You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The ADAA has an obligation to disseminate knowledge in the field of dentistry. Sponsorship of a continuing education program by the ADAA does not necessarily imply endorsement of a particular philosophy, product, or technique.
Methamphetamines (MA) directly affect a person's health, lifestyle, ability to function and mental status. Unlike many other street drugs, the use of meth is on the rise. Dental professionals must have knowledge of the symptoms of use, possible side effects, drug interactions with medications and dental treatment considerations. This will aid in delivering appropriate dental treatment, intervention, patient education and prevention.
According to the 2015 National Survey on Drug Use and Health, approximately 0.9 million people aged 12 or older were current users of methamphetamine, which included about 13,000 children ages 12 to 17.26 Side effects of MA on the oral cavity and the central nervous system (CNS) are severe and can include permanent brain damage.2 Results of MA use are devastating, and can have fatal consequences. MA users experience acute and chronic mental, physical, and behavioral changes. See Table 2 which compares two very dangerous, but different drugs - MA and Cocaine.
History
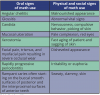
As early as 3000 B.C., Chinese writings mentioned the ephedra plant, the source of the alkaloids ephedrine and pseudoephedrine.3 First synthesized in 1887 as a medication for dealing with everything from "tired blood to breathing difficulties," meth was patented in the 1930's for use in individuals with asthma, rhinitis, and for its anorectic effects. MA's euphoric and anorectic effects were quickly recognized and led to severe abuse of the drug. Table 3 describes the effects of MA use.
During World War II, MA was used by soldiers to increase wakefulness and attention. As a result, many soldiers came home addicted to the substance. The 1940's followed with a pandemic of MA abuse. This pattern of abuse also spread to countries such as Japan and Sweden. There were very few regulations on the use of MA, which led to over-use and abuse.
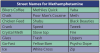
In the 1950's, substance regulations became more stringent and yet MA continued to be abused by students, athletes, truck drivers and others. The Controlled Substance Act of the 1970's (the Act was passed in 1970 and was added to continually through 1980) strictly regulated the manufacturing of this particular amphetamine. Even though there was a severe decline in the manufacturing of MA, the use of "street" meth has increased notably.4 The street name for methamphetamine varies from region to region. Table 4 offers a list of many street names for MA.
Composition
MA is a synthetic psychomotor stimulant and is closely related to decongestants, ephedrine and phenylpropanolamine.1 It is synthesized by converting the main ingredient ephedrine or pseudoephedrine (derived from the ephedra plant) into methamphetamine through a process of distillation. This process can be obtained by simply following "cookbook" directions on the internet, which includes preparation hints as well as the essential ingredients.3 The ingredients necessary are available at any hardware store, feed store and local pharmacy.
Substances such as tincture of iodine, denatured alcohol, red phosphorus, pseudoephedrine, lye, lithium, and anhydrous ammonia, are all readily available and relatively inexpensive (Table 5). Illicitly synthesized MA may be contaminated by inorganic compounds. There have been cases of exposure to many foreign substances, including lead and carcinogenic materials.4
Though many states have limited the distribution of some of the materials necessary in manufacturing street MA, many materials are available by simply crossing a state line or having several people buy from multiple sources. This problem has been compounded by the new technique called shake and bake. This technique allows the process of making methamphetamine to be cut down to 30 minutes. Utilizing something as simple as a two liter-sized plastic bottle, this lab technique can be set up in minutes.22 Though lab seizures were down, rates had decreased since 2004 when many states started placing controls on the purchases of items involved in the production. Unfortunately, rates have slowly started to return to higher levels as cooks have adapted their methods of production to the materials that are available.
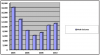
Interesting notes when looking at these statistics:
1. Seizures of large labs are down.
2. Of the small-scale laboratories seized between 2007 and 2009, the number of small-scale lithium ammonia method laboratories increased 158 percent overall, from 1,583 in 2007, to 2,584 in 2008, to 4,089 in 2009. As production is altered, the U.S. government has strived to regulate the ingredients. For example, currently bath salts have been added to the list of restricted ingredients.
