You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Oral health is integral to overall health and wellness. Unfortunately, many children and adults in the United States (U.S.) suffer from poor oral health and a lack of access to oral health care. Nearly twenty years ago, "Oral Health in America: A Report of the Surgeon General" changed the landscape of oral health care by highlighting the profound disparities in oral health across the U.S. and firmly asserting that oral and systemic health are interrelated.1
Oral health disparities and access to care
Children are five times more likely to have dental caries than asthma, and more than half of children aged 5-9 in the U.S. have a carious lesion.1 The prevalence of carious lesions increases with age; by the age of eighteen or older, 84% have had caries or a restoration.1 While dental caries is the most common chronic disease of childhood, low-income children experience a disproportionate incidence and prevalence.1 Dental sealants reduce the risks of carious lesions by up to 80%, yet only one-third of high-risk children have had sealants placed.2 Consequences of dental disparities extend beyond poor oral health; caries and dental disease have been correlated with lower school performance, and psychosocial wellbeing.3 Results from a North Carolina study showed that while a low percentage of absenteeism was due to dental pain or infection, parental reports of poor school performance was higher in children who had experienced dental pain or infection.4
Oral health and access to care are also a significant issue for the adult population. An estimated 90% of adults in the U.S. have a carious lesion and at least 25% have untreated carious lesions.3 In addition, nearly half of adults over the age of 30 have some form of periodontal disease.3 Poor oral health in adults also has wider social implications. A recent study estimated that adults lost 92.4 million hours due to unplanned emergency dental care.5 Younger adults 20-29 years of age are increasingly relying on emergency departments (ED) for toothaches. An estimated 1.27 million ED visits have been for toothaches from this age group, accounting for 42% of all dental pain visits.6 Adults aged 65 and older face even greater oral health disparities. A reported two-thirds of all older adults, and more than 75% of those considered to be low-income, have not had a dental visit in any given year; 20% have untreated caries.7-8 Access to oral health care is needed for people of all ages. Research has shown that providing oral health care to people with chronic illnesses reduces other medical costs, including hospitalizations and emergency room visits.9-10
While advances have been made to improve oral health in both adult and pediatric populations, significant disparities remain, particularly for low income groups. In addition to socioeconomic issues, Healthy People 2020 also identified barriers for all population groups including dental anxiety, cost of care, low health literacy, and limited access to dental providers.11 A variety of oral health care workforce models have been developed as a means to removing these barriers.
Workforce models
Dentists have customarily employed various combinations of allied personnel including dental assistants and dental hygienists within the traditional brick and mortar setting of the private practice/small business. However, decreasing numbers of dentists and factors including geographic location have resulted in areas of low dentist-to-population ratios. Identification of oral health care provider shortage areas has also contributed to the development of alternative workforce models.12 Remote and rural areas have been shown to be more significantly impacted than metropolitan areas as dental providers age out and reach the end of their professional careers.13 As dentists retire from clinical practice however, the number of dental hygienists continues to increase across the U.S.13
Many states have implemented alternative workforce models, some based on well-established models from other industrialized countries, expanding the scope of practice of dental hygienists with the intention of expanding access to care.14 The expanded function dental auxiliary (EFDA) has been shown to be an effective workforce model; general practices utilizing EFDAs have been shown to be more productive and efficient, treat more patients, and have higher gross billings and net income.15 Currently, fifteen states allow expanded functions in some form, with the majority under the direct supervision of a dentist16 and sixteen states allow EFDAs to place and finish amalgam and/or composite resin restorations following the dentist's preparation.16
Access challenges
According to the Maine Department of Health and Human Services Department, the top five contributors to poor health are poverty, lack of access to behavioral and mental health services, transportation, health insurance and employment.17 Nearly one quarter of the population depends on the state sponsored Medicaid program;17 including two-thirds of infants, 40% of children, and nearly 67% of nursing home residents.18 However, very limited dental coverage is available, particularly for those over the age of 21. Lack of dental coverage is compounded by the low number of Medicaid providers, creating significant barriers to care. Furthermore, the dentist to population ratio in rural areas of the state is lower than the national average, with the majority of the state's sixteen counties designated as oral health care provider shortage areas.19 Despite these limitations, state agencies report that advancements have been made towards improving oral health care, particularly by providing access to care through dental and dental hygiene education programs.20 Typically, dental schools and allied dental health education programs act as safety nets, by providing low cost services and community outreach programs. Maine is one of 36 states offering safety nets through dental and allied health education programs.21 However, the two academic institutions in Maine are located in the areas with a high dentist-to-population ratio and geographic barriers remain a significant concern.
