You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Relationships between patients and their health care providers has been shown to be of importance in accepting treatment and patient compliance.1 In medicine, research has shown that the patient-provider relationship affects a wide range of cooperative patient behaviors including medication adherence for Type 2 diabetes,2 medication compliance following coronary bypass surgery,3 exercise regimens for patients with osteoarthritis,4 medication protocols for HIV+ patients,5 and general medication adherence in the elderly.6 In dentistry, Patel et al. demonstrated that patients' acceptance of a surgical periodontal treatment plan was a function of their relationship with their provider,7 and Inglehart et al. found that the frequency of wearing a bite splint was related to the quality of the patient-provider relationship.8
Considering the significance of patient-provider relationships, it is important to gain an understanding of the influencing factors. One aspect, extensively investigated in medicine, is the degree to which a health care provider's appearance, specifically clinic attire, hairstyle, and accessories, affect patients' responses to provider recommendations. Research as early as 1987 showed patients had certain preferences for physician attire9 and traditional attire received more positive responses, while casual, non-traditional clothing choices resulted in more negative responses.10 These views have not changed substantially over the years as even in the most recent decade, patients have indicated preference for white coats as clinic attire.11,12 Traditional professional attire has been shown to inspire more confidence in the provider,13,14 made patients more comfortable,15 and increased patients' perceptions of a physician as being more empathetic16 and more professional.17 While professional clinic attire has been shown to demonstrate a positive effect in terms of professionalism, research has shown that clinic attire had no impact on patients' satisfaction18 and that surgeons' clothing had no effect on patients' opinions regarding the care they had received.19
Nursing literature has also shown that professional clinic attire was preferred by adult patients20 and nurses, and that nurses wearing solid color scrubs, as compared to prints, were viewed as being more skilled and knowledgeable.21 It is noteworthy, however, that white uniforms have been shown to make children more anxious22 and fearful.23 In dentistry, only six studies were found related to this issue, with three focusing on pediatric patients' preferences for different clinic attire styles.24-26 Again, support was found for adult patients' preferences for dentists wearing what is considered to be professional clinic attire.27,28 Additionally, most female dentists preferred lab coats to other types of clinic attire due to infection control concerns.29
No research to date explored the effects of clinic attire on patients' perceptions of dental hygienists, nor has any previous study in the dental literature assessed the impact of hairstyles and accessories on patients' perceptions of their providers. In medicine, research has shown that physical attributes such as hairstyles can have a significant impact on patients' perceptions of their physicians,10 with certain hairstyles (i.e., short hair) being preferred by patients,30 and special attention being given to well-groomed beards and mustaches.31 However, when Brosky et al. asked patients at the Minnesota School of Dentistry to rate the appearance of the dental students and faculty members in the dental clinics, hairstyle was shown to have little impact on patients' opinions of their provider possibly due to their findings that the majority of the respondents described all providers as having a professional appearance.27
Concerning patients' opinions regarding accessories, research in medical settings has shown that earrings, especially when worn by male providers, were viewed negatively or as unprofessional,10,32,33 with nose and lip piercings being most negatively evaluated.33 In another study, patients indicated that the absence of visible tattoos (30%) and the absence of visible piercings (39%) were important factors.34 However, the location of the practice35 and the patients' age might be significant mediators for patients' perceptions and evaluations in this context.36 Research in dentistry has also shown that patients positively evaluated providers who wore a name tag, safety glasses and a mask.28,37
Provider and patient gender may also be a mediating factor when considering the effects of what is considered to be a professional appearance, specifically in the aspects of clinic attire, hairstyle and accessories, on patients' perceptions of their health care providers.38 However, very limited research has focused on the role of gender and professionalism. The purpose of this study was to explore whether a dental hygienists' clinic attire, hairstyle, and accessories affected patients' and dental student providers' perceptions of their professionalism and the role gender plays in these perceptions.
Methods
This study utilized a quasi-experimental design, with subjects randomly assigned to view different photographs of hygienists. This research was determined to be exempt from oversight by the Institutional Review Board for the Behavioral and Health Sciences at the University of Michigan, Ann Arbor, MI (HUM#00055794).