Interaction
At the cellular level, methamphetamines stimulate the release and block the reuptake of neurotransmitters called monoamines (dopamine, norepinephrine, and serotonin). Several areas of the brain are affected by this cellular process and the result is a feeling of euphoria. The "rush" that many meth users report is a result of the high release of monoamines into the CNS.5
Brain imaging studies show that MA increases dopamine level in the reward center of the brain. The reward center is the mediator of addictive behavior. The results of the initial increase in dopamine to the CNS include; increased wakefulness, increased physical activity, decreased appetite, increased respiration, hyperthermia, and euphoria.
Prolonged use of MA results in a depressed dopamine level. This decrease results in symptoms like Parkinson's disease, a severe movement disorder. The continued use will lead to the reduction of dopamine being transferred throughout the body.3 Other CNS effects from the reduction of dopamine include; irritability, insomnia, confusion, tremors, convulsions, anxiety, paranoia and aggressiveness. It is important to note that hyperthermia (with temperatures as high as 108) and convulsions can result in death.1
Brains of Meth Addicts: A Breakthrough
For many generations' scientists have believed that meth can cause changes in the very way that the brain functions. Studies recently done by the University of Washington have confirmed this hypothesis. Meth can cause changes to the neurons in the brain and the synapses and terminals that control transmission of information in the brain. In this experiment utilizing mice, researchers focused on the mouse brain, and how it was affected by methamphetamine over 10 days, which is the mouse equivalent of chronic use in humans.
The study concluded that long administration and withdrawal of the drug depressed the neural terminals controlling the flow of signals between two areas of the brain, the cortex and striatum. Even a long period of withdrawal (the equivalent of years in humans) did not return the terminals to normal activity level. Re-introducing the drug, however, reversed some of the changes in the brain.
The specific areas in the brain that are affected by the drug are the pre-synaptic terminals and are related to the flow of information from the cortex to the striatum. When a person sees something new in their environment, the scientists explained, he/she focuses attention on that item. At the neuron level, that process stimulates the release of dopamine, a chemical involved in transmitting signals in the brain. As the person sees the new item over and over again, the dopamine response drops, and synapses in the brain adapt to the no-longer-new item.
Methamphetamine use makes the nervous system release dopamine, which helps a user focus a lot of attention on a particular goal or thought. Scientists believe that meth allows dopamine in the striatum to filter information coming from the cortex through the pre-synaptic terminals. The filtering of some of the terminals would help someone ignore other things and focus on that one goal or task.
Chronic use alters the filtering process and eventually becomes a permanent depression in the activity of those terminals in the brain. The challenge facing researchers is that the only way to help the pre-synaptic terminals recover in mice, was re-administering the drug. These changes to the brain may account for some of the physiological components of addiction. This finding will be vital in treating patients experiencing addiction and working toward recovery. The previous methods of lowering the dose over time which does not account for the adaptation of the neural terminals in the brain may be replaced by methods that target the chemical receptors. Studies are currently being conducted on targeting the chemical receptors of the brain to reset the system and eliminate the depressed state of the pre-synaptic terminals. Alternate methods of treating this disease are being researched with new vital information and gives increased hope for improving the rate of recovery.23
Recognizing the Physical and Mental Signs and Symptoms of Methamphetamine Abuse
Many dental professionals have treated an MA user without knowing it. The signs and symptoms of MA use are sometimes subtle and at other times clearly evident. Recognizing the signs and symptoms of meth use is vital in keeping patients safe from harming themselves, as well as others, and to create a treatment program that meets each patient's individual needs.
