You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Teaching methods in higher education have traditionally been delivered through a mass lecture format, limiting the opportunities for interpersonal communication between faculty and students.1 The quality and quantity of communication between students and faculty in higher education has been associated with student success and retention in dental hygiene programs.2 Interactions and communications among faculty and students can increase student motivation, engagement, satisfaction in academic and non-academic life, student persistence in academic pursuit, and in the facilitation of teacher immediacy and trust.3
Traditionally, student-faculty communication has been face-to-face during office hours or via the telephone. However, the introduction of the Internet and other technological advances has increased the options of communication tools, including social media which is popular among the digital natives and millennial students.4 Social media (SM) is defined as "a communication medium that is devoted to or characterized by interaction between participants or consumers of the medium."4
Optimal teaching and learning is dependent upon effective communication between the teacher and student. Dobransky and Frymier found that students who participated in out-of-class communication (OCC) with faculty during a course reported higher levels of cognitive learning and a more favorable perception of overall learning.5 Conventional faculty office hours have not been fully utilized by students, and an increasing number of students are requesting more options
for OCC with faculty. Evidence in the differences between perceived expectations and comfort levels of educators and students concerning use of SM in higher education has been
found in the literature.4 This difference in comfort and use of SM between students and faculty has been labeled the social media-based communication gap.4 As technology continues to advance, more options for OCC tools using social media have emerged.
Roblyer et al. concluded that faculty use SM primarily for personal reasons, and found that only 15% of faculty reported using SM to communicate with students and nearly one-third of the faculty expressed uncertainty about SM applications being useful for educational purposes.6 In another study assessing dental school faculty members' use and preference of SM applications, Arnett et al. concluded that SM sites were both underdeveloped and underestimated in terms of their potential educational value to the profession.7 Use of SM use may enrich learning in dental education by illustrating curricula by offering students additional mechanisms to collaborate with faculty and fellow students; enhancing the quality of homework; increasing the retention and application of knowledge and skills; instilling the value of active participation and self-directed learning; and providing a platform for more frequent interdisciplinary collaboration and the development of communities of learners.7
DiVall and Kirwin's findings from a mixed observation and qualitative study of pharmacy students corroborated the results of Roblyer et al. regarding students' perceptions of SM as an OCC tool.6,8 The pharmacy course utilized a learning management website and a class specific Facebook page. Identical information was available on the learning management site and the Facebook page and student preferences were evaluated. Observational results showed that students were more likely to be exposed to course content through the Facebook page than the learning management website and a post-course survey indicated that 86% of the students found the course Facebook page to be beneficial.8 Similarly, undergraduate business students in another study indicated that the course Facebook group page stimulated them to acquire resources from teachers and other classmates, ask for solutions to assignments, and/or provide comments to other students and to the instructor. Perceived ease of use was cited as the critical factor influencing student acceptance of the course Facebook page.9
A systematic review of the benefits and challenges of SM use in medical education identified student engagement as one of the main benefits of SM use.10 Increased opportunity for feedback, increased communication from peers and faculty to students, enhanced collaboration, professional development, career networking and advancement, and resource sharing were also identified as benefits. Technical issues and varying levels of student participation were challenges of SM use in educational settings along with privacy concerns, policy restrictions, and time requirements from both the student perception and faculty perception.10
Beebe et al. found that a variety of technologies are being incorporated into dental hygiene programs to supplement educational strategies.11 Both faculty and students reported increased access to learning resources as an advantage, while faculty also reported increased student engagement.11 Students reported that technology facilitated communication with instructors and classmates.11 Barriers due to technical difficulties identified in the systematic review10 were also reported by nearly three quarters of both the faculty and students.11
Some dental hygiene programs have established policies prohibiting SM communication between faculty and students.12 Among the dental hygiene directors queried by Henry and Pieren regarding whether their programs' code of conduct policy specifically addressed SM, nearly all (96%) programs had a code of conduct policy, however only 36% specifically mentioned SM.12 Of those indicating that SM was not currently included in their code of conduct policy, over half (55%) stated they were considering adding SM to the policy.12 Determining SM trends and patterns by faculty and students for OCC may influence and guide SM policy formation in dental hygiene programs.
