responses were converted to binary responses for comparison due to the small sample size. For the question regarding the challenge to be addressed first, the comparison was whether a choice was selected or not. Each of the pre- and post-survey questions were analyzed separately; first ignoring whether or not the participants were involved in patient care (practicing clinicians) or had other roles. Subsequent analyses were performed to determine whether results differed by the "practicing clinician" (yes/no) classification. The 95% confidence intervals associated with each difference (increase) in proportion were reported. A sensitivity analysis was conducted to assess whether conclusions changed if students were classified as practicing clinicians or not. A 5% statistical significance level was used for the comparison of the proportions. SAS version 9.4 (TS1M1 SAS Institute Inc.; Cary, NC, USA) was used for the data analyses.
Results
The pre-Summit and post-Summit response rates were 75.3% and 70.1% respectively. However, not all of the pre- and post-Summit surveys (62.7%, n=42) could be matched, as not everyone completed both surveys. Of those who completed the post-Summit surveys, not all of the participants provided consistent responses to the five questions needed to create their unique identifier. The results assessing pre- and post-survey change are based on 42 participants, including eight students. A comparison of the characteristics of these 42 and all 58 who completed the pre-Summit survey was performed and the frequency distributions were found to be very similar (Table I).
Participant characteristics
Of the participants with matched pre-post data (n=42), about half, (47.6%) reported that their primary role was in administration, 21.4% teaching and mentoring, 12.0% patient care. Students comprised 19.0% of the data set. Of the participants who were not students, 32.0% were currently practicing clinicians; others were educators or administrators.
Changes in self-reported knowledge and attitudes
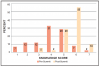
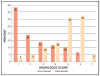
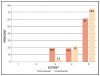
Overall, self-reported knowledge about TD significantly increased pre- (38.1%) to post-Summit (92.9%) as indicated by respondents providing a knowledge score of 5-7, p<0.001 (Figure 1, Table I). There was also a significant increase in knowledge about NC telemedicine policies for Medicaid reimbursement; 16.7% of participants provided responses from 5-7 pre-Summit, increasing to 69.1% post-Summit, p<0.001 (Figure 2, Table II). The majority, 78.6%, indicated in the pre-Summit survey that TD should be developed in NC, providing scores of 4-5; the proportion increased to 95.2% post-Summit, p=0.065 (Figure 3, Table II). Responses regarding the extent to which dental hygienists should have a role in the delivery of services in NC, was high at both time points, (83.3% pre- and 88.1% post-), thus the change was not significant, p=0.727.
Teledentistry issues and utilization
Responses to the nine issues that TD can address in NC were favorable at both time points. Pre-Summit, all participants responded "yes" to seven items: increasing access to care and patient outreach, efficient use of clinician's and patient's time, improving oral health in rural NC, facilitating consultation with health care specialists, and reducing patients' travel costs. Almost all respondents agreed with the remaining two items; TD can increase reimbursement to dentists by provision of more services (97.6%) and TD can increase the number of dentists who are prepared to treat patients in NC's rural/underserved communities (85.7%). There were minor variations in the responses post-Summit, with 100.0% responding "yes" to four of the same issues, and 88.1% to 97.6% responding "yes" to the remaining issues.
Participants were asked about seven possible ways that TD could be used in NC (Table III). Pre-Summit, 92.9% responded that it could be used in the following ways: 1) synchronous use such as for real-time patient consultations, 2) asynchronous use called, "store and forward" to send patient information for specialty consultation, and 3) patient education. A majority, 88.1%, indicated that it could be used for mHealth (mobile health such as smart phones/iPads for monitoring patient health) or oral health screening (i.e., schools, nursing homes, prisons) and for continuing education (85.7%). The greatest response change was for Remote Patient Monitoring (RPM) such as for patients in an intensive care unit in a distant location; pre-Summit (71.4%) and post-Summit (95.2%). For the remaining items, post-Summit responses ranged from 78.6% to 100.0%. Asynchronous use was the only item where the proportion of affirmative responses declined, from 92.3% to 78.6%, reflecting current statutory regulations.