People react to the presence of MA in the body just as they would with the fight or flight syndrome in the presence of danger. MA floods the body with adrenaline, which is the hormone that aids in quick response during an emergency. This reaction gives the user great strength and endurance.1 One person interviewed reported staying awake for over 72 hours in order to complete the painting of his two-story home. Users often report needing less sleep and being able to withstand great amounts of work and strenuous tasks. This unreasonable sense of strength and ability can create an atmosphere for damage to the body and the brain.3
Short-term effects of meth use include vomiting, tremors, hyperactivity, and decreased appetite. Long-term effects are much more devastating, ranging from allergic reactions to strokes (Table 6). MA use causes increased heart rate and blood pressure and can cause irreversible damage to blood vessels in the brain, producing a stroke. Other effects of methamphetamine include respiratory problems, irregular heartbeat, lowered immune response and extreme anorexia. Its use can result in cardiovascular collapse and death.8
Quality of life is often altered due to the higher incidence of conditions such as Parkinson's disease3,6 and Human Immunodeficiency Virus (HIV).7 Psychiatric symptoms include anxiety, psychosis, difficulty controlling anger, violent behavior, depression, and attempted suicide.9
Case Study Involving a Dental Patient
A 27 year old male presented in the clinic with a draining apical abscess on tooth #9. His chief complaint was pain with tooth #9. Further investigation revealed that all his anterior teeth had rampant caries and most of his molars had been worn down to the gingival margin. The patient's plaque level was extremely high and he reported he did not know when he had brushed last. His eyes were dilated, his blood pressure was elevated to 165/89 and his body temperature was 104.5 degrees. While waiting for his appointment he was observed pacing back and forth while picking at his skin. He explained that he was trying to remove the bugs he was sure were embedded beneath his skin. This is known as formication. This feeling is a result of the drug constricting the capillaries near the surface of the skin, causing intense itching.6 Figure 2 illustrates formication. (Note - the accompanying figures are not those of the case study in question.)
Review of his health history revealed he had been using MA in the oral form for eight months. His diet consisted of a high carbohydrate intake in the form of soda to moisturize his dry mouth. The increase in bacteria from a lack of care, dry mouth, and lowered immune response resulted in rampant caries.
The patient's clothing was stained and the remnants of his last meal sat on his chin. He continued to pace for a short period of time and finally sat down and heaved a sigh of relief. Sweat was coming off his head and he started to scratch his skin while he lifted his shirt. His skin was raw from constant scratching and his ribs protruded. His face was gaunt and deep lines chased his sagging skin. After the needs of the patient were assessed, he was referred to a Medical Practitioner for evaluation and drug intervention before starting dental treatment.
Oral Signs and Symptoms
The use of MA has a pattern of damage in the mouth. There are several factors when combined that create an environment that destroys the teeth, the blood supply and supporting tissues. Figures 3 and 4 show two examples of oral destruction MA use can cause.
In the past, the rampant caries associated with MA use was attributed to the acidic nature of MA in the oral cavity when it was smoked. Studies involving the oral intake of the drug for narcolepsy and attention deficient hyperactivity disorder revealed the same characteristic carious lesions seen in MA users.
The current hypothesis involves a group of conditions that when combined create the perfect environment for dental disease to occur.11 MA users are unable to take care of daily tasks such as brushing and flossing due to the "crash" effect of this drug, which can last many days. When they are awake for long periods of time, the energy bursts that they experience do not allow them to concentrate on simple tasks.9
MA works as a vasoconstrictor causing blood vessels to constrict, including the vessels in the mouth. This in turn causes a lack of the blood that nourishes the periodontium and teeth properly. With repeated shrinking, the vessels will not recover, thus causing dental tissue to starve and break down. The end result is tooth decay, gum disease, and bone loss.11
The caries rate in MA abusers is four times higher than control groups.12 The dry mouth, or xerostomia, that accompanies the use of this drug leads to many problems. Without saliva, acids accumulate in the oral cavity, lowering the pH of the mouth and causing the breakdown of tooth enamel. Xerostomia is caused by the vasoconstriction and reduction of salivary gland function. The tongue and lining of the mouth can become raw and irritated without the surfactant action of saliva. This can lead to secondary infections, and limited abilities to speak and eat.8
Many patients try to reduce the dryness by taking in sugary sodas or juices. These drinks, coupled with decreased home care, vomiting, and decreased immune response creates the perfect environment for rampant caries and periodontal disease to occur.
Some chemicals used to manufacture MA are caustic, causing chemical burns to the skin. These harmful chemicals will also come into contact with the soft tissue or mucosal lining of the oral cavity. Without the buffering effects of saliva present to protect the oral tissues, severe inflammation, painful mouth sores, and ulcers can develop.3,4,8 Table 7 offers several signs associated with MA use.
