You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Musculoskeletal disorders (MSDs) are usually defined as injuries to the soft and hard tissues of the body, and may occur after a single event or due to cumulative trauma.1 Work related MSDs are considered a global health and financial burden, costing millions of dollars annually.2,3 For example, in Australia, work related MSDs were reported in over 76,000 workers’ compensation claims.4 Reduced work hours and increased sick leave are a significant burden not only for the individual, but also on the economy.
Research has demonstrated that MSDs are a significant occupational health issue for the dental profession, especially for dentists and dental hygienists.5-7 A number of unique risk factors have been documented among these professionals, including a limited working field, static postures, fine movements and repetitive tasks. A recent review, for example, identified that over half of dental hygienists report MSDs in any body region.7 More specifically, MSDs in the neck, shoulder, wrist/hand and lower back regions is frequently reported across a number of studies.8-11 Despite this fact, there is a distinct lack of evidence regarding the efficacy of preventive measures for MSDs in the dental hygiene profession.
In recent years, there is mounting evidence that undergraduate students are burdened by MSDs.12 In particular, health sciences students have been identified as suffering MSDs at considerable rates.13-15 Computer usage and desk based study have been shown to increase the report of MSDs among cohorts of university students, while psychosocial stress has been suggested as another possible risk factor.14,16-19 Despite this fact, a surprising lack of research has investigated MSDs among dental hygiene student populations.
Dental hygiene is a rapidly growing profession in Australia, as elsewhere, with a number of new baccalaureate programs established within the last decade. Dental hygiene education and training in Australia involves the completion of a 2 year advanced diploma or a 3 year bachelor’s degree program. Given that dental hygiene students are undergraduate students working towards a career that has a high incidence of MSDs, it is of great concern that this particular group may be at an increased risk of developing MSDs.
The focus of the current study was to collect epidemiological data, such as the prevalence, and determine predictors of MSDs over a period of time to allow insight into patterns and trends of risky behaviors or disease. Ascertaining patterns of MSDs among dental hygiene students is essential for employing sound ergonomic principles in the dental hygiene curriculum, as well as influencing how and when preventive strategies should be employed to best effect. As such, the aim of the present study was to determine the longitudinal MSD trends in a cohort of dental hygiene students at an Australian University, across the 3 years of their education and training.
Methods and Materials
This study was carried out as descriptive and exploratory research, using a longitudinal approach. It is an extension of a cross-sectional study that was completed in 2008. As such, the methodology has been published in detail elsewhere.14 An institutional review board approval to collect data over a 3 year period was sought and obtained from the University of Newcastle Human Research and Ethics Committee. All dental hygiene students commencing the Bachelor of Oral Health at the University of Newcastle in 2008 (n=75) were invited to participate in this study. For 3 consecutive years, in the first week of semester 2, students were approached during a scheduled lecture or clinical session and invited to participate in the study. They were invited by a staff member not involved with the research project, and were clearly advised that there were no penalties or rewards for participation. An anonymous, 2 page modified version of the Standardized Nordic Questionnaire was completed by students agreeing to participate.20 This questionnaire is a valid tool that has demonstrated a high level of reliability (k=0.73 to 0.82) and sensitivity (0.9 to 1.0).21 Completing the survey involved answering 17 tickbox questions, covering items such as age, gender, weekly clinical hours, regular exercise and study habits. Participants were asked to indicate whether they had experienced any ache, pain or discomfort in specific body regions in the previous 12 months, whether it lasted longer than 2 days, affected their daily life or required medical attention. An anatomical diagram was included to aid participants in identifying various regions of the body. The survey has been used among a variety of health science student groups in various countries.15,16,22-24
All data collected was entered into a spreadsheet and analyzed using the STATA statistical software package. Descriptive statistics were calculated, with direct logistic regression performed to elucidate potential risk factors for MSD.
Results
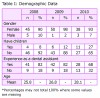
Across the 3 years, response rates ranged from 54 to 68%. From a cohort of 75 students commencing in 2008, 50 students participated in the first year (2008), 51 students in the second year (2009) and 41 students in their final year of study (2010). Demographic data is presented in Table 1. The cohort was predominately female non-smokers, who had prior experience working as a dental assistant.
