You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
One of the more desirable goals for CAD/CAM restorations is to make them unnoticeable in the mouth. In popular discourse, CAD/CAM restorations are often portrayed as unesthetic, unnatural looking, or too similar to temporary restorations. These criticisms ignore the reality that CAD/CAM restorations can appear to be natural if the clinician devotes a sufficient amount of effort to their creation.1
Recommendations for Posterior CAD/CAM Restorations
Accentuate Anatomy
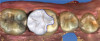
The quality of CAD/CAM restorations is directly correlated with the amount of work dedicated to their manufacture. This principle is exemplified in Figure 1 and Figure 2. The restoration in Figure 2 looks more natural than the one depicted in Figure 1. With sealed margins and correct function in the mouth, both restorations are clinically acceptable; however, the one in Figure 2 is much more esthetic. It has more subtle anatomical details as well as some staining in the grooves to help it blend in with neighboring teeth. The restoration in Figure 1 is an example of how CAD/CAM crowns appear when they are used right from the milling unit without further modification. The restoration in Figure 2 involved the same initial milling process, but a few extra minutes were taken to accentuate the anatomy with an inverted cone diamond bur. The clinician can use the end-cutting bur to scribe anatomy on the occlusal surface of the crown wherever deemed appropriate. Scribing anatomy creates a place for stains to settle after firing, ensuring a more natural look.
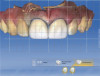
In a similar case involving an onlay (Figure 3 and Figure 4), the clinician scribed anatomy that resulted in the appearance of natural stains. Figure 3 shows the scan that was taken being displayed on a CAD/CAM system; Figure 4 shows the final restoration bonded into place.
Figure 5 provides further elucidation of this critical finishing step. Many clinicians who observe this image conclude that teeth Nos. 13, 14, and 15 are crowns, when in fact, they are not. There is actually a bridge, which gives the impression of separate restorations. An appropriate instrument for this situation is a fine, needle-shaped diamond bur. After the restoration is milled, the dentist can create anatomy on the buccal surface, define embrasure spaces further, define connector spaces, and use an endodontic file with some stains to accentuate the interproximal surface of the connectors. This process creates the illusion of separate teeth.
As demonstrated by these examples, the first recommendation for making posterior CAD/ CAM restorations look more natural is to accentuate the anatomy on the occlusal and buccal surfaces after the crown is milled. In most instances, this will significantly enhance the final outcome.
Hybrids Are Optimal
Figure 6 displays a case with a two-surface inlay on an upper first molar. After a failing amalgam restoration was cleaned up and the tooth was prepared for the two-surface inlay design, the clinician used a hybrid material to mill the restoration. Because the hybrid material blends more effectively into the surrounding tooth structure2 when bonded, the cavosurface margin between the restoration and tooth surface is mostly hidden.
Similarly, the case depicted in Figure 7 involved placing a hybrid onlay on an upper first molar. After the dry fitting, bonding, and polishing, the surface between the restoration and the tooth was barely visible.
Improving Translucency
The next recommendation concerns translucency. Figure 8 shows a case restored with several "crownlays"; they were intentionally finished to be difficult to recognize. The clinician placed crownlays on teeth Nos. 3 and 4 and positioned the finishing line above the height of contour. For this type of case, it is often best to use high-translucency blocks and make a rollercoaster margin to help the restoration blend in.
In a case that was completed before the clinician had become involved with CAD/CAM, a laboratory-made porcelain-fused-to-metal (PFM) crown was placed. Several years later, the patient returned to the dentist, unhappy with the appearance of the crown (Figure 9). The clinician offered to change the crown at no cost. Although the initial result was clinically acceptable, esthetically, it was not exemplary. The dark margin was exposed, the finishing line was above the gum line, and the final shade of the restoration did not match the adjacent teeth. For the new restoration, the clinician used a glass-ceramic crown. When doing a full-coverage crown that is required to block a dark stump, a low translucency material is preferred. The clinician also spent time staining and glazing the restoration to more closely mimic the neighboring teeth. For posterior restorations, the translucency of the material plays a large role in the final outcome. High translucency materials are preferred for partial coverage restorations, and low translucency materials are preferred for full-coverage restorations.3-5
Staining Enhances Esthetics
Figure 10 depicts a crown that was placed on tooth No. 4. Preoperatively, an existing silver amalgam filling with recurrent decay had been visible, so the decision was made to convert it to a crown. The clinician used some staining and glazing to help mimic the neighboring teeth. The aforementioned case in Figure 5 also provides an example of the power of staining, demonstrating how a bridge can be made to look more like individual teeth using stains placed between the connectors.