Challenges
Participants were given a list of seven challenges for implementing and delivering TD services in NC and asked which one should be addressed first (Table IV). Both pre- and post-Summit, the most frequent challenge reported was the "state practice act requiring direct supervision of dental hygienists, limiting their TD use in community settings." This challenge was selected by 33.3% (pre-Summit) and 59.5% (post-Summit), a significant increase compared to all other responses, p=0.013 (Table II, Table IV). Because respondents were asked to select one challenge, the increase in the state practice act category was balanced by decreases in some of the other categories such as reimbursement issues. Further examination was performed on whether the choice of state practice act regarding dental hygiene varied between those self-identified as practicing clinicians vs other professional roles. The pre-post change in proportions was a little larger for practicing clinicians than others, but was not significant for either group, p=0.063 (95% CI: 0.05, 0.72) and p=0.147 (95% CI: 0.30, 0.63), respectively.
Student classification sensitivity analysis
Students could have self-identified as practicing clinicians or not. Students were not asked to indicate their year of enrollment in their respective programs. The sensitivity analysis compared findings as if all the students had been classified as practicing clinicians or not and indicated that the conclusions did not change regardless of how the students were classified.
Discussion
Dental hygienists are powerful advocates for the community and are vastly underutilized when addressing access to care needs. Teledentistry is a model that can incorporate utilization of dental hygienists to screen, counsel, and refer; addressing both preventive needs and connection to a dental care provider. A major finding of this study was the significant increase in identifying the NC State Practice Act as the first challenge to be addressed to implement TD among the Summit respondents. The scope of practice for dental hygienists in NC is one of the most restrictive in the nation, requiring direct, onsite supervision of dental hygienists and a prior dentist examination.22 Unique circumstances can allow for indirect supervision of dental hygienists, but a prior examination by a dentist is always required.
Teledentistry can provide an alternative method to the current on-site clinical examination process. The findings provide impetus for working with the legislature, to make modifications, so that dental hygienists can play a key role in the implementation of TD. The virtual dental home model in California is a successful example of dental hygienists being a key part of the TD team.23
In a TD literature review that included evaluation of clinical outcomes and costs, Daniel et al found that different types of oral health care personnel have been used to conduct remote clinical screenings and capture intraoral images. The authors discussed that "expanding the roles of dental hygienists and removing practice restrictions would increase the number of oral health care providers who could perform screenings, care and referrals using TD."24 A Tennessee study comparing decayed and filled surface (DFS) scores of 4-7-year-old children obtained by a dentist and dental hygienist using clinical methods versus a dentist and dental hygienist using TD (intraoral photographs) methods found that the DFS scores between the two groups and methods were not significantly different, p>0.10.25 Studies comparing larger numbers of dentists' diagnoses via TD and hygienists' screening assessments may be needed.
A key barrier to the implementation of TD practices has been found in the restrictive dental practice acts that states, such as NC, place on the roles and functions of dental hygienists. Teledentistry can be used as an effective tool for conducting a remote consultation between a patient at the originating site and a consulting provider at the distant site. Its benefits lie in the convenience for both patient and provider, improving access to care for those who reside in rural and underserved communities, avoidance of having to travel considerable distances and the knowledgeable triaging of patient referrals.
A 2014 TD survey of Australian dental practitioners supports the findings of this study. Authors expressed agreement with its advantages and usefulness for patients, especially those in rural locations, and aspects of dental practice including communication with patients, colleagues and facilitation of referrals. Concerns were expressed regarding data security, patient consent and privacy, equipment costs and technical compatibility,26 indicating mutual issues to address in order for TD to advance globally. A systematic review of multinational barriers to adopting telemedicine also identified similar barriers for TD, in addition to high cost, lack of reimbursement, and public policy barriers regarding state provider licensing and inter-state commerce restrictions in the United States.27
This study had limitations. Since the Summit participants were invited and agreed to attend an all-day event, they may have been more likely to be interested in learning about the topic and predisposed to having more favorable attitudes towards TD than individuals who were not invited to attend. Regardless, initial self-reported TD knowledge was relatively low among the invitees. While these results do not reflect TD knowledge of NC residents or clinicians at large, it would also be likely to be low. To advance TD, more extensive communication and education to both lay and clinician audiences will be necessary.