The 12 month prevalence of MSDs by body region for the 3 year period between 2008 to 2010 is presented in Table 2. Neck pain was the most commonly reported MSD, and its prevalence rate increased steadily over the 3 year period (the prevalence rates ranging from 66% in 2008, to 68.3% in 2010). Lower back pain was also commonly reported by students, with the results showing a noticeable increase in the final year of study (rising from 60.8% in 2009, to 68.3% in 2010). Wrist/hand pain was reported by over one-third of respondents in the first year of study; however, this increased noticeably in the second year, and even further in the final year (34%, 41.2% and 43.9%, respectively). The prevalence of upper back pain lasting longer than 2 days (22%, 27.5%, 34.1%) increased steadily across the 3 years of training, while pain lasting longer than 2 days in the neck, shoulders and wrist/hand regions peaked in the second year of study.
All students who reported feelings of extreme stress associated with the clinical requirements of the dental hygiene course indicated that they had experienced pain in the neck, shoulder, upper back and lower back, a finding that was consistent for all 3 years of the study. Logistic regression analysis did not elucidate any statistically significant correlations between year of study, number of clinic hours or prior experience as a dental assistant with MSD.
A comparison of 12 month prevalence of MSDs in the neck, shoulder, wrist/hand and lower back regions among student cohorts is displayed in Table 3. All studies utilized the Standardised Nordic questionnaire anatomical diagram for investigating the 12 month prevalence of MSD.
Discussion
This study investigated the prevalence of MSDs among a group of dental hygiene students, over the 3 year duration of their education and training program. The results suggest that MSD is a common problem, in particular at the neck, shoulder, wrist/hand and lower back regions, which were reported frequently across the 3 years from 2008 to 2010. The cohort of students in this study closely resembles those in other studies of dental hygiene students, which were also predominantly female with an average age in the mid-twenties.25,26 A study from the U.S. found that second year dental hygiene students were more likely to report any MSD (70%) than their first year counterparts (62%).26
Compared with students undertaking other health science studies, dental hygiene students appear to suffer from MSDs at considerably higher rates.14,16,22,27,28 A comparison of 12 month prevalence of MSD in the neck, shoulder, wrist/hand and lower back regions among student cohorts suggests that dental hygiene students are more likely to suffer from wrist/hand pain and lower back pain than other health science students. Clinical tasks carried out by hygiene students are very repetitive and require static postures - these risk factors may not be as common for other health sciences students, which may explain the differences in reported MSD rates. Perhaps the most comparable group to dental hygiene students are occupational therapy students, whose reports of neck and shoulder pain appear to be related more to computer usage and increasing age rather than occupational risks.16 Higher prevalence rates documented in the current study may also be influenced by the relatively high proportion of females in dental hygiene cohorts, given that previous research has indicated that females are more likely to report MSDs than their male counterparts.29
It is interesting that the current study did not find any statistically significant correlations between MSDs and previous experience as a dental assistant, number of clinical hours or year of study. Previous research among dental hygiene students suggests that those with a dental assisting background self-reported neck and shoulder pain more than their inexperienced student counterparts.30 Furthermore, studies of nursing students in both Australia and Japan have found an association between reported MSD and previous experience working in a hospital.22,31 It may be that as the clinical requirements of the course increase, students spent less hours working in paid employment - this may have minimized the effect of dental assisting on reported MSD. Practicing dental professionals may be at an increased risk of developing MSD over time, with a study of Swedish dentists, hygienists and assistants reporting increased pain levels after 5 years when compared to baseline measures.8
A number of studies have also reported increasing age to be correlated with increased MSD symptoms, in both student groups14 and practicing hygienists.10,32,33 It may be that a combination of factors, such as increased time practicing in clinical settings and one’s natural increase in age, contributes to MSD, however, neither correlated individually with reported MSD in the current study.
Based on the findings of the current and previous studies, it is important that dental hygiene students undertake comprehensive occupational health and ergonomics modules during their education and training. Contemporary research has found that among practicing hygienists, education on patient and operator positioning can help reduce the risk of MSD.34 Despite this fact, there is limited research published on this topic.35 Future studies should investigate the educational component of ergonomics in the curriculum, along with the expertise of faculty in this area.