An a priori power analysis was conducted to compute the sample size needed to have the power to conduct analyses of variance. It showed a minimum of 269 subjects would be required. Adult patients receiving care at the University of Michigan School of Dentistry were informed about the study and invited to participate in the anonymous survey. Agreeing to respond and complete the survey was considered implied consent. Participants received a free parking voucher upon completion of the survey as a token of appreciation. First and second year dental students comprised the second cohort of participants. Students were informed about the research study at the end of a regularly scheduled class period and invited to respond to an anonymous survey. No instructors were present during the recruitment effort. Students received the surveys and returned them anonymously to the research team.
Each survey consisted of demographic background questions (gender, age, and educational status) and 6 additional sections. Each of the 6 sections contained a photograph of a clinician (dental hygienist) followed by five questions. Three physical characteristics (hairstyle, clinic jackets and ear jewelry/accessory) were selected for evaluation. Traditional hairstyles, clinic jacket and earring characteristics were considered to be "professional" whereas less-traditional characteristics were considered to be "unprofessional" for the purposes of this study. Male and female clinicians were photographed for each characteristic. Participants were asked to evaluate the clinician photographed based on how professional and hygienic the clinician appeared, their level of confidence in the clinician's abilities, their level of trust in the clinician, and whether they would want to be treated by the clinician. Responses were given on a 7-point answer scale ranging from 1 = "not at all" to 7 = "very much." Participants received three randomly selected sections with male clinician photographs and three sections with female clinician photographs (Figure 1).
The survey was piloted tested by 30 dental hygiene students enrolled in a research methodology class. Changes in the wording of the questions were made based on the feedback received. In addition, a factor analysis (Extraction Method: Principal Component Analysis; Rotation Method: Varimax Rotation) was used to determine if the 5 items loaded on one underlying factor to assess for construct validity. The reliability of the 5-item scales was determined with Cronbach alpha inter-item consistency scores and the reliability was considered to be excellent.
Descriptive statistics, such as percentages and means, were computed to provide an overview of the responses. Independent sample t-tests were used to compare the mean responses to professional versus unprofessional/less traditional photographs. Two- and three-way analyses of variance were used to test whether the average responses in regard to the male versus female clinicians with professional versus unprofessional/less-traditional appearance differed and whether male versus female respondents' mean responses differed in regard to the gender of the clinicians photographed with various physical attributes.
Results
A total of 402 adult patients ranging in age from 18 to 93 years (n=402; mean: 54 years) and 318 first- and second-year dental students ranging in age from 20 to 40 years (n=318; mean: 25 years) consented to participate. Participant demographic information is shown in Table I.
In general, all of the clinicians depicted in the photographs were rated positively for the three areas of consideration: hairstyle, clinic attire, and ear accessories with means ranging from 4.85 to 6.12 on a 7-point answer scale, with "7" indicating the most positive rating.
Male and female clinicians with less traditional hairstyles were on average rated as less professional and less hygienic; respondents were less confident in their abilities, had less trust in them, and had less of a desire to be treated by them. Ratings of professionalism were not affected whether the clinician photographed wore a white, traditional clinic jacket versus a blue jacket. Clinicians photographed wearing unprofessional/less-traditional ear accessories (i.e., ear plugs) were rated on the average as less professional than clinicians with professional accessories. Responses for all three areas of consideration (means and standard deviations) are shown in Table II.
The gender of the clinician photographed was shown to have a significant effect on the respondents' rating levels in all three areas (hairstyle, clinic attire, and ear accessories). In all three areas, male clinicians were rated as less professional than the female clinicians in all five of the related response items (main effect: clinician gender). The interaction effects between the photographed clinician's gender and their professionalism ratings were also significant for each dependent variable for hairstyles and clinic attire. Female providers with a professional hairstyle received the most positive evaluations, while the male provider with the unprofessional/less-traditional hairstyle received the least positive evaluations.
A slightly different pattern of responses was found for the five mean ratings of the male versus female providers and clinic attire. The female provider with the white clinic jacket had the most positive mean evaluations, while the male provider with the white jacket was viewed less positively. No significant interaction effects were found between the clinician gender and the professionalism ratings of ear accessories. An overview of the professionalism ratings of the male versus female clinicians comparing the professional versus unprofessional/less-traditional hairstyles, clinic jackets, and ear accessories is shown in Table III.
