You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Fundamental skills necessary for clinical treatment must be acquired during the undergraduate or vocational levels of dental hygiene education. Sufficient education for students to reach a successful level of competency is necessary. Computer-assisted learning (CAL) in dental or dental hygiene education has been proven valuable, favorable, and beneficial when used alongside live patient interactions or lecture curricula.1-6 The use of CAL is increasing in dental education,1,7 and CAL could be an effective teaching strategy for subject areas in which few cases are available for clinical instruction or in areas where insufficient contact hours are reported in dental education.8
Educators and clinicians have been developing interactive simulation modules using an original authoring tool (SIMTOOL) developed at the Tokyo Medical and Dental University (TMDU; Tokyo, Japan) since 2003,8-15 and over 100 dental simulation learning modules have been published.16-18 The use of CAL has recently been investigated on domestic and international levels, and the feedback for the modules and CAL has been shown to be positive (data unpublished).
Computer-assisted learning simulation training modules for dental hygienists and dental hygiene students using SIMTOOL has been developed to provide learning opportunities in subject areas where case availability is limited since 2005.11,12 Additional focus areas include situations where clinical education reflecting the current knowledge and trends is required but the number of educators and/or lecture/clinical contact hours are limited.11,12 In response to this need, a new series has been created to assist dental hygienists and dental hygiene students in acquiring clinical decision-making and communication skills in the English language in preparation for future clinical settings.10 Proficiency in English will become essential for healthcare professionals to be able to communicate with an increasing number of international patients. Communication skill acquisition in both Japanese and English is an important issue in dental hygiene education in Japan,8-10,19 yet the materials, training hours, and educators remain limited. This English-language communication series has gained positive evaluation from learners in regard to content and system operation10; however, the learning outcomes and overall usefulness of the content have not been investigated. The purpose of this study was to evaluate the learning outcomes and practicality of interactive basic English conversation simulation modules developed for a Computer Learning System (CLS) in dental hygiene education.
Methods
Study population
This study was approved by the Dental Research Ethics Committee of Tokyo Medical and Dental University (TMDU; approval no. 968; Tokyo, Japan). During a five-week period (April 4 - May 9, 2016), all 29 fourth-year undergraduate dental hygiene students from the School of Oral Health Care Sciences at TMDU were given access to five interactive modules (Basic English Conversation Practice for Dental Hygienists) for self-learning via an LMS (WebClass; Data Pacific [Japan] Ltd., Tokyo, Japan). Students were familiar with the function of e-learning modules from previous LMS experiences.
Assessment tools
Baseline English language communication skills were assessed with a pre-test on the first day the learning modules became available (April 4, 2016). A post-test was administered on May 9, 2016, at the conclusion of the five-week study period. The pre- and post-tests consisted of 10 multiple-choice listening-type questions (10 points per question). Questions were based on a case study of an English-speaking patient who called to make an appointment, and subsequently presented to the clinic to learn how to brush and floss. The degree of difficulty between pre- and post-tests was consistent, and both tests covered the same situation. Post-test items were rewritten and re-recorded with slight differences to decrease the possibility of increased score due to memorization.
A questionnaire was also distributed via the LMS at the conclusion of the study period to assess the learners' self-perception of their field of study knowledge, the materials' influence on their learning and their usefulness outside of the classroom, the learners' eagerness and interest in the content, and ease of operation for CAL. Responses to questions (Q1-Q8) were on a four-point Likert scale and the opportunity to provide open-ended comments was provided on Q9. Informed consent was given via the LMS prior to beginning the questionnaire.
Interactive modules and e-learning system
Five educators who were either native Japanese or English speakers, with backgrounds in periodontology, operative dentistry, dental hygiene, dental education, or nursing science, authored the interactive modules using SIMTOOL and Microsoft Moviemaker 2.6 (Microsoft; Redmond, WA, USA). SIMTOOL requires no computer-programming knowledge, making it easy for clinicians or educators to develop interactive learning modules without any Internet technology expertise. Quality of the learning modules was assured in two stages: first, by members of the Educational Simulation Production Subcommittee, consisting of healthcare professionals representing most dental specialties, established under the TMDU Dental Educational Committee; and, second, by two reviewers, based on content, interactivity, online user-friendliness, and efficacy of multimedia usage in the scenario.