In another case involving a failing amalgam restoration (ie, tooth No. 30), there was still some healthy tooth structure present on the mesial surface (Figure 11). The tooth was prepared, and an onlay was planned and placed (Figure 12 through Figure 14). Some occlusal cavosurface margin was visible. It is clear from these images that, beyond choosing an appropriate restorative material, performing a small amount of staining and glazing enabled the clinician to blend the restoration with the neighboring teeth. Therefore, the final recommendation for posterior CAD/CAM restorations is that subtle staining can greatly enhance the esthetics of outcomes.6
Recommendations for Anterior CAD/CAM Restorations
Keep the Midline Straight
For anterior restorations, the midline is critical. Figure 15 and Figure 16 show two different cases in which tooth No. 9 was restored. For the case in Figure 15, the clinician placed a veneer on tooth No. 9. For the case in Figure 16, the clinician converted a large composite filling, which was staining and chipping, into a veneer. In Figure 15, the midline is canted, whereas in Figure 16, the midline is straight, making it look more natural by comparison. With anterior restorations, it is very important to avoid creating a canted midline.7 The most important recommendation is to pay attention to the midline's straightness. Within a CAD/CAM system, using a grid while treatment planning can help clinicians set the midline straight.
Achieve Symmetrical Centrals
A second recommendation for anterior restorations relates to the cases shown in Figure 17 and Figure 18. In both cases, the clinician restored teeth Nos. 8 and 9. For the case in Figure 17, veneers were placed; for the case in Figure 18, crowns were placed. The case depicted in Figure 18 looks better esthetically because the centrals in Figure 17 are not symmetrical. For the case in Figure 18, tooth No. 8 was somewhat overlapped onto tooth No. 9, which lead to a perfectly symmetrical result. When working on anterior teeth, it is important to make the centrals symmetrical.8,9 With a straight midline and symmetrical centrals, the case in Figure 18 looks more esthetically pleasing when compared to a case with a canted midline and asymmetrical centrals. Because the centrals are symmetrical, other less than optimal aspects of the case are less noticeable. For example, the gingival zenith of tooth No. 11 was pointier than that of tooth No. 6, and the width of tooth No. 7 was greater than that of tooth No. 8. These discrepancies are less integral in the presence of a straight midline and symmetrical centrals.
Respect Contact Length/Gingival Height Ratio
Figure 19 and Figure 20 show two separate cases in which teeth Nos. 8 and 9 were restored with full-coverage crowns. The result shown in Figure 19 is more esthetic than the one shown in Figure 20. In Figure 19, the lines go from the gingival zenith to the height of the papilla and from the height of the papilla to the contact length. These lengths are relatively equal. As a result, the contact length does not appear too long. In Figure 20, the height/length ratio of the papilla is approximately 60:40 or 70:30. The optimal height/length ratio of the papilla is 50:50.10,11 The case in Figure 20 involved a longtime patient of the clinician's practice who had orthodontic work performed. She was young and unhappy with the discoloration of tooth No. 8. In addition, she was unhappy with the overlap of tooth No. 9 over tooth No. 10 and was unwilling to endure further orthodontic procedures. Root canals had been previously performed on both teeth Nos. 8 and 9. To address these issues, the clinician decided to put crowns on the teeth with a CAD/CAM system. Although there was a 50/50 ratio at the outset, by the time the case was finished, the ratio was skewed. While designing the crowns, the clinician made a mistake, and the contact length was closed up slightly more than it should have been, which made it appear much taller than it was initially.