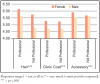
Given that the ratings of clinicians with different hairstyles had an inter-item consistency of Cronbach alpha=.947, the ratings of clinicians with different clinic jackets had an alpha of .949, and the ratings of clinicians with different ear accessories had an alpha of .965, three indices were computed as a measure of overall professionalism by averaging the five responses in each of the three appearance categories. Female depicted clinicians were consistently more positively evaluated in each of the three categories as compared to the male depicted clinicians (Figure 2).
In addition to analyzing the effect of the depicted clinician's gender (Table III) differences in the gender of the respondents' evaluations of the professional versus unprofessional/less-traditional characteristics were also investigated first for female clinicians and followed by a second set of analyses for male clinicians. The interaction effects of "participant gender" and "type of hairstyle" were significantly different for all five questions related to hairstyle in the analysis of female clinicians. Female participants consistently rated female clinicians with professional hairstyles most positively on all five attributes and consistently rated female clinicians with unprofessional/less traditional hairstyles least positively, while male participants' responses fell between the female subjects' responses. Female evaluations of male clinicians with professional hairstyles were also rated most positively compared to the overall evaluations of male participants (Table IV).
The type of clinic jacket and ear accessories worn by female clinicians did not result in significantly different evaluations by male versus female participants, nor did the type of ear accessories worn by male clinicians. However, male and female participants differed in their evaluations of male clinicians and the type of clinic jacket worn (Table IV).
One final question examined was whether patient participants differed from dental student participants in their ratings of the male versus female clinicians in each of the appearance categories (Table V). While there was no significant main effect of the participants' role (dental student versus patient) for the hairstyle and clinic jacket related responses, dental students consistently evaluated the depicted female and male clinicians in the ear accessory category more negatively than the patients. When analyzing whether students versus patients differed in their responses to female versus male depicted clinicians with professional or unprofessional/less traditional hairstyles, the data showed that students consistently evaluated female clinicians with unprofessional hairstyles less positively than the patients. Patients however, consistently rated male depicted clinicians with unprofessional/less traditional hairstyles least positively.
Discussion
Medical and dental1-8 research explored which role relationships between patients and clinicians can play in patients' treatment acceptance and compliance. Gaining a better understanding of the factors impacting these relationships is critical to improving patient care outcomes. One significant factor in this context is the perceived level of professionalism of health care providers in medicine and dentistry.10-29 The Commission of Dental Accreditation (CODA) included Standard 2-19 on ethics and professionalism among their CODA standards for dental hygiene education programs.39 Consequently, dental hygiene students learn the aspects of professionalism during their education,40 and graduates strive to uphold the dental hygiene oath to maintain the highest standards of professional competence and personal conduct.41
Dental hygienists' overall appearance may be viewed as one aspect of personal conduct and has been shown to play a role in patient-provider interactions. Research in medicine has shown that unprofessional hairstyles,10,30,31 clinic coats9-17and accessories10,32-34negatively affected patients' evaluations. This study focused on how patients and dental students, considered as future dentists, evaluated these three characteristics portrayed in photographs of both male and female dental hygienists. The descriptions of the two types of appearances described in this study as professional vs. unprofessional/less traditional, deserve further discussion. The dental school in which this study was conducted has clearly defined appearance guidelines in their best practices' clinic guide. The photographs described in this study as "professional" followed these guidelines while the photographs described as "unprofessional" did not follow the guidelines. However, for the general population or for the patient participants in this study, the distinction between what is considered to be professional and unprofessional appearance may differ greatly. Patients' own values might affect their responses to dental hygienists' attire and physical characteristics. To reflect this possibility, the term "less traditional" was added to the term "unprofessional." In addition, dental students, as future dentists and potential employers, may develop their perceptions of professionalism based on their experiences as students. Including dental students in the study population, added an additional perspective to the data.