The pattern of decay is distinctive in that, initially, it involves the smooth buccal surface of posterior teeth and the interproximal of the anterior teeth. It eventually leads to the complete destruction of the coronal portion of the tooth.1,3,12
MA users are chronic grinders and clinchers due to the muscle constriction that accompanies MA use. Grinding quickly wears down the teeth to small nubs. Grinding and clinching were once attributed to the impurities of the processing in homemade laboratories. There is no current clinical evidence to support this theory.11 Youth are known to use infant pacifiers to help alleviate these symptoms.
The other result of the vasoconstriction of blood vessels is the gaunt look and quick aging of patients. (Figure 5) Tissues of the face quickly die and result in a sagging appearance due to a lack of nutrients and blood supply.2,3,9 This aging affect can be seen in before and after photos and is irreparable. The intense itching that many MA users experience is known as formication - the constriction of capillaries near the surface of the skin. Compulsive scratching often leads to infection and bacterial cellulitis.6
Treatment Considerations and Planning
Being aware of the signs and symptoms of meth abuse is the first step of treatment. (Tables 6 and 7) Updating the health history, communicating concerns, assessing the current use of MA, and referring for rehabilitation must occur before treatment begins.
MA users have a higher tolerance for anesthetics, a reduced ability to metabolize medications, and a greater chance of a drug interaction.13 Dental professionals must communicate with the patient and discover when the last dose of MA occurred. No vasoconstrictors should be used within 24 hours of MA use. An increase in blood pressure from vasoconstrictors, such as epinephrine, can lead to a stroke or cardiac arrest.14 Sharing these facts with the patient may help them to feel comfortable to share their MA habits.
Using frank, direct questions that are non-judgmental will aid in quick diagnosis. The health history can help in the screening process. Include questions such as "Do you have a history of drug dependency?" on the health history. Document all conversations on drug use and history in the patient's chart. It is important to include the patient's report of the last date of use and the medications that are prescribed for the patient or drugs taken by the patient.
After initial examination ask open ended questions such as "How did your teeth get to be this way?" Further conversation can include comments such as, "Normally, we don't see this kind of decay and/or tooth damage very often. It usually happens if someone drinks excessive amounts of sugary soda or takes drugs." You may have to ask, "Have you used Meth or are you using now?" Point out the signs of damage to the patient that can be seen clinically. Express concern and use the opportunity to educate your patient while discussing their dental findings. Present the facts non-judgmentally, explaining how important it is to stop now. Once the patient's needs have been determined there are many treatments that can be recommended to prevent further damage.
Pain control: No patient should have to live with pain. The typical MA patient may not experience the pain you would expect from such extensive caries because MA can block or lessen pain receptors. Other patients will have such severe pain that it is difficult for them to eat. Dr. James Hill has developed a special understanding of the pain needs of MA patients. Dr. Hill practices general dentistry in the California Correction system. Dr. Hill stated, "The most important thing that I can do is help to restore people's self-image and self-esteem. It is so important that I treat them as I would want to be treated. I would not want to be in pain, and I should do everything that I can to help my patients get out of pain." Dr. Hill explained he is seeing an increasing number of patients with the severe effects of MA use. He said, "It is very frustrating to watch someone go through the process of extensive pain and losing all their teeth but, having someone turn their life around after receiving treatment makes it all worthwhile."19
Unless there are contraindications, anti-inflammatory medications should be the first drug of choice for pain control as they are very effective at relieving pain. Prescribing narcotics should be avoided. Cardiac reactions have been reported when mixing narcotics with MA. Patients addicted to MA will use narcotics to increase the high. Pain control in the office should include use of a long-lasting anesthetic such as Marcaine® if the patient has not had meth in the last 24 hours.13 If the dental team is unsure if the patient has used MA in the past 24 hours, anesthetic should not be administered. When using anesthetic, vasoconstrictors should be avoided. Caution should be used when using general anesthesia and nitrous oxide as adverse reactions can occur when mixing drugs.
