You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
At the center of many occlusal philosophies is a specific orthotic. Many times, the orthotic becomes such an integral part of the philosophy that the splint is named after the person who devised it or the institution where it was invented. For example, the Michigan Splint,1 which is of the full-coverage variety, was developed by Sigurd Ramfjord and Major Ash Jr at the University of Michigan. Victor Lucia, who created the Lucia jig in 1964,2 described the use of an “anterior jig” and was the first to use an anterior deprogrammer. Henry Tanner3 developed a mandibular orthotic, used by The Pankey Institute, called the Tanner Appliance.
These dentists were experts in the diagnosis and treatment of occlusal issues; however, there is not one “magic” appliance that will solve all problems. The use of any specific type of orthotic should be reserved for a clearly defined purpose that relates to a specific condition. Today diagnosis and classification of every temporomandibular joint disorder, as well as problems affecting the masticatory musculature, is possible. Thus, classification of specific problems should always precede selection of treatment, including the choice of an orthotic, if indicated. Too often, the orthotic, rather than a diagnosis, becomes the starting point of treatment. This article will revisit the Dawson classification of occlusion and align specific occlusal treatments to the appropriate classification.
The goal of every occlusal treatment is to create a healthy, pain-free, stable occlusion. There are five requirements4 for achieving long-term occlusal stability. These occlusal goals are:
- Stable holding contacts on all teeth (or an acceptable substitute) when condyles are in centric relation (CR) or adapted centric posture (ACP).
- Anterior guidance in harmony with the envelope of function.
- Immediate disclusion of the posterior teeth in protrusion.
- Immediate disclusion of the posterior teeth on the nonworking side.
- Immediate disclusion of the posterior teeth, whenever possible, on the working side.
DAWSON CLASSIFICATION REVISITED
The most commonly used occlusal classification in dentistry, the Angle’s classification,5 fails to observe the relationship of the teeth to the TMJs or consider the health, position, or condition of the TMJ. By contrast, in the Dawson classification,6 the health and stability of the joint is a primary concern, as well as the relationship of the joints to the maximal intercuspation. A joint that is changing position or deteriorating will directly impact the arch-to-arch relationship and ultimately radically affect occlusion.
Dawson I: Maximum intercuspation is in harmony with the CR.
This is one of the primary goals for the completion of occlusal therapy for a healthy TMJ. The teeth occlude in maximum intercuspation when the condyles are in CR (which is the maxillo-mandibular relationship when the properly aligned, condyle-disc assemblies are in the most superior position against the eminentiae, irrespective of tooth position or vertical dimension).7
Dawson Ia: Maximum intercuspation is in harmony with ACP.
This is one of the primary goals for the completion of occlusal therapy for a disordered TMJ. The teeth occlude in maximum intercuspation when the condyles are in ACP (the manageably stable relationship of the mandible to the maxilla that is achieved when deformed TMJs have adapted to a degree that they can comfortably accept firm loading when completely seated at the most superior position against the eminentiae).8 Technological advances using conventional computed tomography images or cone-beam computed tomography (CBCT) are indispensible aids in determining when a disordered TMJ is stable.
Dawson II: Condyles must displace from a verifiable CR for maximum intercuspation to occur.
Dawson IIa: Condyles must displace from an ACP for maximum intercuspation to happen.
With the II or IIa occlusion, CR or ACP joint position has been verified, ruling out an intracapsular TM disorder as a source of pain. Therefore, if pain is a factor, the discomfort most likely will be caused by a muscle related to the discrepancy between maximum intercuspation and ideal condylar relationship. The treatment goal is to achieve a Type I or Type Ia. Any surgical intervention for the TMJ is contraindicated in this group. Treatment can be reversible with an occlusal orthotic (anterior deprogrammers are an excellent choice to help with condylar seating). In many patients, definitive occlusal therapy can be considered as the primary treatment modality using one or more options:
- Occlusal equilibration
- Orthodontics
- Restorative dentistry
- Orthognathic surgery
The goal is to do the least amount of dentistry, using the most conservative approach, to satisfy the five requirements of a stable occlusion.
Dawson III: TMJs cannot accept loading without tenderness or tension, so the relationship of maximum intercuspation to the ideal joint position cannot be determined until the TMJ problem is resolved. Typically, this is transitory and resolvable.
For the patient who may have an intracapsular structural disorder, special emphasis is placed on diagnosis using the Piper Classification. Treatment will vary from simple permissive occlusal splint to short-term directive splint to help decrease inflammation in the joint. Anti-inflammatory medications or surgical correction may be indicated. When the diagnosis has been established, the goal of initial treatment is directed toward guiding the joints to accept CR or ACP: a second treatment phase will establish the ultimate objective of a Type I or Type Ia occlusion.
An analysis must determine whether the failure to seat the condyles is the result of muscle bracing that prevents complete seating of the joints, or if the joints cannot be completely seated due to a structural intracapsular disorder. If the problem is limited to muscle bracing, an anterior deprogrammer splint is a good diagnostic device. If the appliance eliminates the muscle hypercontraction allowing the joints to seat, occlusal interferences are the cause of muscle bracing. A good outcome can be predicted if the occlusal harmony is perfected. Failure of the anterior splint to relieve the discomfort may indicate the presence of a TMJ intracapsular disorder.