Overall, an unprofessional/less traditional hairstyle resulted in significantly fewer positive evaluations than a professional hairstyle. However, wearing a white (professional) vs. blue clinic jacket did not affect the average evaluations in this study. It is possible that more casual outfits such as cartoon print scrubs or wearing casual clothing such as jeans or exercise gear might result in more negative evaluations. Wearing large hoop earrings or gauges also did not result in overall more negative evaluations. While these two ear accessories did not affect patients' and dental students' evaluations, it is possible that other accessories such as large earrings worn by male providers,10,32,33 nose and lip piercings,33,34 and visible tattoos34 might have a negative effect on the evaluations, and wearing a name tag, safety glasses and a mask might have more positive effects.28,37 The practice location35 and the patients' age and ethnicity might also be significant moderators for patients' perceptions and evaluations of professionalism.36
One interesting question is whether these overall perceptions prevail when the clinicians' gender is considered. Given that an estimated 98% of dental hygienists in the United States are female42 and only about 4.2% of current dental hygiene students are male,43 it could be both patients and dental students/future dentists apply different considerations for the majority of female dental hygienists versus the minority of males in the profession. Findings from this study showed that overall, photographs of male dental hygienists were consistently more negatively evaluated than females. This finding could imply that educational interventions are needed to inform the public about the increasing numbers of male dental hygienists.
Responses of male versus female participants did not differ overall in this study. However, when the interaction between gender and perceptions of professionalism were explored, the data showed that female patients and dental students rated female dental hygienists with unprofessional/less traditional hairstyles more negatively than male patients and dental students. In addition, dental students seem to apply higher standards overall regarding professionalism than patients.
This study has several limitations. First, a quasi-experimental design with photographs of male and female clinicians was used. In each category evaluated (hairstyle, clinic attire and ear accessory), the same male and female clinicians portrayed both the professional and the not professional/less traditional appearances. However, it cannot be ruled out that the three males and the three females used in this study were not markedly different. Future studies should consider using photographs from the same male and female clinicians for each type of appearance in all three categories. A second limitation was the absence of photographs of clinicians from non-European backgrounds, limiting the generalizability of the findings. Future research should explore the role of ethnicity/race in the context of professional appearance of providers. A third limitation was that this study was conducted in a mid-sized city in the Midwestern United States. Cultural and social norms in major cities such as New York or Los Angeles or in rural areas differ and may affect the evaluations of the characteristics studied. Future research should also consider standardizing the photographs in regard to background and photo size. The lack of standardization of the photographs within and across the sets may have resulted in error variance of the responses. Finally, first- and second-year dental students do not have extensive clinical experiences and may not be ideal respondents when exploring the role of one's professional education and experiences on evaluations of professionalism. Future studies may consider collecting data from practicing dental hygienists and dentists.
Conclusions
Findings from this study showed that hairstyle, in both male and female dental hygienists, was viewed as a physical characteristic that influenced perceptions of professionalism among both patients and dental students. In general, male clinicians were viewed as being less professional than females, regardless of hairstyle, clinic attire or ear accessory. While the gender of the patient or dental student participant was not shown to significantly affect the perceptions of professionalism, both female patients and female students viewed the female clinician with an unprofessional/less traditional hairstyle most negatively. Characteristics of physical appearance may affect patients' and future dental providers' perceptions of professionalism in dental hygienists.
Acknowledgments
The authors would like to thank Dean H.M. Chenensky, Nirali Kadakia, and Benjamin Yoon for their help with the data collection and preparation for analysis and the University of Michigan Undergraduate Research Opportunity Program (UROP) for their financial support for the payment of the parking vouchers.
About the Authors
Michael B. O'Brien, BA is a research assistant, Department of Periodontics and Oral Medicine, School of Dentistry, University of Michigan, Ann Arbor, MI; Ashley Copus, RDH, BS is a dental hygienist in private practice; Julia Johnson, RDH, BS is a dental hygienist in private practice; Marita R. Inglehart, Dr phil habil is a professor, Department of Periodontics and Oral Medicine, School of Dentistry and adjunct professor, Department of Psychology, College of Literature, Science and Arts, University of Michigan, Ann Arbor, MI.
Corresponding author: Marita R. Inglehart; mri@umich.edu
References
1. Ley P. Communicating with patients: Improving communication, satisfaction and compliance. Psychology and Medicine Series. New York, NY. Croom Helm. 1988. 210 pages.