The results of this study are concerning for a group yet to embark on their professional careers, and this raises some serious questions about career longevity and the efficacy of preventive measures. Further investigations into the epidemiological patterns of MSD among larger cohorts of dental hygiene students are necessary. Also, longitudinal studies following students into their employment would also be extremely valuable. It has also been established elsewhere that there is very limited research investigating the effectiveness of preventions or interventions for MSD.7
The present study required careful design to ensure that the students invited to participate did not feel as though they were coerced, or that there was any perceived benefit or disadvantage to their education if they chose to participate. As such, the privacy and anonymity of the students was vital, and for this reason the follow-up of individual students was not possible. Another perceived limitation of the study may be the use of a self-reporting survey, as possible response bias may limit the generalizability of the results. However, while there is a plethora of research involving MSD, little research has investigated this occupational health issues among dental hygiene students. Given that this study appears to be the first to follow a cohort of dental hygiene students across their 3 years of training, the findings are nevertheless valuable, adding to the small body of research and facilitating an increasing understanding of MSD in our profession.
Conclusion
The results of this study provide valuable insight into the epidemiological patterns of this occupational health issue. Dental hygiene students are reporting MSDs at considerably higher rates than students in other health science disciplines. What continues to remain unclear is the risk factors involved and, therefore, how to instigate appropriate preventive strategies.
Melanie J. Hayes, BOH, BHSc(Hons), PhD, is an Oral Health Lecturer; Derek R. Smith, BSc, BEd, MHSc, MPH, PhD, DrMedSc, is Professor of Environmental and Occupational Health; Jane A. Taylor, BDS, BScDent (Hons), MScDent, PhD, is Associate Professor and Program Convenor of Oral Health. All are at the Faculty of Health at the University of Newcastle, NSW, Australia.
References
1. Graham C. Ergonomics in dentistry, Part 1. Dent Today. 2002;21(4):98-103.
2. Hanson M, Burton K, Kendall N, Lancaster R, Pilkington A. The costs and benefits of active case management and rehabilitation for musculoskeletal disorders. Prepared by Hu-tech Associates Ltd for the Health and Safety Executive, 2006.
3. United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States, Second Edition. Rosemont, IL: American Academy of Orthopaedic Surgeons [Internet]; 2011.
4. Work-related musculoskeletal disease in Australia. Australian Safety and Compensation Council [Internet]. 2006. Available from: http://www.safeworkaustralia.gov.au/sites/SWA/about/Publications/Documents/119/WorkRelatedMusculoskeltalDisorders_2006Australia_2006_ArchivePDF.pdf.
5. Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009;7(3):159-165.
6. Puriene A, Janulyte V, Musteikyte M, Bendinskaite R. General health of dentists. Literature review. Stomatologija. 2007;9(1):10-20.
7. Hayes MJ, Smith DR, Cockrell D. An international review of musculoskeletal disorders in the dental hygiene profession. Int Dent J. 2010;60(5):343-352.
8. Akesson I, Johnsson B, Rylander L, Moritz U, Skerfving S. Musculoskeletal disorders among female dental personnel--clinical examination and a 5-year follow-up study of symptoms. Int Arch Occup Environ Health. 1999;72(6):395-403.
9. Anton D, Rosecrance J, Merlino L, Cook T. Prevalence of musculoskeletal symptoms and carpal tunnel syndrome among dental hygienists. Am J Ind Med. 2002;42(3):248-257.
10. Liss GM, Jesin E, Kusiak RA, White P. Musculoskeletal problems among Ontario dental hygienists. Am J Ind Med. 1995;28(4):521-540.
11. Ylipaa V, Arnetz BB, Preber H. Predictors of good general health, well-being, and musculoskeletal disorders in Swedish dental hygienists. Acta Odontol Scand. 1999;57(5):277-282.
12. Smith DR, Leggat PA. Back pain in the young: A review of studies conducted among children and university students. Curr Pediatr Rev. 2007;3(1):69-77.
13. Leggat PA, Smith DR, Clark MJ. Prevalence and correlates of low back pain among occupational therapy students in Northern Queensland. Can J Occup Ther. 2008;75(1):35-41.