The interactive modules provided learners a self-paced, independent learning opportunity to practice with cases covering telephone requests for regular and emergency treatment appointments (modules 1-3), tooth brushing (module 4) and flossing instruction (module 5). The modules provided virtual clinical settings or experiences to take learners through decision-making processes for making appointments and for explaining procedures and treatments by having them choose the correct answer from multiple-choice questions in English. An example of the learner's view is shown in Figure 1. Instructors were able to insert situations or other information in audio/visual format into the three windows on the upper half of the screen. Photos or video clips from actual clinical scenes, X-rays, explanatory notes, dental formulae, and/or recorded voices/sounds could be uploaded to these windows. Each window could also be enlarged by selecting an icon at the bottom right corner. Learners could listen to conversations or sounds related to the situation by clicking the "play" button at the bottom left corner of the window. Instructions and multiple-choice questions could be found on the lower half of the screen. To assist learners in practicing listening skills on simulated real-life situations, the multiple-choice answers for the conversations were not displayed. Once the learners selected and confirmed their choice, the next page would display their answer and explanatory notes as to the appropriateness of that choice (Figure 1). All multiple-choice answers and explanatory notes were shown in this area. It was possible for learners to review all questions, and correct answers with explanations after completing the module (Figure 2). The authors were able to assign a score for each question, based on the difficulty level, with a maximum score of 100 for each module.
Utilization of modules
Students' self-study times were recorded via the LMS; data included their access period, access number, and score for each material. Based on this data, participants were classified into two groups (study group and non-study group), based on their use/non-use of the modules within the five-week access period. Inclusion criteria for the study group was that they accessed all modules for more than one minute each; the remaining students were categorized into the non-study group.
Statistical analysis
The pre- and post-examination scores and the differences in score for each student were analyzed by the Mann-Whitney U test and the Wilcoxon signed-rank test, respectively, using SPSS Statistics for Windows, Version 23.0 (IBM Corp.; Armonk, NY). In the study group, the number of self-study access times for each module, between participants whose scores increased and participants whose scores either remained the same or decreased, were analyzed based on the Mann-Whitney U test.
Results
Questionnaire
Twenty-nine students used the modules and all 29 answered the post-questionnaire for a response rate of 100% (Figure 3). Of the respondents, 97% agreed/somewhat agreed that they learned a lot from the modules (Q2), 93% considered that the module content would be useful/somewhat useful for them in the future (Q3), and 52% responded they had the level of professional knowledge contained in the modules (Q1). Ninety percent of respondents answered favorably to continuing learning with the modules (Q6), 79% of respondents expressed a desire to continue learning with more simulation modules (Q5), and 86% of respondents expressed a desire to take a class on the content covered in the modules (Q4). Respondents' general comments are shown in Table I.
Pre- and post-test results
A total of 28 of the 29 students took the post-test. Out of a possible score of 100 points, the average pre-test score was 45 points with a median of 40 points and the average post-test score was 66 points with a median of 75 points. The study group (n = 22), participants who accessed all of the modules over the five-week period, had an average score of 48 points and a median of 40 points on the pre-test, whereas the post-test average score was 71 points with a median score of 80 points.
The non-study group (n = 6), participants who chose not to use the modules, had an average pre-test score of 33 points and a median score of 40 points, and the post-test average and median scores were 47 points and 35 points, respectively.
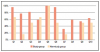
Post-test questions 7 and 8 had a low percentage of correct answers for both the study and non-study groups (29% and 46%, respectively); question 9 had 54% correct responses. The remaining questions had more than 60% correct answers, regardless of the group (Figure 4).