Legislative measures
Legislation has been passed in recent years in Maine to allow for a variety of alternative workforce models, including EFDAs, to reduce oral health disparities. Individuals interested in becoming an EFDA must be either a licensed dental hygienist or a dental assistant certified by the Dental Assisting National Board and must complete a board of dental practice approved EFDA education program to be eligible for licensure. EFDA duties include placing and contouring of amalgam and composite restorations, fabricating and removing temporary crowns and bridges, applying pit and fissure sealants and topical fluorides, applying cavity liners and bases, bonding orthodontic bands and brackets, and supra gingival polishing.22 However, these EFDA duties must be performed under the direct supervision of the dentist. In contrast, direct access is defined as the ability to initiate treatment based on assessment of the patient's needs without the specific authorization or physical presence of a dentist.23
Limitations on direct access to care can significantly limit the effectiveness of the EFDA and other alternative workforce models. There is a gap in the literature regarding the effectiveness of the EFDA workforce model first established in 2011 in Maine. However, legislation was passed in 2014 in Maine establishing the Dental Hygiene Therapist (DHT) midlevel provider model. While the intent of increasing access to oral care mirrors that of the EFDA, the direct supervision requirements for both models is the same. In order to effectively assess patient outcomes related to these new workforce models, it is necessary to first assess the practice patterns, effectiveness and challenges of the existing model.
While assessments at the state level are a critical component to program planning and evaluation, they are seldom executed.1 The purpose of this study was to assess the implementation of the EFDA into dental practices within the state of Maine, analyze the geographic practice patterns of EFDAs and evaluate the attitudes regarding EFDA preparatory and continuing education requirements.
Methods
This survey research project was a collaboration between the University of Michigan School of Dentistry and the University of Maine at Augusta and was given exempt status by the University of Maine at Augusta IRB (HUM00121000).
An investigator created, online survey was designed using QualtricsÒ (Provo, UT). The survey consisted of 19 questions including the EFDA practice demographics, skills performed, population served, and continuing dental education courses related to EFDA skills. The University of Michigan Survey Research Center was consulted prior to the distribution of the survey to validate the content. The survey was pilot tested online by 14 practitioners and faculty members who were not participating in the study. A roster of the Licensed Expanded Function Dental Auxiliaries (EFDA) including names, email addresses, and mailing addresses was purchased from the Maine Board of Dental Practice. Two of the investigators were eliminated from the subject population, resulting in a total of 73 potential respondents. Inclusion criteria were having an active EFDA license in the state of Maine. Recruitment emails were sent to the licensed EFDAs with a link to an electronic survey. In an attempt to increase the response rate, paper surveys were also mailed to all EFDAs. The paper surveys were coded to avoid respondent duplication. A follow-up email was sent to non-respondents after two weeks. An additional, follow-up email was sent two weeks after the first reminder, asking subjects to either complete the electronic survey, or the paper survey.
Results
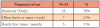
Thirty-eight electronic surveys and five paper surveys were completed for a response rate of 59% (n=43). Nearly three-fourths of the respondents (74%, n=32) had been actively practicing within the previous 12 months, and a majority (67%, n=29) had been practicing as an EFDA between one and five years. Credentials of the respondents varied; a majority of respondents (60%, n= 26) reported holding only the Dental Assisting National Board, Certified Dental Assistant (CDA) credential. The remaining respondents (40%, n=17) were licensed dental hygienists with 10% (n=4) also holding a CDA credential (Table I). Over two-thirds of the respondents (70%, n= 23) reported performing EFDA duties daily, 21% (n=7) of the respondents performed EFDA duties two to four days per week, and 9% (n=3) of the respondents performed EFDA duties only a few times per month, if at all (Table II).
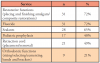
The most frequently reported EFDA duties were restorative services and topical fluoride application (72%, n=31), sealants (65%, n=28), and pediatric prophylaxis (40%, n=17). Regularly provided EFDA functions are shown in Table III.