2. Brundisini F, Vanstone M, Hulan D, et al. Type 2 diabetes patients' and providers' differing perspectives on medication nonadherence: a qualitative meta-synthesis. BMC Health Ser Res. 2015 Nov;15:5.
3. Sengstock D, Vaitkevicius P, Salama A, et al. Under-prescribing and non-adherence to medications after coronary bypass surgery in older adults: strategies to improve adherence. Drugs & Aging. 2012 Feb;29(2):93-103.
4. Marks R. Knee osteoarthritis and exercise adherence: A review. Curr Ag Sci. 2012 Feb; 5(1):72-83.
5. Apollo A, Golub SA, Wainberg ML, et al. Patient-Provider relationships, HIV, and adherence. Soc Work Health Care. 2006;42(3-4):209-24.
6. Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly: looking beyond cost and regimen complexity. Am J Geriatr Pharmacother. 2011 Feb;9(1):11-23.
7. Patel AM, Richards PS, Wang H, et al. Surgical or non-surgical periodontal treatment? Factors affecting patient decision making. J Periodontol. 2006 Apr;77(4):678-83.
8. Inglehart MR, Widmalm SE, Syriac PJ. Occlusal splints and quality of life: Does the quality of the patient-provider relationship matter? Oral Health Prev Dent. 2014 Sept;12(3):249-58.
9. Dunn JJ, Lee TH, Percelay JM, et al. Patient and house officer attitudes on physician attire and etiquette. JAMA. 1987 Jan;257(1):65-8.
10. Gjerdingen DK, Simpson DE, Titus SL. Patients' and physicians' attitudes regarding the physician's professional appearance. Arch Intern Med. 1987 Jul;147(7):1209-12.
11. Chang DS, Lee H, Lee H, et al. What to wear when practicing oriental medicine: patients' preferences for doctors' attire. J Altern Compl Med. 2011 Aug;17(8):763-7.
12. Jabbal, A. Medical student dress code in the orthopaedic out-patient department. Clin Teach. 2014 Dec;11(7): 507-11.
13. Budny AM, Rogers LC, Mandracchia VJ, et al. The physician's attire and its influence on patient confidence. J Am Pediatr Med Assoc. 2006 March-Apr;96(2):132-8.
14. McKinstry B, Wang JX. Putting on the style: what patients think of the way their doctor dresses. Br J Gen Pract. 1991 Jul;41(348):270,275-8.
15. Lill M, Wilkinson TJ. Judging a book by its cover: descriptive survey of patients' preferences for doctors' appearance and mode of address. BMJ. 2005 Dec;331(7531):1524-7.
16. Chung H, Lee H, Chang DS, et al. Doctor's attire influences perceived empathy in the patient-doctor relationship. Patient Educ Couns. 2012 Dec;89(3):387-91.
17. Gooden BR, Smith MJ, Tattersall SJ, et al. Hospitalized patients' views on doctors and white coats. Med J Aust. 2001 Aug 20;175(4):219-22.
18. Fischer RL, Hansen CE, Hunter RL, et al. Does physician attire influence patient satisfaction in an outpatient ob-gyn setting? Am J Obstet Gynecol. 2007 feb;196(2):186.e1-5.
19. Edwards RD, Saladyga AT, Schriver JP, et al. Patient attitudes to surgeons' attire in an outpatient clinic setting: substance over style. Am J Surg. 2012 Nov;204(5):663-5.
20. Albert NM, Social L, Meyer KH, et al. Impact of nurses' uniforms on patient and family perceptions of nurse professionalism. Appl Nurs Res. 2008 Nov;21(4):181-90.
21. Thomas CM, Ehret A, Ellis B, et al. Perception of nurse caring, skills, and knowledge based on appearance. J Nurs Adm. 2010 Nov;40(11):489-97.
22. Roohafza H, Pirnia A, Sadeghi M, et al. Impact of nurses clothing on anxiety of hospitalized children. J Clin Nurs. 2009 Jul;18(13):1953-9.