The Uses and Gratification Theory (UGT) and the Technology Acceptance Model (TAM) as they relate to SM use for OCC provides a theoretical framework for understanding SM use for OCC. The UGT supports the use of technology as a means for OCC research by examining the "how and why" individuals select and use specific media to satisfy their communication needs. The UGT defines the role of the individual as one who actively seeks, selects and uses media in order to achieve gratification by accomplishing a goal or fulfilling a need. When expectations are met or exceeded, recurrent use of the media leads to habitual use.13 Quan-Haase and Young applied the UGT to new media options introduced by developing technology.13 The ongoing relevance of the UGT persists as technology advances and increases the options for media use in educational programs, by exploring the motives behind why individuals will choose and use specific media.
Similar to the U&G theory, the Technology Acceptance Model (TAM) presents two important factors that influence how technology is accepted and used.9 First, the technology must be perceived as useful. The perceived usefulness refers to the expected positive benefits of technology use as the determining factor of the intention to use, and has been positively associated with adoption of SM in an educational setting.9,14-15 Arrigoni et al. stated that when choosing communication tools, it is important to consider the usability of the communication tools and their potential and purpose.16 Second, technology must be perceived as easy to use. The ease of use factor is a strong predictor determining the acceptance of technology, especially in the early adoption phase.9 The TAM presents two factors that support the "how and why" of media and technology of the UGT. Using the TAM and the UGT, a deeper evaluation of student and faculty perceptions concerning SM use as an OCC tool can be evaluated.
The purpose of this pilot study was to determine if entry-level dental hygiene students and dental hygiene faculty perceive using SM applications as an OCC tool can enhance learning in a dental hygiene program.
Methods
This cross-sectional, comparative research study evaluated entry-level dental hygiene students' and dental hygiene faculty members' social media utilization and preferences for OCC to enhance learning. Variables tested included: learning, entry-level dental hygiene students, dental hygiene faculty, social media applications, and electronic devices.
An investigator-designed survey was constructed based on the literature to evaluate the hypotheses. A report by comScore cited the most popular SM applications by adults, including digital natives or millennial students (individuals born between 1980-2001, aged 18-24 years)17 which represents average entry-level dental hygiene students. For the purpose of this study, the top four SM applications that were both collaborative and facilitate communication between two parties were selected for this questionnaire included Facebook, Facebook Messenger, Twitter and SnapChat. Learning management systems (LMS) were also included in the questionnaire as educational institutions have used LMS to facilitate communication and enhance learning between faculty and students. In addition, the types of electronic devices used to access SM applications for OCC were also studied. The Pew Research Center studied the types of devices that affect how adults interact and communicate with each other and spend their time, and identified the cellular or smartphone as the most popular device.18 Desktop, laptop, and tablet computers were additional devices owned by adults that facilitate communication through SM applications.18 Considering this information, the survey included items related to electronic device type (smartphone, desktop computer, laptop computer, and tablet). Abbreviations SM and OCC were written out fully on the survey.
Validity, using a Content Validity Index,19 was tested by five dental hygiene educators, who were not participating in the study and all items were rated as being either relevant or very relevant. The survey was also evaluated for reliability by another cohort of dental hygiene experts using the test/retest procedure. The research protocol was deemed exempt by the Human Subjects Research Committee at Idaho State University (IRB -FY2017-227).
A convenience sample of dental hygiene students and faculty from nine entry-level dental hygiene programs in Utah, Idaho, California, Washington, and Oregon were invited to participate. The dental hygiene programs were located in community colleges offering associate degrees and in four-year university settings offering either associate or baccalaureate degrees.
Students were required to be enrolled in a dental hygiene program as either a first- or second-year student at the time the survey was completed to be eligible to participate. Students who had graduated, were enrolled in a degree completion or a graduate program, or were expecting to enroll in a dental hygiene program at a future date were not eligible to participate. Eligibility requirements for dental hygiene faculty included being employed as full time, part-time, or adjunct and teaching a didactic course or in the clinic setting with a license as a Registered Dental Hygienist (RDH), Doctor of Dental Surgery (DDS), or Doctor of Medicine in Dentistry (DMD).
Paper surveys were mailed to a designated survey administrator at each participating dental hygiene program. The survey administrator distributed the survey to eligible, dental hygiene students and faculty according to written instructions to ensure uniformity in administration at each participating site. The survey packet included a cover letter, an informed consent statement, and questionnaires. After participants completed the survey, the completed questionnaires were mailed back to the principal investigator in a return postage-paid envelope. Data was entered manually into SPSS Statistics 24 software (IBM; Armonk, NY) . Descriptive and inferential statistics were utilized for data analysis, significance was established at p=0.05.