This mistake can be avoided. Figure 21 presents a similar case in which the patient had a skiing accident and needed root canals for teeth Nos. 8 and 9. When the clinician was designing the restorations with the CAD/CAM system, an initial scan of the teeth was taken, which showed the original position of the gingiva prior to any reduction of the teeth or cord packing. The clinician prepared both teeth for crowns and finished the design (Figure 22). Looking carefully, an open black triangle can be seen between teeth Nos. 8 and 9. When designing this case, some dentists or assistants might want to close the gap by adding porcelain, but ultimately, that would be detrimental because it would create a disproportionate contact length.12
Using a CAD/CAM system to overlay the original biocopy image onto the proposed preparations can provide the clinician with valuable insights to inform the restoration. In this case, when the original scan that was taken before preparing the teeth was superimposed over the proposals, it became clear that the final position of the gingiva was actually much higher (Figure 23). The gap displayed in Figure 22 was a result of the packed cord on teeth Nos. 8 and 9 as well as the gingiva being pushed back. When the clinician sees that the original position of the gingiva is higher, he or she can safely assume that after the crowns are placed and bonded, the gingiva will bounce back and close the black triangle.12 The gap can be left open while the clinician transitions to final milling and cementation. Because the height of the gingiva is maintained, the contact does not lengthen. It is important not to blunt the gingiva. In an anterior case, the biocopy should always be scanned so it can be referred to later during the design phase. Many important details can be determined from the biocopy, including the height of the gingiva, the emergence profile, the length of the incisal edges, the height of the teeth, and other information.13,14
Custom Staining Is Crucial
A 93-year-old patient was unhappy with the appearance of his teeth and insisted that something be done about them on the same day as his recall examination (Figure 24). Among his maxillary and mandibular incisors, there was some recurrent decay, failing composite fillings, and the presence of overlaps. This type of case usually necessitates that a wax-up from the laboratory be transferred into the mouth for patient approval, but this patient was in a hurry. The clinician agreed to have the teeth prepared in the morning and then delivered in the evening. The restorations were designed using a grid to make them as symmetrical as possible. When the restorations were milled, there was a shade change between the gingival third and the incisal third, but the change was not enough to mimic the patient's surrounding natural teeth. Consequently, the clinician had to perform extensive staining. Four stains were used, including dark orange on the gumline, which transitioned to yellow and beige on the body of the restoration. Figure 25 shows the final postoperative image. Due to recession, the patient's teeth appeared longer, and there were also some dark areas around the gumline. Using the different stains enabled the clinician to mimic the shade variation in the patient's natural teeth. Oftentimes, a custom staining job is necessary to achieve acceptable esthetics in anterior CAD/CAM restorations.
Assess Texture of Neighboring Teeth
The extent to which a clinician incorporates staining, glazing, or polishing should involve an assessment of the texture and luster of the neighboring dentition. A patient presented with a large composite filling on tooth No. 9 that had failed or fractured (Figure 26). The filling had been replaced several times before the patient requested a more permanent restoration. A veneer was chosen, and the clinician prepared the case. A dry try-in of the veneer is shown in Figure 27. Dry try-ins are one of the most important parts of an appointment because this is when the clinician decides whether to stain and glaze or just polish.15
In this case, the clinician noticed some incisal translucency on the adjacent teeth. However, when the clinician compared tooth No. 8 to teeth Nos. 7 and 10, it was clear that No. 8 was less lustrous. When compared with the laterals, it did not have a high-gloss finish-it had a matte appearance. To avoid making the restoration for tooth No. 9 too shiny, the clinician decided that an extensive glazing cycle was not needed and instead, finished it to mimic the translucency seen on the adjacent teeth. Blue stains were applied to the incisal edge, and the restoration was put through a crystallization process. After the restoration was finished, the clinician tried it in the patient's mouth and began polishing. It was checked every few seconds, and the polishing was discontinued when the facial texture of the veneer matched that of tooth No. 8. (Figure 28).
In a case where an implant was placed in position No. 9 by a periodontist, the patient needed a crown, so the clinician made a custom abutment with a CAD/CAM system (Figure 29). After milling, the clinician used a 330 bur to scribe some of the texturing seen on tooth No. 8 onto tooth No. 9 (Figure 30). The texturing was mimicked using an articulating paper technique in which the clinician rubbed the articulating paper on both teeth. These cases illustrate the importance of closely assessing the texture and luster of neighboring teeth.
Split Complex Cases Into Two Appointments
A patient presented with failing veneers, some of which had open margins, had debonded, or had been recemented (Figure 31). Contributing to the patient's unhappiness with the final result, there was also recurrent decay and recession as well as a crack on the veneer on tooth No. 9. When the clinician took the case, tooth No. 6 had a relatively new crown. The decision was made to leave this crown in place, but remove the veneers on teeth Nos. 7, 8, 9, 10, and 11. The clinician prepared these teeth for full-coverage crowns. The final result demonstrates a straightened midline, corrected symmetry of centrals, and even improved esthetics on the incisal edges (Figure 32). Because the original contact length was too long, the clinician cleaned up the gingiva and gave it a more gradual emergence profile, enabling it to grow back. Next, the laterals were made to look more natural by ensuring that the mesial-line angles traveled toward the distal, as opposed to being too symmetrical. When the clinician tried to mimic the mesial-line angle equally on teeth Nos. 7 and 10, triangular-looking laterals resulted. A lateral should look more like a triangle (ie, with the apex going toward the gingiva) than a thin or thick oval. The inclination of the laterals should also be mesial and lingual; however, this patient presented with laterals inclined facially and distally.7
Preoperatively, there was no definition of the incisal embrasures in this case. Postoperatively, the incisal embrasure between the centrals was the smallest, the incisal embrasures between the centrals and the laterals were somewhat larger, and the incisal embrasures between the laterals and the canines were the largest. Incisal embrasures tend to become larger distally.16,17
This case illustrates the final recommendation for anterior CAD/CAM restorations, which is to split complex cases into two appointments. When clinicians create CAD/CAM restorations for more complex cases all in one day, they have to manage the patient and the case simultaneously. Rushing can lead to mistakes and subsequently, less-than-natural results after the case is bonded into place.