Only 12% (n=5) of respondents reported practicing in a community/public health setting, while 60% (n=26) practiced in private dental offices (Table IV). Over one- third of the respondents (35%, n=17) reported working in Penobscot County, which is not designated as a dental provider shortage area (Figure 1). In regard to access to care, over one-half (51%, n=22) indicated that their practice did not accept Medicaid. In the county with the highest number of EFDA respondents (Penobscot), one-fourth (25%, n=4) were employed in practices accepting Medicaid. However, over one-half of the respondents 58% indicated feeling that they were making a moderate to significant impact on access to care; individuals working in practices accepting Medicaid felt more strongly regarding their impact on access to care.
A majority (80%, n=34) of respondents reported that less than half of their continuing education courses were relevant to EFDA practice. However, 20% (n=9) indicated that additional topics including dental assistant EFDAs being licensed in local anesthesia and nitrous oxide analgesia, general supervision, and being able to prepare teeth as part of the EFDA preparatory education could increase access to care. Respondents had the opportunity to answer an open-ended question regarding what would make them more effective as an EFDA. Of the respondents (n=23) who opted to respond, 39% (n=9) felt that preparatory education and certification in local anesthesia and nitrous oxide for CDA certified EFDAs would help increase access to care. Of the EFDA respondents suggesting preparatory education and certification in the administration of local anesthesia and nitrous oxide, all of the respondents were credentialed exclusively as CDAs. The administration of local anesthesia and nitrous oxide are already within the scope of practice for Maine dental hygienists who have completed the educational requirements and hold a permit. Educating both dentists and the public regarding the scope of practice for EFDAs was a concern for respondents (22%, n=5).
Discussion
Ever since "Oral Health in America: A Report of the Surgeon General" was published in 2000,1 many individual states have moved forward in creating rules or legislation for a wide variety of workforce models including the EFDA, and dental therapists.24 Currently, there are eleven states that have passed some type of mid-level provider legislation with a least six more pursuing dental therapy legislation.24 While data is continuously being collected on dental therapists and advanced dental therapists licensed in Minnesota, little to no assessment has been conducted on the effectiveness of other workforce models, particularly the EFDA. The lack of needs assessment and program evaluation was a key finding of the Surgeon General's report from 20001 and is particularly evident in Maine, where workforce models including independent practice dental hygienists, public health supervision dental hygienists, and EFDA practitioners were created. These existing workforce models have not been assessed for their impact, however, Maine moved forward and enacted legislation for dental hygiene therapy in 2014.
It is important to know how workforce models such as EFDA are being integrated into practice, and the geographic practice patterns. This information can assist states, safety net providers, and other stakeholders to better advocate for, and strategically implement midlevel providers such dental therapists to effectively address access to care issues. The state of Maine has 15 out of 16 counties designated as dental health care provider shortage areas. Results from this study indicate the vast majority of EFDA providers are practicing in counties that are not considered shortage areas (Figure 1).
A majority of EFDAs in Maine are employed in private practices rather than public health or community settings and fewer than one-half of those private practices accepted Medicaid reimbursement. This finding is particularly concerning considering that an estimated 38% of children in the United States have public dental insurance (Medicaid and/or the Children's Health Insurance Program), and 12% are completely without coverage.25 The literature indicates that the number of children covered by Medicaid for dental care has doubled since 2000, almost reaching parity with private insurance utilization.26 The disparity in practices accepting Medicaid patients may still be a significant barrier to accessing oral health care for many children as well as adults. Some respondents in this study noted that the EFDA was more beneficial in public health settings than private dental practices. Multiple respondents also noted that in private practice, patients come to see that dentist specifically, not another provider.
Only 20% of procedures performed by the EFDA respondents were restorative in nature. This may be due to the incidence and prevalence of caries within their patient population; however, it could also be related to the private practice setting and the non-acceptance of public insurance (Medicaid). According to the literature, in the general population 25% of adults have untreated carious lesions, 37% of children aged 2-8 have caries in primary teeth, while 21% of children aged 6-11 and 58% of adolescents aged 12-19 have caries in permanent teeth.7
In 2010, the Centers for Medicare and Medicaid set a target of 52% of children enrolled in Medicaid or Children's Health Insurance Program utilizing preventive services.25 Despite these increased efforts through new workforce models, this national target has not been met and socioeconomic status remains a significant barrier. Higher socioeconomic status has been shown to be directly associated with decreasing caries incidence.26 Positive findings in this study relate to the national preventive care goal; respondents reported that almost two-thirds of the procedures they performed were preventive in nature. Fluoride and sealant application were both equally provided at 22%, while pediatric prophylaxis was 14% of the reported procedures. However, these findings should be further examined, as they could be due to the number of EFDA respondents (40%) who were also licensed dental hygienists; these procedures are already a part of regular dental hygiene practice. It could be that the majority of the EFDA providers in Maine (60%) may not be performing preventive procedures.