Results
A total of 418 students and 149 faculty members met the eligibility criteria; 325 students (n=325) and 77 faculty completed the surveys (n=77) for a combined response rate of 70.9%.
The majority of students and faculty were female; most students were younger than 34 years of age while most faculty were older than 41years of age. A majority of the faculty (62%) had been teaching for less than 10 years and most were registered dental hygienists. Table I provides a summary of demographic data for both students and faculty.
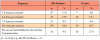
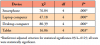
Respondents were asked how learning was enhanced by using SM for OCC. Most students and faculty were similar in their viewpoints on how SM enhanced learning. One exception was under the question "facilitates acquisition of new knowledge." For this item, a higher proportion (55.8%) of faculty members selected this option as compared to students (35.7%), which was statistically significant (p= .001, Table II). Students and faculty were asked to rate how comfortable they were using SM as an OCC tool. Four hundred participants responded to this survey item (Table III). Pearson Chi Square was used to determine significant difference in the comfort level of entry-level DH students and faculty using SM as an OCC tool and the results were not statistically significant (p =.36).
Respondents were given options to choose how SM was currently being used for OCC. Both faculty and DH students selected "questions about assignments," "clarification on lecture topics," and "feedback on assignments" as their top three choices for this survey item (Table IV). Pearson Chi Square results were statistically significant for "questions about tests," "questions about assignments," and "I do not use SM" (p =.001). While more DH students use SM for questions about tests and assignments than faculty, more faculty noted that they did not use SM for OCC with students.
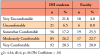
Respondents were asked to identify their frequency of use of SM applications for OCC (Table V). Most students and faculty indicated they use SM 10 or more times per semester. Pearson Chi Square showed these responses were statistically significant (X2 =16.92; df =4; p =.002). Cramer's phi coefficient was .21 representing a small effect size. The locus of the difference appears to be the percentage of the "do not use" responses and the percentage of the "10+ times per semester" responses between students and faculty.
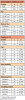
Dental hygiene students and faculty were asked to rank the SM applications they use for OCC. Learning management systems was used most frequently by both groups (n=223, 71.5% for students; n=51, 68.9% for faculty) followed by Facebook (n=68, 22.1% for students; n=11, 15.5% for faculty). Twitter, SnapChat, and Facebook Messenger were least used in comparison (data not shown). Findings were statistically significant between all groups at the p<.001 level
with the exception of the Twitter group as shown in Table VI. The major difference indicated the faculty members did not use any of these SM applications in comparison to the students.
Respondents were asked to rank the SM applications they prefer to use for OCC. Results were similar between faculty and DH students (Table VI). Learning management systems were preferred most often by DH students ( n=221, 70.6%) and faculty (n=54, 74.0%) followed by Facebook (DH students n=64, 20.6%; faculty n=9,13.2%). All other categories were "do not prefer" for faculty except for the "learning management system." Statistical significance was found between SnapChat and LMS most likely due to the large difference in the number of students who do not prefer SnapChat compared to faculty, and due to the number of faculty preferring LMS as compared to faculty who do not prefer it at all.
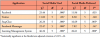
Dental hygiene students and faculty ranked the electronic devices used most frequently for OCC (Table VII). DH students ranked the smartphone as their first choice (n=181, 58.6%) while the laptop was a second choice for electronic device use (n=146, 47.4%). Faculty identified the laptop as their first choice for electronic device use (n=26, 35.6%), and desktop was their second choice (n=24, 32.9%).
Discussion
This study examined dental hygiene students and faculty perceptions whether the utilization of SM applications as an OCC tool would also enhance learning. Results from this study indicated both faculty and DH students see the relevance of SM for increasing course engagement, encouraging active thinking and providing ready access for communication. Faculty participants felt that the use of SM facilitated acquisition of new knowledge and only about five percent of DH students and faculty felt that SM for OCC did not enhance enhanced learning.