14. Hayes MJ, Smith DR, Cockrell D. Prevalence and correlates of musculoskeletal disorders among Australian dental hygiene students. Int J Dent Hyg. 2009;7(3):176-181.
15. Nyland LJ, Grimmer KA. Is undergraduate physiotherapy study a risk factor for low back pain? A prevalence study of LBP in physiotherapy students. BMC Musculoskelet Disord. 2003;4:22.
16. Smith DR, Leggat PA, Clark MJ. Upper body musculoskeletal disorders among Australian occupational therapy students. Brit J Occup Ther. 2006;69(8):365-372.
17. Warren N. Causes of musculoskeletal disorders in dental hygienists and dental hygiene students: A study of combined biomechanical and psychosocial risk factors. Work. 2010;35(4):441-454.
18. Sanders MJ, Turcotte CM. Occupational stress in dental hygienists. Work. 2010;35(4):455-465.
19. Smith DR, Wei N, Ishitake T, Wang RS. Musculsoskeletal disorders among Chinese medical students. Kurume Med J. 2005;52(4):139-146.
20. Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233-237.
21. Palmer K, Smith G, Kellingray S, Cooper C. Repeatability and validity of an upper limb and neck discomfort questionnaire: the utility of the standardized Nordic questionnaire. Occup Med. 1999;49(3):171-175.
22. Smith DR, Leggat PA. Musculoskeletal disorders among rural Australian nursing students. Aust J Rural Health. 2004;12(6):241-245.
23. Smith DR, Leggat PA. Prevalence and distribution of musculoskeletal complaints among medical students. J Musc Pain. 2007;15(4):39-46.
24. Smith DR, Choe MA, Jeon MY, Chae JR, An GJ, Jeong JS. Epidemiology of musculoskeletal symptoms among Korean hospital nurses. Int J Occup Saf Ergon. 2005;11(4):431-440.
25. Werner RA, Franzblau A, Gell N, et al. Prevalence of upper extremity symptoms and disorders among dental and dental hygiene students. J Calif Dent Assoc. 2005;33(2):123-131.
26. Morse TF, Michalak-Turcotte C, Atwood-Sanders M, et al. A pilot study of hand and arm musculoskeletal disorders in dental hygiene students. J Dent Hyg. 2003;77(3):173-179.
27. Smith DR, Choe MA, Chae YR, Jeong JS, Jeon MY, An GJ. Musculoskeletal symptoms among Korean nursing students. Contemp Nurse. 2005;19(1-2):151-160.
28. Lorusso A, Vimercati L, L’Abbate N. Musculoskeletal complaints among Italian X-ray technology students: a cross-sectional questionnaire survey. BMC Res Notes. 2010;3:114.
29. Rolander B, Bellner AL. Experience of musculo-skeletal disorders, intensity of pain, and general conditions in work -- the case of employees in non-private dental clinics in a county in southern Sweden. Work. 2001;17(1):65-73.
30. Morse T, Bruneau H, Michalak-Turcotte C, et al. Musculoskeletal disorders of the neck and shoulder in dental hygienists and dental hygiene students. J Dent Hyg. 2007;81(1):10.
31. Smith DR, Mihashi M, Adachi Y, Koga H, Ishtake T. A detailed analysis of musculoskeletal disorder risk factors among Japanese nurses. J Safety Res. 2006;37(2):195-200.
32. Shenkar O, Mann J, Shevach A, Ever-Hadani P, Weiss P. Prevalence and risk factors of upper extremity cumulative trauma disorder in dental hygienists. Work. 1998;11(3):263-75.
33. Ylipaa V, Szuster F, Spencer J, Preber H, Benko SS, Arnetz BB. Health, mental well-being, and musculoskeletal disorders: a comparison between Swedish and Australian dental hygienists. J Dent Hyg. 2002;76(1):47-58.
34. Hayes MJ, Taylor JA, Smith DR. Predictors of work-related musculoskeletal disorders among dental hygienists. Int J Dent Hyg. 2012;10(4):265-269.
35. Beach JC, DeBiase CB. Assessment of ergonomic education in dental hygiene curricula. J Dent Educ. 1998;62(6):421-425.