EFDA providers in Maine may be encountering challenges to providing care to the populations they were intended to serve. In addition to types of practice settings and acceptance of public insurance reimbursement, limitations surrounding direct supervision for EFDA duties presents a significant challenge. Barriers related to supervision requirements underscores the necessity of including direct access in any alternative workforce model. Direct supervision requirements restrict EFDAs in Maine to practicing in geographic areas with dentists available and willing to employ them, thus limiting their overall impact in providing access to care for underserved populations. The majority of EFDAs licensed in Maine practice in Penobscot County, which is not a designated provider shortage area.
Currently, nearly 40 states allow some form of direct access to dental hygienists, but this does not necessarily apply to other oral health workforce models.27 While licensed hygienists in Maine may provide direct access if licensed as an independent practice dental hygienist or have public health supervision authority; they are not permitted to perform EFDA delegable duties without the direct supervision of a dentist employer. Direct access has been shown to improve access to care and reduce oral health disparities where it is available.27-28 However, there are several limitations to EFDA duties related to providing direct access to care. EFDA practitioners may only perform reversible procedures and require a dentist for restorative tooth preparation before placing the amalgam or composite restoration.
Adjustments to the EFDA scope of practice to allow for direct access to preventive procedures including pediatric prophylaxis and sealants could potentially expand access to care. Several states allowing for direct access to dental hygiene care require additional education and practice beyond the entry level to ensure competent practitioners with a wider base of knowledge for less supervised practice. Requirements for direct access procedures in Oregon include 500 hours of clinical practice in a community setting during dental hygiene education, or an additional 2,500 hours of clinical practice if already licensed for the Expanded Practice Permit.29 Additionally, 12 hours of continuing education is required in addition to the hours required for dental hygiene licensure per renewal cycle.29
The state of Maine has both preparatory education and additional continuing education requirements for EFDA licensure. Practitioners interested in becoming an EFDA must complete a formal education program approved by the Maine Board of Dental Practice and complete a total of 50 hours of continuing education during each five-year renewal cycle.22 Respondents from this study indicated an average of 35% of the total number of continuing education courses per renewal cycle were directly related to EFDA practice. This finding is concerning as the content of continuing education coursework is a critical for licensure and maintaining competency. The Commission on Dental Accreditation requires that dental hygiene educators routinely complete continuing education in their course content areas to remain current and competent.30 Continuing education requirements for EFDAs should also be reflective of their range of duties.
A number of EFDA/CDA respondents (21%) indicated a desire to learn to administer local anesthesia and nitrous oxide and oxygen sedation in order to improve their impact on the access to care. The scope of practice for such functions would require significant increases in basic preparatory education and continuing education content for CDA/EFDAs as well as for licensed dental hygienists not holding a local anesthesia permit. This presents a significant challenge to increasing delegable duties as the majority of respondents were EFDA/CDAs with limited formal educational background. Certification by the Dental Assisting National Board indicates minimum, entry level competency, there are no formal education requirements to become a CDA, or to be a dental assistant in Maine. In addition, Maine does not recognize dental assistants in the practice act unless they have earned the EFDA credential.
There were limitations to this study including self-reporting bias inherent in survey research. Another limitation was that respondents were not asked to indicate whether the EFDA procedure was performed on a pediatric versus an adult patient. Additionally, respondents were not asked to indicate what percentage the EFDA delegable duties comprised with respect to the overall practice. Finally, the response rate (59%) was not indicative of all EFDAs licensed in Maine.
Conclusion
Consistent and regular assessments of alternative dental workforce models intended to decrease disparities in access to oral health care are needed to determine the impact of these models and improvement areas. EFDA practitioners in Maine routinely provide restorative and preventive care. However, the majority of EFDAs practice in locations not identified as provider shortage areas and may not be providing access to care for the intended populations. Consideration should be given to the existing barriers including direct supervision requirements when implementing alternative workforce models intended to increase access to care. Future studies should focus on the specific patient populations of EFDA providers, assessments of patients' perceptions of access to EFDA services and the care provided.
Acknowledgements
This project received funding from a University of Maine at Augusta Presidential Research Grant.