23. Meyer D. Children's responses to nursing attire. Pediatr Nurs. 1992 mar-Apr;18(2):157-60.
24. Kuscu OO, Caglar E, Kayabasoglu N, et al. Short communication: preferences of dentist's attire in a group of Istanbul school children related with dental anxiety. Eur Arch Paediatr Dent. 2009 Jan;10(1):38-41.
25. Mistry D, Tahmassebi JF. Children's and parents' attitudes towards dentists' attire. Eur Arch Paediatr Dent. 2009 Dec;10(4):237-40.
26. Panda A, Garg I, Bhobe AP. Children's perspective on the dentist's attire. Int J Paediatr Dent. 2014 Mar; 24(2):98-103.
27. Brosky ME, Keefer OA, Hodges JS, et al. Patient perceptions of professionalism in dentistry. J Dent Educ. 2003 Aug;67(8):909-15.
28. McKenna G, Lillywhite GR, Maini N. Patient preferences for dental clinical attire: a cross-sectional survey in a dental hospital. Br Dent J. 2007 Dec;203(12):681-5.
29. Austin GB, Tenzer A, Lo Monaco C. Women dentists' office apparel: dressing for success in an age of infection control. J Law Ethics Dent. 1991;4:95-100.
30. Hennessy N, Harrison DA, Aitkenhead AR. The effect of the anesthetist's attire on patient attitudes. Anaesthesia. 1993 Mar;48(3):219-22.
31. Matsui D, Cho M, Rieder MJ. Physicians' attire as perceived by young children and their parents: The myth of the white coat syndrome. Pediatr Emerg Care. 1998 June;14(3):198-201.
32. Menahem S, Shvartzman P. Is our appearance important to our patients? Fam Pract. 1998 Oct;15(5):391-7.
33. Newman AW, Wright SW, Wrenn KD, et al. Should physicians have facial piercings? J Gen Intern Med. 2005 Mar;20(3):213-8.
34. Au S, Khandwala F, Stelfox HT. Physician attire in the intensive care unit and patient family perceptions of physician professional characteristics. JAMA Intern Med. 2013 Mar 25;173(6):465-7.
35. Kanzler MH, Gorsulowsky DC. Patients' attitudes regarding physical characteristics of medical care providers in dermatologic practices. Arch Dermatol. 2002 Apr;138(4):463-6.
36. Keenum AJ, Wallace LS, Stevens AR. Patients' attitudes regarding physical characteristics of family practice physicians. South Med J. 2003 Dec;96(12):1190-4.
37. Shulman ER, Brehm WT. Dental clinical attire and infection-control procedures. Patients' attitudes. J Am Dent Assoc. 2001 Apr;132(4):508-16.
38. Tiwari A, Abeysinghe N, Hall A, et al. Should doctors wear white coats? The patient's perspective. J Eval Clin Pract. 2001 Aug;7(3):343-5.
39. Commission on Dental Accreditation (CODA). Accreditation standards for dental hygiene education programs. [Internet]. Chicago (Ill.): Commission on Dental Accreditation; 2013 [modified:2018 Sept; cited 2019 Jan 22]. Available from: https://www.ada.org/~/media/CODA/Files/2019_dental_hygiene_standards.pdf?la=en
40. Beemsterboer PL. Ethics and law in dental hygiene. 2nd ed. St. Louis: Saunders Elsevier; 2009. Chapter 1, Ethics and professionalism; p. 3-21.
41. Cruz, N. Ethics and law in dental hygiene. Dental hygiene oath. [Internet]. StudyLib; 2013 - 2019 [cited 2019 Jan 22]. Available from: https://studylib.net/doc/9595198/ethics-and-law-in-dental-hygiene.
42. American Dental Hygienists' Association. Oral health fast facts. [Internet]. Chicago: American Dental Hygienists' Association; 2019 [cited 2019 Jan 22]. Available from: https://www.adha.org/resources-docs/72210_Oral_ Health_Fast_Facts_&_Stats.pdf.
43. American Dental Education Association. Dental hygiene by the numbers. [Internet]. Washington, DC: American Dental Education Association. 2019 [cited 2019 Jan 22]. Available from: https://www.adea.org/GoDental/Future_Dental_Hygienists/Dental_hygiene_by_the_numbers.aspx