These findings support those of Samuels-Peretz et al. who studied faculty and students in six different college-level courses in ten disciplines using SM.20 Their results showed students agreed SM facilitated higher order, integrative, and reflective learning, and the faculty perceptions of learning was highly correlated with those of the students'.20
A majority of students in the Samuels-Peretz et al. study, reported using SM tools in their courses several times per week.20 This finding corresponds with results from this study which showed DH students were using SM applications in their courses ten or more times per semester. One-third of the dental hygiene faculty were using SM applications as part of their courses as frequently as students. However, 27.4% of faculty indicated not using any SM applications at all and nearly 10% only used SM 1-3 times per semester. These results suggest there is a SM communication gap between the faculty and the DH students, or a reflection of clinical dental hygiene faculty survey participants not using SM applications in their teaching role. Esteve del Valle et al. suggested another reason for lack of faculty use of SM applications may be a lack of technology support.21
A majority of DH students in this study indicated being very comfortable or moderately comfortable (54.5%) in using SM for OCC, however the faculty respondents had greater variation in their comfort levels. Open ended comments provided by DH students to explain a "very uncomfortable" (21%) response were incongruent with that selection, indicating that some respondents may have mismarked or misread the comfort scale. Examples of these comments
include "using for a long time," "easily accessible," "faster," "easy to use," "grew up with technology and social media," "continually use it," "love it," "I know how to navigate and
use a computer and Internet," are examples of responses indicating that the respondent may be comfortable using SM as opposed to the "very uncomfortable" choice selected. Dental hygiene students' comfort level and frequency of use identified in this study parallel the "ease of use" and "perceived usefulness" of technology associated with the Technology Acceptance Model.9 The ease of use represents an underlying factor as to why students select SM for OCC, which also corresponds with the Uses and Gratification Theory which explains media choice for needs fulfillment.13
Use of electronic devices for OCC differed between DH students and faculty in this study. Faculty reported using either a laptop or desktop, while DH students used smartphones most often for OCC. One explanation for this difference is that the educational institution might be providing laptop or desktop technology for work-related use, and faculty may prefer to use smartphones for personal use. Dental hygiene student demographics indicate they are a younger cohort and more likely to gravitate toward smartphone technology; a finding supported by a study of nursing students in an undergraduate program.22
Several limitations to this pilot study must be noted. A convenience sample was used of faculty and DH students from dental hygiene programs in the western United States and the results cannot be generalized to the entire population. In addition, the survey was self-designed, however it was generated from the literature and validity was established using a Content Validity Index. An assumption was made that the participants would understand the term social media so it was not defined as part of the directions to the respondents. Some faculty commented they did not believe that a LMS was an example of social media. The literature supports LMS
as a social media application;20, 23 a definition of social media application in the survey directions may have clarified this. However, by including a broad selection of SM applications,
this study exposed a difference in beliefs among DH students and faculty concerning which applications are considered SM. Additional research is needed to explore this difference.
Furthermore, demographic variables were not correlated with the defining variables of the study.
Additional research related to SM and OCC in dental hygiene education is needed. In particular, it is important to examine the impact of university policies on social media and how they influence faculty members' use of SM and ability to use SM for OCC with students. Samuels-Peretz suggests that the integration of SM into college courses can support deeper learning.20 However, if university policies stringently limit the use of SM, faculty may interpret these policies as prohibitive to SM use as a learning tool. Qualitative research could be conducted to further explore faculty perceptions of their expertise and comfort with SM applications, and make comparisons based on generational demographics. Esteve del Valle et al. suggest institutions desiring to encourage future adoption and use of SM in teaching to enhance learning should utilize more experienced instructors for input, and provide technology offerings to further support SM use.21 This study also demonstrated there were differences between faculty and DH students in SM use and preferences. Expanding this study to include a larger and more demographically diverse student population may provide further insight on distinctions between DH students and faculty regarding SM use, experiences, preferences and perspectives to guide future education and training on integrating SM technology into the dental hygiene curriculum.
Conclusion
Social media as an out-of-class communication tool is perceived as contributing to optimal learning and teaching. Dental hygiene students and faculty differ in their frequency and levels of comfort in using SM for out-of-class communication. Additional research related to the phenomenon of social media and communication to enhance learning in dental hygiene should be explored.
Kathren R. Diamond, RDH, MS is an adjunct instructor, Department of Dental Hygiene, Weber State University, Ogden, UT.
JoAnn R. Gurenlian, RDH, MS, PhD is a professor and Graduate Program Director; Jacqueline Freudenthal, RDH, MHE is an associate professor and Department Chair; both in the Department of Dental Hygiene, Idaho State University, Pocatello, ID.
Corresponding author: Kathren R. Diamond;kathrendiamond@weber.edu
References
1. Bowman ND, Akcaoglu M. "I see smart people!" Using Facebook to supplement cognitive and affective learning in the university mass lecture. Internet High Educ. 2014 Oct; 31;23:1-8.