The post-test scores were significantly higher for participants who utilized the modules to study, compared to participants who did not (p = 0.024). Participants in the study group scored significantly higher on the post-test than they scored in the pre-test (p = 0.001). There were no significant differences between the post- and pre-test scores for the non-study group.
There were no significant differences in the study group on the number of times each module was accessed between those participants whose scores increased (n=18) and participants whose scores remained the same or decreased (n=4), based on the Mann-Whitney U test (p = 0.03, p = 0.5, p = 0.185, p = 0.823, and p = 0.65 for modules 1-5, respectively).
Discussion
In this study, it was found that undergraduate dental hygiene students considered the modules developed with SIMTOOL and made available via the LMS for self-study were beneficial for acquiring skills and knowledge. The questionnaire results revealed that the learners considered the interactive modules, as well as the operating system, to be convenient and beneficial, findings in accordance with previous studies.8-13 However, in previous studies, learning outcomes were not investigated.
Participants who studied the materials presented in the simulation module over the course of the five-week study period had significant score increases, which seems to demonstrate the value of self-study with e-learning modules (p = 0.001). On the other hand, there were no significant differences in learning outcomes for those participants who did not utilize the modules. This finding indicates that CAL simulation learning has a positive impact on improving the necessary skills for dental hygienists in a clinical setting.
The lack of change in the scores for participants who did not utilize the study modules negated the possibility that the pre-test activity itself could be considered practice and improved the students' skills. The pre- and post-tests had been re-written and re-recorded, to cover the same clinical situations with slight differences while maintaining the same level of difficulty in anticipation of the possible effect of the test activity alone influencing the outcome. In addition, the test results suggest that the learners are not able to maintain their skills or knowledge for more than 6 months, as these simulation modules were made available to five of the 28 students one year earlier (August 2015). Following that session, no access was recorded until the beginning of the current study. Even with the prior exposure to the modules, no significant differences in the pre-test scores were demonstrated between participants with previous experience (Mann-Whitney U test; p > 0.05). This finding indicates that previous experience without continuous use had no effect on test scores. This short-term outcome may be derived from the study style and the subject itself. Students did not have many opportunities to study dental English at the university level and have stopped studying the language before acquiring competence. Some reports indicate that dental hygiene students in Japan consider English as difficult to learn.20 While 98% of the participants who responded that they considered the ability to communicate in English as important for dental hygienists, English has been noted as a problem or concern in slowing down international exchanges.21 This factor was one reason behind the development of this series of modules.
The low percentage of correct answers to pre- and post-test questions 7 and 8 also reflected participant's difficulty in understanding English. For these questions, participants had to distinguish between English pronunciations that sounded the same as if they were printed in Japanese kana characters and included the usage or choice of verbs that are always difficult for non-native speakers.
English is indispensable for healthcare professionals and is the most frequently used language in the clinical setting when the patients' native language differs from that of the dental hygienist. However, English language education for healthcare workers in Japan is still in the improvement stage,19,21-23 making communication skill acquisition in English an urgent challenge.8,19 Therefore, aspects of English as a second language (ESL) should be included in CAL simulation modules. In addition to emphasizing proficiency in various aspects of English, this series also emphasized the clinical decision-making process. The modules had components requiring clinical knowledge, experience, and decision-making skills (e.g. tooth brushing instruction) similar to other clinical simulation modules, with the added bonus of learning the instructions in English.