Nancy Foster, RDH, EFDA, CDA, EdM is an associate professor in the Dental Health Programs, University of Maine at Augusta, Bangor, ME, and a clinical lecturer in the Department of Periodontics and Oral Medicine, University of Michigan School of Dentistry, Ann Arbor, MI.
Amanda Willette, CDA, EFDA, MSEd is an assistant professor and dental assisting coordinator in the Dental Health Program, University of Maine at Augusta, Bangor, ME.
Danielle Furgeson, RDH, MS, DHSc is a clinical assistant professor and graduate program director in the Department of Periodontics and Oral Medicine, University of Michigan, School of Dentistry, Ann Arbor, MI.
Corresponding author: Danielle Furgeson, RDH, MS, DHSc; furgeson@umich.edu
References
1. US Department of Health and Human Services. Oral health in America: a report of the surgeon general [Internet].Rockville (MD): National Institute of Dental and Craniofacial Research; 2000 [cited 2018 August 5]. 322p. Available from: https://profiles.nlm.nih.gov/ps/retrieve/ResourceMetadata/NNBBJT
2. Center for Disease Control and Prevention. At a glance 2016: Oral health: Working to improve oral health for all Americans [Internet]. Washington DC: Department of Health and Human Services; 2016 [cited 2018 Jul 27]. Available from: http://www.cdc.gov/chronicdisease/pdf/aag-oral-health.pdf
3. Guarnizo-Herreño CC, Wehby GL. Children's dental health, school performance, and psychosocial well-being. J Pediatr. 2012 Dec;161(6):1153-9.
4. Jackson SL, Vann WF, Kotch JB, et al. Impact of poor oral health on children's school attendance and performance. Am J Public Health. 2011 Oct;101(10):1900-6.
5. Kelekar U, Naavaal S. Hours lost to planned and unplanned dental visits among US adults. Prev Chronic Dis. 2018 Jan11;(15):1-7.
6. Nasseh K, Vujicic M. Dental care utilization steady among working-age adults and children, up slightly among the elderly [Internet]. Chicago (IL): American Dental Association Health Policy Institute; 2016 Oct [cited 2018 Jul 27]. 11p. Available from: https://www.ada.org/en/~/media/ADA/Science and Research/HPI/ Files/HPIBrief_1016_1
7. Dye BA, Thornton-Evans G, Li X, Lafolla TJ. Dental caries and tooth loss in adults in the United States, 2011- 2012: NCHS data brief number 197. Washington DC: National Center for Health Statistics; 2015 May [cited 2018 Jul 27]. 8p. Available from: https://www.cdc.gov/nchs/data/databriefs/db197.pdf
8. Slavkin H. A national imperative: oral health services in Medicare. J Am Dent Assoc. 2017 May;148(5):281-3.
9. Avalere Health. Evaluation of cost savings associated with periodontal disease treatment benefit [Internet]. Washington, DC: Avalere Health; 2016 Jan [cited 2018 Jul 28]. Available from: https://oralhealth.hsdm.harvard.edu/files/oralhealth/files/avalere_health_estimated_impact_of_medicare_periodontal_coverage.pdf
10. Lewis CW, McKinney CM, Lee HH, et al. Visits to US emergency departments by 20- to 29-year-olds with toothache during 2001-2010. J Am Dent Assoc. 2015 May;146(5):295-302.
11. US Department of Health and Human Services. Healthy People 2020 oral health overview [Internet]. Washington, DC: US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. c2014 [Modified 2019 Aug 14; cited 2018 Jul 28]; [about 3 screens]. Available from: https://www.healthypeople.gov/2020/topics-objectives/topic/oral-health
12. Darling BG, Kanellis MJ, McKernan SC, Damiano PC. Potential utilization of expanded function dental auxiliaries to place restoratives. J Public Health Dent. 2015 Spring ;72(2):163-8.
13. US Department of Health and Human Services. Health resources and services administration data warehouse [Internet]. Washington, DC: US Department of Health and Human Services; c2018 [Modified 2019 Aug 17; cited May 1, 2018]. Available from: https://data.hrsa.gov/maps/quick-maps?config=mapconfig/HPSADC.json
14. Simmer-Beck M, Walker M, Gadbury-Amyot C, et al. Effectiveness of an alternative dental workforce model on the oral health of low-income children in school-based setting. Am J Public Health. 2015 Sep;105(9):1763-9.