Not all attendees completed the post-Summit survey or remembered the responses they provided on the pre-survey to create a code that could be used for the identifier to match the post-survey. Thus, the number of matched pairs to assess differences before and after the Summit was limited to a subset of the total number of participants. However, the pre-Summit survey distributions of characteristics for all respondents (n=58) were similar to those used in the analytical matched sample (n=42). The number of dental hygienists or dental hygiene students who attended the Summit was small (n=2). It is not known if they completed the survey. While the dental hygienist perspectives regarding TD were of interest, in order to maintain confidentiality, the responses were not segregated.
Conclusions
Teledentistry Summit participants' self-reported knowledge was high following the event and attitudes were found to be favorable for moving forward with TD in NC. Respondents indicated that TD should be developed in NC and could address many issues to improve patient care. The majority felt dental hygienists should have a role in TD and that the state practice act governing their scope of practice was the first challenge that should be addressed.
Disclosure
The following organizations provided sources of support for the Summit: BlueCross BlueShield of North Carolina Foundation, The Duke Endowment, Delta Dental of North Carolina, the North Carolina Dental Society, and the University of North Carolina at Chapel Hill Adams School of Dentistry, Office of the Dean. The authors received no financial support for the research, authorship and/or publication of this paper.
About the Authors
Jane A. Weintraub, DDS, MPH is the Rozier Douglass Distinguished Professor in Dental Public Health, Division of Pediatric and Public Health, Adams School of Dentistry and Gillings School of Global Public Health; Leiana R. Edwards, BS was the Operations Supervisor of the Office of Teledentistry, Office of the Dean, Adams School of Dentistry; Jennifer L. Brame, RDH, MS is an associate professor and the Director of the Graduate Dental Hygiene Education and Dental Hygiene Programs, Division of Comprehensive Oral Health, Adams School of Dentistry; Lewis Lampiris DDS, MPH was an associate professor and the Assistant Dean for Community Engagement and Outreach, Division of Pediatric and Public Health, Adams School of Dentistry; B. Alex White DDS, DrPH is an associate professor, Department of Health Policy and Management, Adams School of Dentistry and Gillings School of Global Public Health; Reuben Adatorwovor, PhD is an assistant professor, Department of Biostatistics, College of Public Health, the University of Kentucky and formerly a doctoral student in the Department of Biostatistics, Gillings School of Global Public Health; N. Shaun Matthews DDS, MD is an associate professor and the Director of Telehealth, Division of Craniofacial and Surgical Care, Adams School of Dentistry; all at the University of North Carolina at Chapel Hill, Chapel Hill, NC.
Corresponding author: Jane Weintraub, DDS, MPH; Jane_Weintraub@unc.edu
References
1. Khan SA and Omar H. Teledentistry in practice: literature review. Telemed J E Health. 2013 Jul;19(7):565-7.
2. ATA. Telemedicine glossary [Internet]. Arlington: ATA; c2018 [cited 2019 July 12]. Available from: https://www.americantelemed.org/resource/reference/
3. Chen JW, Hobdell MH, Dunn K, et al. Teledentistry and its use in dental education. J Am Dent Assoc. 2003 Mar;134(3):342-6.
4. Rocca MA, Kudryk VL, Pajak JC, Morris T. The evolution of a teledentistry system within the Department of Defense. Proceedings. AMIA Symposium. 1999;921-4.
5. Shirolkar R, Ruparelia KP, More C, Ruparelia P. Teledentistry: an art and science of healing. J Indian Acad Oral Med Radiol. 2011;23(2):108-11.
6. Daniel SJ and Kumar S. Teledentistry: a key component in access to care. J Evid Based Dent Pract. 2014 Jun14; Suppl:201-8.
7. Glassman P, Harrington M, Mertz E, Namakian M. The virtual dental home: implications for policy and strategy. J Calif Dent Assoc. 2012 Oct 22;40(7):605-11.
8. Estai M, Bunt S, Kanagasingam Y, et al. Diagnostic accuracy of teledentistry in the detection of dental caries: a systematic review. J Evid Based Dent Pract. 2016 Sep 7;16(3):161-72.
9. Alabdullah JH and Daniel SJ. A systematic review of the validity of teledentistry. Telemed J E Health. 2018 Jan 5;24(8):639-48.