If it becomes necessary to prescribe narcotics for a known MA user, consider asking permission to discuss any prescriptions with the patient's drug counselor, sponsor, or medical doctor. It is important to include in this discussion the proper use of the medication, limits of use, and side effects. Some patients will use their extensive decay to get prescriptions for painkillers. Dental offices should be extremely cautious when prescribing narcotic drugs, especially if they are not patients of record.
Patients may go "doctor shopping" from one dental office to another to obtain drugs. The Substance Abuse and Mental Health Services Administration (SAMHSA) reported that prescription drugs are the second most popular category of recreational drugs (just behind marijuana). Surveys of recovery groups in 2002 revealed that fifty-four percent of addicts reported obtaining narcotics by manipulating their dentist. Always keep prescription pads in a locked place to limit access for patients. It is further recommended not to print the dentist's Drug Enforcement Agency (DEA) number on the prescription pad.16
Xerostomia: The vasoconstriction of the salivary glands, along with the drying agents in MA, leaves the oral mucosa severely dry. Upon examination, patients with xerostomia may complain of generalized mouth soreness, dry mouth, painful or burning tongue, taste changes, difficulty in chewing, and problems with talking and swallowing. Clinical presentation of xerostomia includes oral fissuring, ulceration, and epithelial atrophy. Saliva substitutes and moisturizers can reduce some symptoms. Encourage patients to drink water rather than quenching their thirst with sodas, sports drinks, or fruit juices that contain sugar. Without saliva to buffer the acid attacks, decay can happen quickly and extensively. Preventive fluoride treatments both in-office and at home are strongly recommended to strengthen and remineralize the damaged enamel rods. Recommend the use of xylitol products to reduce the development of caries, resist the fermentation of bacteria, reduce plaque formation and increase salivary flow.17
Decay: Patients may report that their tooth decayed "from the inside out." (Figure 6) A possible explanation may be because there is reduced blood supply to the tooth. With repeated vasoconstriction, the vessels won't recover and without nutrients to the tooth, it will die. Treating a carious lesion with conventional means is of little value with a patient who is using MA. The disease will reoccur under the restorative material. Sealing the area with fluoride and xylitol releasing fluoride varnish and/or glass ionomer sealant & surface protectant are treatment modalities that may be of benefit until the patient stops drug use. Dr. Hill reported using both acrylic and composite temporary crowns with great success. Intermediate restorative material (IRM) aids in relieving pain and serves as a temporary solution. IRM is easy to use and its strength properties approach that of zinc phosphate cement, it has good sealing properties, low solubilities and excellent abrasion resistance with grinding.
Mitchell Goodin, DDS, of Eldorado, California, treats hundreds of MA patients a year. He has made it his mission to educate dental professionals, youth and "anyone who will listen."20 His experience has shown that most MA users end up losing their teeth. He suggested "comfort care" until it is time for extractions and dentures.
Periodontal Disease: Meth users do not generally seek regular dental treatment. When they do, they will often present with gingivitis (bleeding, inflamed gingival tissue) or periodontitis (bone loss) from lack of professional oral care and inadequate home care. Patient education on plaque control, nutrition and the etiology of disease can help the patient maintain the area until they are ready for treatment. Nutritional deficiencies need to be addressed to aid in healing of tissue after treatment. Dr. Hill suggested the use of alcohol free chlorhexidine until treatment can take place.
Oral mucosa: Oral mucosa wounds, angular cheilitis, mucositis, and candida albicans (oral thrush) are the results of a compromised immune response coupled with exposure to a dry, acidic environment. Having the patient swish with a mixture of Kaopectate® and Benadryl® mixed at a fifty-fifty percentage will aid in healing and give relief from pain. Evaluate the patient for the presence of candida albicans. For oral candidiasis prescribe either Nystatin® suspensions or clotrimazole troches which are both extremely effective treatment.18
Tweakers: All offices need to have a protocol for the tweaker patient. People who abuse Meth regularly are known as ‘tweakers'. Tweakers often behave or react violently. Keep in mind, the tweaker may not have slept in three to fifteen days and may be irritable and paranoid. If the tweaker is also using alcohol or other drugs, the danger may be intensified and a distance should be maintained.