15. Beazoglou TJ, Chen L, Lazar VF, et al. Expanded functions allied dental personnel and dental practice productivity and efficiency. J Dent Educ. 2012 Aug; 76(8):1054-60.
16. American Dental Hygienists' Association. Restorative duties by state [Internet]. Chicago: American Dental Hygienists' Association; 2016 Apr [cited 2018 Jul 28]. 2 p. Available from: https://www.adha.org/resources-docs/7516_Restorative_Duties_by_State.pdf
17. Market Decisions Research and Hart Consulting. Maine shared needs assessment and planning process for Androscoggin county [Internet]. Augusta: Maine Center for Disease Control and Prevention and Hart Consulting Inc; 2016 Feb [cited 2018 Jul 21]. Available from: https://www.maine.gov/dhhs/mecdc/phdata/SHNAPP//documents/county-reports/whole-reports/Maine%20Shared%20CHNA%20ANDROSCOGGIN%20County%20Report-2-29-16.pdf
18. Maine Equal Justice Partners. Maine's medical assistance programs-who's covered and who's not [Internet]. Augusta: Maine Equal Justice Partners; 2017 [cited 2019 Aug 20]. Available from: https://mejp.org/content/maines-medical-assistance-programs-whos-covered-and-whos-not
19. Health Resources and Services Administration. Health professional shortage areas [Internet]. Rockville (MD): Division of Data and Information Services, Office of Information Technology, Health Resources and Services Administration; 2018 [cited 2018 Jul 29]. Available from: https://data.hrsa.gov/tools/shortage-area/hpsa-find
20. Maine Center for Disease Control and Prevention. Oral health in Maine [Internet]. Augusta (ME): Maine Center for Disease Control and Prevention; 2013 Jan [cited 2018 Jul 29]. Available from: https://www.Maine.gov/dhhs/mecdc/population-health/odh/documents/oral-health-in-Maine-2013.pdf
21. Contreras O, Sterwart D, Valachovic R. ADEA data brief examining America's dental safety net [Internet]. Washington, DC: American Dental Education Association; 2018 Apr [cited 2018 Jul 6]. Available from: https://www.adea.org/policy/white-papers/Dental-Safety-Net.aspx
22. Maine Board of Dental Practice. Maine dental practice act rules for dental assistants, chapter 3 [Internet]. Augusta (ME): Maine Board of Dental Practice; 2010 Jun [cited 2018 Jul 6]. Available from: https://www.maine.gov/sos/cec/rules/02/chaps02.htm#313
23. American Dental Hygienists' Association. Direct access states [Internet]. Chicago (IL): American Dental Hygienists' Association; 2018 [cited 2018 Jul 18]. Available from: https://www.adha.org/resources-docs/7513_Direct_Access_to_Care_from_DH.pdf
24. American Dental Hygienists' Association. Expanding access to care through mid-level oral health practitioners [Internet]. Chicago (IL): American Dental Hygienists' Association; 2018 [cited 2018 Sept 8] Available from: https://www.adha.org/resources-docs/Expanding_Access_to_Dental_Therapy.pdf
25. Shariff JA, Edelstein BL. Medicaid meets its equal access requirement for dental care, but oral health disparities remain. Health Aff (Millwood). 2016 Dec 1;35(12):2259-67.
26. Curtis AM, VanBuren J, Cavanaugh JE, et al. Longitudinal associations between dental caries increment and risk factors in late childhood and adolescence. J Public Health Dent. 2018 Sep;78(4):321-28.
27. Naughton DK. Expanding oral care opportunities: direct access care provided by dental hygienists in the United States. J Evid Based Dent Pract. 2014 Jun;14:171-82.
28. Turner S, Tripathee S, MacGillivray S. Direct access to DCPs: what are the potential risks and benefits? Br Dent J. 2013 Dec; 215(11):577-82.
29. Oregon Board of Dentistry. State of Oregon dental practice act [Internet]. Portland (OR): Oregon Board of Dentistry; 2016 Jan [cited 2018 July 26]. Available from: https://digital.osl.state.or.us/islandora/object/osl%3A7628/datastream/OBJ/view
30. Commission on Dental Accreditation. Accreditation standards for dental hygiene education programs [Internet]. Chicago (IL): American Dental Association; 2018 Feb [cited 2018 July 26]. Available from: https://www.ada.org/~/media/CODA/Files/2019_dental_hygiene_standards.pdf?la=en