10. Mandall NA, O'Brian KD, Brady J, et al. Teledentistry for screening new patient orthodontic referrals. Part 1: a randomized controlled trial. Br Dent J. 2005 Nov 26;199(10):659-62.
11. Queyroux A, Saricassapian B, Herzog D, et al. Accuracy of teledentistry for diagnosing dental pathology using direct examination as a gold standard: results of the tel-e-dent study of older adults living in nursing homes. J Am Med Dir Assoc. 2017 Feb 22;18(6):528-32.
12. Kopycka-Kedzierawski DT, McLaren SW, Billings RJ. Advancement of teledentistry at the University of Rochester's Eastman Institute for Oral Health. Health Aff (Millwood) 2018 Dec;37(12):1960-6.
13. Fricton J, Chen H. Using teledentistry to improve access to dental care for the underserved. Dent Clin North Am. 2009 Jul;53(3):537-48.
14. Berndt J, Leone P, King G. Using teledentistry to provide interceptive orthodontic services to disadvantaged children. Am J Orthod Dentofacial Orthop. 2008 Nov;134(5):700-6.
15. Carrard VC, Roxo Gonçalves M, Rodriguez Strey J, et al. Telediagnosis of oral lesions in primary care: the EstomatoNet Program. Oral Dis. 2018 June 7;24(6):1012-9.
16. Estai M, Kanagasingam Y, Tennant M, Bunt S. A systematic review of the research evidence for the benefits of teledentistry. J Telemed Telecare. 2018 Apr;24(3):147-56.
17. United States Census Bureau. QuickFacts North Carolina population estimates, July 1, 2019. [Internet]. Suitland: U.S. Department of Commerce. 2020 [cited 2020 June 4]. Available from: https://www.census.gov/quickfacts/NC
18. Kaiser Family Foundation; Dental care health professional shortage areas (HPSAs) as of September 30, 2019 [Internet]. Washington, DC: Kaiser Family Foundation; c2020 [cited 2020 June 4]. Available from: https://www.kff.org/state-category/providers-service-use/
19. Barnett ML, Ray KN, Souza J, Mehrotra A. Trends in telemedicine use in a large commercially insured population, 2005-2017. JAMA 2018 Nov 27; 320(20):2147-9.
20. UNC Medical Center. 24/7 Virtual Urgent Care [Internet]. Chapel Hill: UNC Health Care; c2020. [cited 2020 June 4]. Available from https://www.uncmedicalcenter.org/uncmc/care-treatment/urgent-care/24-7-virtual-urgent-care/
21. University of the Pacific. Virtual dental home system of care [Internet]. San Francisco: Arthur A. Dugoni School of Dentistry; c2020 [cited 2020 June 4] Available from: https://dental.pacific.edu/departments-and-groups/pacific-center-for-special-care/innovations-center/virtual-dental-home-system-of-care
22. Oral Health Workforce Research Center. Variation in dental hygiene scope of practice by state [Internet]. Albany: SUNY School of Public Health; c2015. [updated 2019 January; cited 2020 June 4] Available from: http://www.oralhealthworkforce.org/resources/variation-in-dental-hygiene-scope-of-practice-by-state/
23. Glassman P, Harrington M, Mertz E, Namakian M. The virtual dental home: implications for policy and strategy. J Calif Dent Assoc. 2012 Jul 40(7):605-11.
24. Daniel S, Wu L, Kumar S. Teledentistry: a systematic review of clinical outcomes, utilization and costs. J Dent Hyg. 2013 Dec;87:345-52.
25. Daniel SJ, Kumar S. Comparison of dental hygienists and dentists: clinical and teledentistry identification of dental caries in children. Int J Dent Hyg. 2017 Nov;15(4):e143-e148.
26. Estai M, Kruger E, Tennant M. Perceptions of Australian dental practitioners about using telemedicine in dental practice. Br Dent J. 2016 Jan 15; 220(1)25-9.
27. Scott Kruse C, Karem P, Shifflett K, et al. Evaluating barriers to adopting telemedicine worldwide: a systematic review. J Telemed Telecare. 2018 Jan;24(1):4-12.