The tweaker craves more Meth, but no dosage will help recreate the first rush. This may cause frustration and lead to unpredictable behavior and violence. To support their habits, tweakers often participate in spur-of-the-moment crimes, such as purse snatching or burglaries. Tweakers are often involved in domestic disputes and automobile accidents. They may also be present at raves or parties. They may at first appear to be normal. A closer look will reveal eye movement ten times faster than normal, a voice with a slight quiver and jerky movements.15 Table 9 offers information in dealing with a tweaking MA user. Dental professionals are mandated reporters. If abuse or neglect is occurring as a result of MA use, dental professionals are mandated to report it to the proper authorities.
Summary
Methamphetamine abuse is on the rise. It is an extremely serious, addicting drug that affects all aspect of patient life and health. The supplies to make MA are under watch to aid in the decrease in production. Research is being conducted to help addicts recover brain function in a healthy way. Altered brain function, rampant caries, xerostomia, and rapidly deteriorating appearance are a few noticeable signs of chronic MA abuse. Understanding the disease process, treatment strategies, and drug abuse referral systems can lead to appropriate intervention and ensure proper treatment, patient education and prevention of disease progression.
Glossary
Angular cheilitis - skin lesions on the lips and particularly as breaks of tissue in the corners of the lips. It is caused by parasitic fungus, vitamin B deficiency, compromised immune system and vasoconstriction of the tissue.
Anorexia - an eating disorder in which people do not eat correctly due to distorted body image and obsessive fear of weight gain, or the general symptom of decreased appetite.
Anti-inflammatory - the property of a substance or treatment that reduces inflammation. Anti- inflammatory drugs make up one half of analgesics, remedying pain by reducing inflammation as opposed to opioids, which affect the brain.
Candida albicans - diploid asexual fungus (a form of yeast), and a causal agent of opportunistic oral and vaginal infections in humans.
Central nervous system - (CNS) represents the largest part of the nervous system, including the brain and the spinal cord. Together with the peripheral nervous system, it has a fundamental role in the control of behavior.
Clotrimazole troches - an anti-fungal medication, held in the mouth until dissolved.
Cocaine - a crystalline tropane alkaloid that is obtained from the leaves of the coca plant. It is a stimulant of the central nervous system and an appetite suppressant, giving rise to what has been described as a euphoric sense of happiness and increased energy. It is most often used recreationally for this effect. Cocaine is formally used in medicine as a topical anesthetic, specifically in eye, nose and throat surgery.
Ephedrine - alkaloids from the ephedra plant that are used to treat low blood pressure, asthma and weight loss. It is also considered a performance enhancing drug. Ephedra is a stimulant and thermogenic. It can stimulate the brain, increase the heart rate, constrict blood vessels, and bronchial tubes. Their thermogenic properties can cause an increase in metabolism evidenced by an increase in body heat.
Fight or flight syndrome - the fight-or-flight response, also called the acute stress response. Animals react to threats with a general discharge of the sympathetic nervous system, priming the animal for fighting or fleeing.
Formication/ meth bugs - constriction of blood vessels due to the intake of MA that leads to intense itching and the feeling that there are bugs crawling under the skin.
Glossitis - inflammation or infection of the tongue. It causes the tongue to swell and change color. Finger- like projections on the surface of the tongue (papillae) may be lost, causing the tongue to appear smooth.
Hyperthermia - an acute condition that occurs when the body produces more heat than it can dissipate. Heat regulating mechanisms of the body eventually become overwhelmed and unable to effectively deal with heat and body temperature climbs uncontrollably. This is a serious medical emergency that requires immediate medical attention. It can be brought on by the use of drugs.
Methamphetamine - (MA) a psycho stimulant drug that is very addictive, activating certain systems in the brain. It is chemically related to amphetamine but, at comparable doses, the effects of methamphetamine are much more potent, longer lasting, and more harmful to the central nervous system.
Meth mouth - an informal name for the advanced tooth decay and oral disease seen in methamphetamine users. It is caused by the combination of vasoconstriction, poor oral care, xerostomia, grinding, clenching, and high intake of sugary drinks. The pattern of decay is distinctive in that, initially, it involves the smooth buccal surface of posterior teeth and the interproximal of the anterior teeth.