Virtual patient simulations have been designed for the acquisition or promotion of critical reasoning skills as a part of the development of treatment competencies when the number of live patient encounters is insufficient.24 The use of patient simulation is especially beneficial in fields that require many hours of study or that have manpower shortages, which can occur in dental hygiene education. Decision-making skills in English for dental professionals is a good example where self-study with computer-assisted simulation modules might be a solution strategy.8
Communication skills are very important for the dental hygiene profession; especially for professionals employed in hospitals or clinics with a high number of international patients. The nature of dental hygienists' responsibilities may require them to use a wider range of communication skills, as compared to other dental professionals. Therefore, acquiring communication skills in English is indispensable. However, opportunities for acquiring these skills are limited in Japan and the logistics of providing them is problematic for many educational institutions.21 Additional advantages of CAL simulation modules includes instant feedback and the ability for students to study independently on their own schedule from wherever they have a computer and Internet access. The learning modules used in this study conform to the Sharable Content Object Reference Model (SCORM) 1.2 standards; thus, they can be directly incorporated into the LMS of any commercially available e-learning platform at any educational institution.
Acquiring the level of technical knowledge and dental English necessary for use in a clinical setting takes ongoing practice. Before reaching that level, maintaining the skill and knowledge may be difficult without any supporting tools or study opportunities. Further research is needed to investigate learning outcomes in actual clinical settings after a designated period of use of simulated instruction. Limitations of this study include its small cohort. Future studies should use a larger cohort and collaborate with other universities over a longer period of time. In addition, the pre- post-test focused on evaluating the acquired knowledge; another examination method should be included for skill and attitude acquisition.
Conclusion
Competence in fundamental clinical skills must be acquired during undergraduate dental hygiene education. CAL simulation modules can be designed into the curricula to assist students in acquiring specific skills that are a part of their competencies. Modules made available through an LMS were shown to be beneficial for Japanese undergraduate dental hygiene students in the acquisition of knowledge and skills for clinical decision-making in the English language.
About the Authors
Naoko Seki, DDS, PhD is an assistant professor, Institute of Global Affairs, Tokyo Medical and Dental University and Department of Dental Education Development, Graduate School of Medical and Dental Sciences, Tokyo, Japan.
Janelle Moross is a senior associate professor, Institute of Global Affairs, Tokyo Medical and Dental University and Institute of Education, Tokyo Medical and Dental University, Tokyo, Japan.
Hiromi Otsuka is an adjunct lecturer, Department of Preventive Oral Health Care Science, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Masayo Sunaga, RDH, BLA is an assistant professor, Institute of Education, Tokyo Medical and Dental University, and Department of Educational Media Development, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Mio Naito is a graduate student, Department of Dental Education Development, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Keiko Kondo is a senior associate professor, Department of Lifetime Oral Health Care Science, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Kayoko Shinada, DDS, PhD is a professor, Department of Preventive Oral Health Care Science, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Ikuko Morio, DDS, PhD is a professor, Institute of Global Affairs, Tokyo Medical and Dental University and Department of Dental Education Development, Graduate School of Medical and Dental Sciences, Tokyo, Japan.
Atsuhiro Kinoshita, DDS, PhD is a professor, Institute of Education, Tokyo Medical and Dental University and Department of Educational Media Development, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Corresponding author: Atsuhiro Kinoshita, DDS, PhD; kinoshita.emdv@tmd.ac.jp
References
1. Cederberg RA, Bentley DA, Halpin R, et al. Use of virtual patients in dental education: a survey of U.S. and Canadian dental schools. J Dent Educ. 2012 Oct;76(10):1358-64.
2. McCann AL, Schneiderman ED, Hinton RJ. E-teaching and learning preferences of dental and dental hygiene students. J Dent Educ. 2010 Jan;74(1):65-78.
3. Brearley ML, Kan K, Cameron A, et al. Teaching paediatric dentistry by multimedia: a three-year report. Eur J Dent Educ. 2002 Aug;6(3):128-38.
4. Boynton JR, Green TG, Johnson LA, et al. The virtual child: evaluation of an internet-based pediatric behavior management simulation. J Dent Educ. 2007 Sep;71(9):1187-93.
5. Schittek M, Mattheos N, Lyon HC, et al. Computer assisted learning. A review. Eur J Dent Educ. 2001 Aug;5(3):93-100.
6. Rosenberg H, Sander M, Posluns J. The effectiveness of computer-aided learning in teaching orthodontics: a review of the literature. Am J Orthod Dentofacial Orthop. 2005 May;127(5): 599-605.