Conclusion
Many criticisms of CAD/CAM technology ignore the need for specialization and detail oriented postfabrication methods. When fabricating CAD/CAM restorations, enhancements are essential to creating a natural, esthetically pleasing outcome. In the pursuit of a successful result, clinicians should consider recommendations for posterior and anterior CAD/ CAM restorations. The choice of techniques should be case-driven and take into account the patient's preoperative esthetics and desires. The benefits of CAD/CAM, especially when there is a significant amount of attention paid to customization, make it a viable option for many dental practices.
About the Author
Dhaval Patel, DDS
Private Practice
Roseville, California
References
1. Wittneben JG, Gavric J, Belser UC, et al. Esthetic and clinical performance of implant-supported all-ceramic crowns made with prefabricated or CAD/CAM zirconia abutments: a randomized, multicenter clinical trial. J Dent Res. 2017;96(2):163-170.
2. Patel B, Chhabra N, Jain D. Effect of different polishing systems on surface roughness of nano-hybrid composites. J Conserv Dent. 2016;19(1):37-40.
3. Awad D, Stawarczyk B, Llie N. Translucency of esthetic dental restorative CAD/CAM materials and composite resins with respect to thickness and surface roughness. J Prosthet Dent. 2015;113(6):534-540.
4. Zhang Y, Lawn BR. Novel zirconia materials in dentistry. J Dent Res. 2018;97(2):140-147.
5. Zhao M, Sun Y, Zhang J, Zhang Y. Novel translucent and strong submicron alumina ceramics for dental restorations. J Dent Res. 2018;97(3):289-295.
6. Rinke S, Fischer C. Range of indications for translucent zirconia modifications: clinical and technical aspects. Quintessence Int. 2013;44(8):557-566.
7. Nold SL, Horvath SD, Stampf S, Blatz MB. Analysis of select facial and dental esthetic parameters. Int J Periodontics Restorative Dent. 2014;34(5):623-629.
8. Ormianer Z, Solodukhin AL, Lauritano D, et al. Bilateral symmetry of anterior maxillary incisors: evaluation of a community-based population. J Biol Regul Homeost Agents. 2017;31(2 Suppl):37-43.
9. Betrine Ribeiro J, Alecrim Figueiredo B, Wilson Machado A. Does the presence of unilateral maxillary incisor edge asymmetries influence the perception of smile esthetics? J Esthet Restor Dent. 2017;29(4):291-297.
10. Fischer KR, Grill E, Jockel-Schneider Y, et al. On the relationship between gingival biotypes and supracrestal gingival height, crown form, and papilla height. Clin Oral Implants Res. 2014;25(8):894-898.
11. Nayak A, Raipoot N, Nayak R, Nayak R. Analysis of morphologic attributes in dental esthetics: a new concept. Int J Periodontics Restorative Dent. 2017;37(6):873-880.
12. Brianezzi LFF, Brondino BM, Chaves GC, et al. Interdental papilla formation after diastema closure. Gen Dent. 2017;65(6):e13-e16.
13. Patel D. CAD/CAM design techniques for predictable anterior restorations. Inside Dentistry. 2015;11(2):62-70.
14. Sannino G, Germano F, Arcuri L, et al. CEREC CAD/CAM chairside system. Oral Implantol (Rome). 2015;7(3):57-70.
15. Brady LA. Anterior veneer try-in. Lee Ann Brady DMD Dental Practice Excellence. https://leeannbrady.com/esthetic-dentistry/anterior-veneer-try-in. Accessed May 22, 2018.
16. Eduarda Assad Duarte M, Martins Machado R, Fonseca Jardim da Motta A, et al. Morphological simulation of different incisal embrasures: perception of laypersons, orthodontic patients, general dentists, and orthodontists. J Esthet Restor Dent. 2017;29(1):68-78.
17. Foulger TE, Tredwin CJ, Gill DS, Moles DR. The influence of varying maxillary incisal edge embrasure space and interproximal contact area dimensions on perceived smile aesthetics. Br Dent J. 2010;209(3):E4.