Narcolepsy - narcolepsy is a neurological condition characterized by Excessive Daytime Sleepiness (EDS). A narcoleptic will most likely experience disturbed nocturnal sleep, confused with insomnia, and disorder of rapid eye movement sleep.
Neurotoxic - occurs when the exposure to natural or manmade toxic substances, which are called neurotoxins, alters the normal activity of the nervous system. This can eventually disrupt or even kill neurons, key cells that transmit and process signals in the brain and other parts of the nervous system. Symptoms may appear immediately after exposure or be delayed. They may include limb weakness or numbness, loss of memory, vision, and/or intellect, headache, cognitive and behavioral problems and sexual dysfunction. Individuals with certain disorders may be especially vulnerable to neurotoxins.
Neurotransmitters - any one of numerous chemicals that modify or result in transmission of nerve impulses between synapses.
OTC - acronym for "over the counter" medications.
Psychomotor stimulant - causes voluntary movement usually associated with neural activity.
Parkinson's Disease - degenerative disorder of the central nervous system that impairs motor skills and speech. It is characterized by muscle rigidity, tremor, slowing of physical movement (bradykinesia) and in extreme cases, a loss of physical movement (akinesia).
Shake and bake, or one-pot - cooking method that is a variation of the lithium ammonia method of production. Instead of producing methamphetamine through a series of sequential steps normally used the one-pot method is concluded in a single reaction vessel (typically a 2-liter plastic soda bottle). All ingredients are mixed together at the outset. The mixture is left to react, naturally producing the necessary ammonia, which then reacts with the lithium metal to convert the pseudoephedrine into methamphetamine. Like all clandestine methamphetamine production operations, the one-pot method is dangerous because the reactions are volatile and difficult to control.
Striatum - a subcortical part of the forebrain, the major input stations of the basal ganglia which control functions such as voluntary motor control and learning.
Synapse - the space between an axon and dendrite (two neurons) where a neurotransmission takes place.
Synaptic terminal - a bulb at the end of an axon in which neurotransmitter molecules are stored and released to the receiving dendrite.
Tweaking - slang term for someone exhibiting pronounced symptoms and MA use. This includes repetitive performance of useless tasks, hyperactivity, an inhibited ability to relate socially, lack of appetite, inattention to body hygiene, exaggerated fidgeting, formication and psychosis. Due to psychosis the patient may act irrationally or violently.
Trismus - pathologic condition in which the muscles of the jaws contract for long periods of time.
Vasoconstrictor - a substance such as ice or drugs that causes a narrowing of blood vessels and decreased blood flow; may result in an increase in blood pressure and eventual tissue damage.
Xerostomia - dry mouth due to lack of saliva. Can cause difficulty in speech and eating. It also leads to halitosis and a dramatic rise in the number of carious lesions, as the protective effects of saliva are no longer present and can make the mucosa more vulnerable to infection. Xerostomia is one of the major factors in the condition Meth Mouth.