2. Holt MP. Student retention practices in associate degree, entry-level dental hygiene programs. J Dent Hyg. 2005 Jun;79(3):6.
3. Komarraju M, Musulkin S, Bhattacharya G. Role of student-faculty interactions in developing college students' academic self-concept, motivation, and achievement. J Coll Stud Dev. 2010 May/June;51(3):332-42.
4. Kalamas M, Mitchell T, Lester D. Modeling social media use: bridging the communication gap in higher education. J Advert Educ. 2009 May;13(1):44-57.
5. Dobransky ND, Frymier AB. Developing teacher‐student relationships through out of class communication. Commun Q. 2004 Summer;52(3):211-23.
6. Roblyer MD, McDaniel M, Webb M, Herman J, Witty JV. Findings on Facebook in higher education: a comparison of college faculty and student uses and perceptions of social networking sites. Internet High Educ. 2010 Jun;13(3):134-40.
7. Arnett MR, Loewen JM, Romito LM. Use of social media by dental educators. J Dent Educ. 2013 Nov; 77(11):1402-12.
8. DiVall MV, Kirwin JL. Using Facebook to facilitate course-related discussion between students and faculty members. Am J Pharm Educ. 2012;76(2):32.
9. Thongmak M. Factors determining learners' acceptance of Facebook in a higher education classroom. KM & EL. 2014 Sept;6(3):316-31.
10. Cheston CC, Flickinger TE, Chisolm MS. Social media use in medical education: a systematic review. Acad Med. 2013 Jun;88(6):893-901.
11. Beebe CR, Gurenlian JR, Rogo EJ. Educational technology for millennial dental hygiene students: a survey of US dental hygiene programs. J Dent Educ. 2014 Jun;78(6):838-49.
12. Henry RK, Pieren JA. The use of social media in dental hygiene programs: a survey of program directors. J Dent Hyg. 2014 Aug;88(4):243-9.
13. Quan-Haase A, Young AL. Uses and gratifications of social media: A comparison of Facebook and instant messaging. Bull Sci Technol Soc. 2010 Sept;30(5):350-61.
14. Cao Y, Ajjan H, Hong P. Using social media applications for educational outcomes in college teaching: A structural equation analysis. Br J Educ Technol Jun. 2013;44(4):581-93.
15. Sharma SK, Joshi A, Sharma H. A multi-analytical approach to predict the Facebook usage in higher education. Comput Human Behav. 2016 Feb;55:340-53.
16. Arrigoni C, Alvaro R, Vellone E, Vanzetta M. Social media and nurse education: An integrative review of the literature. J Mass Communicat Journalism. 2016 open access;6(1):187-201.
17. The 2016 U.S. Mobile App Report [Internet]. Virginia: comScore; 2016 Sept [cited 2017 Jun]. Available from http://www.comscore.com/Insights/Presentations-and-Whitepapers/2016/The-2016-US-Mobile-App-Report
18. Technology Device Ownership: 2015 [Internet]. Washington, DC: Pew Research Center; 2015 Oct [cited 2017 Jun]. Available from http://www.pewinternet. org/files/2015/10/PI_2015-10-29_device-ownership_FINAL.pdf
19. Sireci S, Faulkner-Bond M. Validity evidence based on test content. Psicothema. 2014;26(1):100-7.
20. Samuels-Peretz D, Dvorkin Camiel L, Teeley K, Banerjee G. Digitally inspired thinking: can social media lead to deep learning in higher education? College Teaching. 2017 Sept;65(1):32-9.
21. Esteve Del Valle M, Gruzd A, Haythornthwaite C, et al. Social Media in educational practice: faculty present and future use of social media in teaching [Internet]. Hawaii In Proceedings of the 50th Hawaii International Conference on System Sciences; 2017 Jan [cited 2017 Jun]. Available from https://scholarspace.manoa.hawaii.edu/bitstream/10125/41169/1/paper0020.pdf
22. Hay B, Carr PJ, Dawe L, Clark-Burg K. "iM ready to learn": undergraduate nursing students knowledge, preferences, and practice of mobile technology and social media. Comput Inform Nurs. 2017 Jan;35(1):8-17.
23. Cartledge P, Miller M, Phillips B. The use of social networking sites in medical education. Med Teach. 2013 Jul;35(10):847-57.