7. Hillenburg KL, Cederberg RA, Gray SA, et al. E-learning and the future of dental education: opinions of administrators and information technology specialists. Eur J Dent Educ. 2006 Aug;10(3): 169-77.
8. Seki, N, Moross J, Sunaga M, et al. Evaluation of simulation learning materials use to fill the gap in Japanese dental English education. J Med Dent Sci. 2016 Mar;63(1): 1-8.
9. Seki, N, Moross J, Sunaga M, et al. Development of new interactive materials for medical interviews in English [in Japanese]. JJDEA. 2014 Dec;30:170-5.
10. Seki, N, Moross J, Sunaga M, et al. Development of ESL clinical simulation teaching materials for dental hygienist education [in Japanese and English]. Poster presented at: The Annual Meeting of the 35th Japanese Dental Education Association; 2016 Jul 2; Osaka, Japan.
11. Yoshida N, Aso T, Asaga T, et al. Introduction and evaluation of computer-assisted education in an undergraduate dental hygiene course. Int J Dent Hyg. 2012 Feb;10(1):61-6.
12. Yoshida H, Sunaga M, Yoshida N, et al. Development and evaluation of a new computer assisted education software for dental hygienist students to practice the subgingival scaling and root planning [in Japanese]. JJSDH. 2009 Aug;4:58-63.
13. Kubota T, Cho Y, Kajiwara M, et al. The use of a computer-assisted simulation system in undergraduate education of laboratory technologists [in Japanese]. Jpn J Clin Pathol. 2007 Jun;55:517-21.
14. Ohyama A, Yoshioka T, Kohase H, et al. Implementation and assessment of faculty development for making simulation teaching materials [in Japanese]. JJDEA. 2008 Apr;24:88-101.
15. Ohyama A, Shimizu C, Satou M, et al. Implementation and assessment of simulation education system in medicine and dentistry, at the clinic of general dentistry and oral diagnosis in our dental hospital [in Japanese]. Jpn J Oral Diag/Oral Med. 2009 Mar; 22:1-10.
16. Kinoshita A, Kawakatsu N, Nagasawa T, et al. TMDU clinical training series for dentists 2nd ed (2015) [in Japanese][e-learning system/cloud distribution], Tokyo, Japan: University of Tokyo Press; 2012 Dec (1st ed). 93 e-learning scenarios.
17. Seki N, Sunaga M, Fukui Y, et al. TMDU clinical training series for ESL dentists on medical interviews [in Japanese] [e-learning system/cloud distribution], Tokyo, Japan: University of Tokyo Press; 2014 Aug. 10 e-learning scenarios.
18. Takemawari Y, Miura Y, Sagawa K, et al. TMDU clinical training series for dental hygienists on MFT [in Japanese] [e-learning system/cloud distribution], Tokyo, Japan: University of Tokyo Press; 2014 Aug. 22 e-learning scenarios.
19. Morros J, Seki N, Morio I. English education for healthcare professionals in Japan. Jpn Dent Sci Rev. 2017 Nov;53(4):111-6.
20. Fukuda M, Yamasaki M. Effects of active learning in English classrooms based on questionnaires. JJSDHE 2016 Oct;7:129-36.
21. Takenouchi A, Sakurai/Matsukubo M, Matsukubo T. Interest in international programmes-a survey of Japanese dental hygiene students and educators. Int J Dent Hyg. 2017 Nov;15: e93-9.
22. Morse Z, Nakahara S. English language education in Japanese dental schools. Eur J Dent Educ. 2001 Nov; 5:168-72.
23. Rodis OM, Matsumura S, Kariya N, et al. Undergraduate dental English education in Japanese dental schools. J Dent Educ. 2013 May;77(5):656-63.
24. Cook DA, Triola MM. Virtual patients: a critical literature review and proposed next steps. Med Educ. 2009 Apr;43(4):303-11.