References
1. Colfax, G. N. (2005). Methamphetamine-The Scope of the Problem, Medscape HIV/AIDS, 11(2)
2. Albertson, T. E. et al. (1999, April). Methamphetamine and the Expanding Complications of Amphetamines, WJM, 170(4), 214-219
3. Curtis, E.K. (2006, Mar-Apr). Meth Mouth; A Review of Methamphetamine Abuse and its Oral Manifestations, Gen Dent. 54 125-129
4. Derlet, R. W., Heischober, B., (1990, Dec). Methamphetamine: Stimulant of the 1990s?, WJM 153(6) 625-627
5. Daberkow, D.P., Kesner R.P. Keefe K.A., (2005, May). Relationship Between Methamphetamine-Induced Monoamine Depletions in the Striatum and Sequential Motor Learning, Pharmacol Bio Chem Behavior, 81(1).198-204
6. Prah, O.P.H. (2005, July). Methamphetamines: Are Tougher Anti-Meth Laws needed? CQ Researcher, 15, 589-612
7. Boddiger, D. (2005). Methamphetamine Linked to Rising HIV Transmission. Lancet .365, 1217-1218
8. National Institute on Drug Abuse, InfoFacts: Methamphetamine (Rockville, MD: US Department of Health and Human Services), from the web at http://www.nida.nih.gov/infofacts/methamphetamine.html last accessed Nov, 9, 2006
9. Zweben, J., et al. (2005). Methamphetamine Treatment Project, Psychiatric Symptoms Methamphetamine Users. AM J Addict, 13, 181-190
10. Diago, Steven, (2003, Dec). When Your Patient is an Addict. AGD Impact, 33(9)
11. Shaner, J.W. Meth Mouth and Rampant Caries in Meth Abusers, APC, 20(3) 146-150
12. De Cugno, F., et.al, (1981). Salivary Secretion and Dental Caries Experience in Drug Addicts. Arch Oral Bio. 26, 363-367
13. Murphy D., Wilmer, S., (2002). Patients Who are Substance Abusers. NYDent J., 68, 24-27
14. Eyalka, T., (2005). Rural America's Epidemic Destroying Patients' Teeth, Ill Dental News, 74, 4-5
15. http://www.mappsd.org/Treatment.htm, Accessed 10/11/2006
16. http://www.samhsa.gov/ accessed 10/11/2006
17. Creanor S.L., Strang R., Gilmour W., et al. (1992). The Effect of Chewing Gum Use on In-situ Enamel Lesion Remineralization. J Dent Res 71, 1895-1900
18. Jose A. Vazquez, (1999). Options for the Management of Mucosal Candidiasis in Patients With AIDS and HIV Infection Pharmacotherapy © Pharmacotherapy Publications, 19(1) 76-87
19. American Dental Association update. August 1, 2007
20. Personal interview with Dr. James Hill DDS 11/03/2006 conducted by Noel Kelsch, RDH
21. Personal interview with Dr. Mitchell Goodin 11/6/2006 conducted by Noel Kelsch, RDH
22. http://www.tricities.com/news/2011/sep/25/battling-meth-epidemic-ar-1334775/. Accessed November 16, 2011.
23. University of Washington (2008, April 9). Methamphetamine Addiction Mechanism Discovered, Explains Why Cravings Last So Long. Science Daily. Retrieved November 16,2011: http://www.sciencedaily.com/releases/2008/04/080409120619.htm
24. http://drugabuse.gov/infofacts/methamphetamine.html.Accessed December 8, 2011.
25. http://www.myaddiction.com/education/articles/meth_statistics.html. Accessed December 8, 2011
26. Center for Behavioral Health Statistics and Quality. (2016). Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health (HHS Publication No. SMA 16-4984, NSDUH Series H-51). Retrieved from http://www.samhsa.gov/data/
27. NIDA. (2013, September 19). Methamphetamine. Retrieved from https://www.drugabuse.gov/publications/research-reports/methamphetamine on 2017, October 23
About the Author
Noel Brandon-Kelsch, RDH
Noel Brandon-Kelsch is an international speaker, writer and Registered Dental Hygienist in Alternative Practice. She reaches clients by taking a backpack out on the street and delivering preventive tools. Her 20 years of service to clients experiencing the effects of methamphetamine abuse have led her to spread the message of hope and prevention to all health care professionals. She is passionate about oral health and has the uncanny ability to motivate and enlighten audiences through her unique humor and cutting-edge information. She takes tough subject matter and presents it in such an interesting way that it becomes thought provoking even to those not involved in her industry. She is the infection control columnist for RDH magazine, a syndicated newspaper columnist, has been published in many books. She has brought the message of oral health to media networks from Disney Radio to ESPN. Noel has received many national awards including Colgate Bright Smiles Bright Futures, RDH Magazine Sun Star Butler Award of Distinction, USA magazine Make a Difference Day Award, President's Service Award, Foster Parent of the Year, Hu-Friedy Master Clinician Award.
Resources for Rehabilitation
It is important for the dental office to be equipped with resources to refer the patient to the proper health care professional for treating drug addiction.
Having a list of area resources will help in delivering care. Health departments and social service agencies can aid in gathering this information (Table 8 and Table 9).