Dawson IV: The occlusal relationship is in an active stage of progressive disorder because of pathologically unstable TMJs.
The TMJ is actively degrading, making it impossible to establish a stable TMJ/occlusal relationship. The goal is to manage the progression of the TMJ deformation until stability of the TMJs can be confirmed. Similar to Type III, a second phase of therapy using the four treatment options will be required to achieve the optimal goal of a Type Ia occlusion. The use of anterior deprogrammers is contraindicated in this group. If an occlusal splint is to be employed, a maxillary or mandibular full-coverage permissive appliance should be considered.
DIAGNOSTIC PROTOCOL
At the center of any quality occlusal philosophy is a regimented diagnostic protocol. Occlusal disease can manifest in any or all parts of the gnathostomatic system. It is the clinician’s job to determine if the occlusion is ideal and whether the occlusal discrepancy is causing problems with the joints, muscles, or teeth. A programmed analysis of the entire system is the only way to determine this. TMJ/occlusal analysis should include these seven steps:
- History—A thorough history reveals a great deal about the health and function of the TMJs and other parts of the system. If pain has been a factor, note its specific region, triggers, intensity, and duration.9 Developing a picture of the structural damage to the system, based on the patient’s history, is a critical component of the examination.
- Range of Motion—Normal range of motion on opening is 40 mm to 60 mm without discomfort. Note any deviations to the right or left, remembering that the chin generally deviates toward the damaged joint. A range of 10 mm to14 mm is normal in protrusion, with 10 mm to the right and left.10
- Load Testing—Orthopedic load testing is standard protocol when examining the health of other joints.11 For verification of comfort in CR or ACP, any sign of tension or tenderness warrants further evaluation.
- TMJ Auscultation—Technology such as joint vibration analysis or TMJ Doppler auscultation allows clinicians to evaluate the health of various parts of the joint.12-19 An intact healthy joint is quiet on rotation and translation, eliciting zero vibration. In the disordered TMJ, fine, medium, and course crepitus can be found on the medial or lateral poles, allowing a better understanding of the disease inside the joint and a more precise diagnosis.
- Muscle Palpation—Muscles that are tender on palpation indicate muscular hyperactivity.20 This can lead to joint overload, disc displacement, or damage to the teeth/supporting structure, as well as contributing significantly to the patient’s pain.
- Tooth Wear, Mobility Migration—A thorough evaluation of the dentition for wear facets, migrating teeth, and mobile teeth is part of the diagnosis for occlusal stability. Evaluating the teeth intraorally, along with the use of properly mounted diagnostic casts and high-resolution digital photography, is an excellent way to study and document occlusal issues.21
- TMJ Imaging—If all other findings of the examination are negative, detailed imaging of the joint is not necessary. CT images are the gold standard to view the joint’s hard tissues. Increased diagnostic capabilities allow the clinician to determine if the joint is actively breaking down, regressive remodeling, or stabilized.22-25 An MRI can be used when it’s necessary to see specific details with regard to the disc or edema in the joint space.26-28
RELATING OCCLUSAL TREATMENT TO THE DAWSON CLASSIFICATION
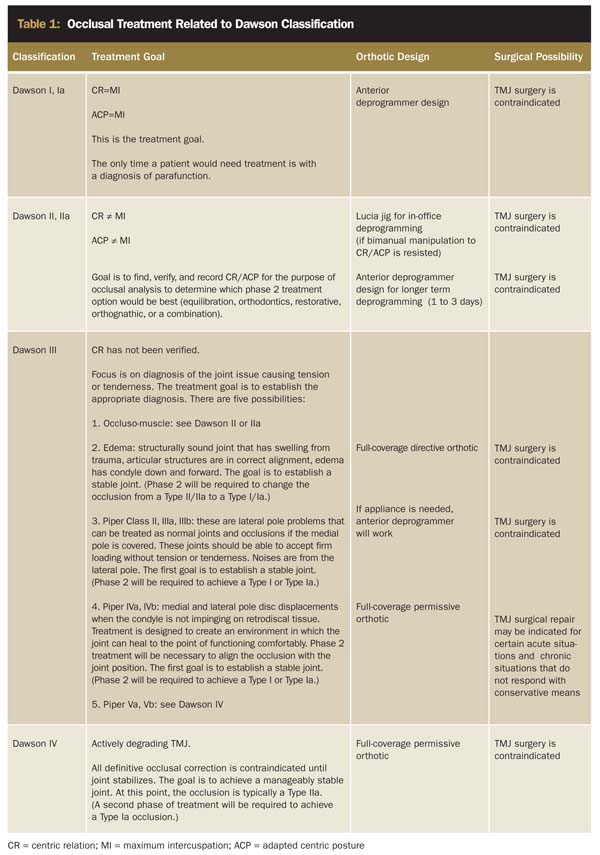
As stated previously, the first goal of occlusal treatment is to establish Type I in the healthy TMJ and Type Ia in the disordered TMJ. The clinician must determine which patient will need an orthotic, and, if so, what design (Table 1). If splint therapy is successful, what other types of dentistry will be needed afterwards to fulfill the remaining requirements of a stable occlusion? To simplify this discussion, treatment may be divided into two phases.
 |
Phase 1 Treatment: Occlusal Splints
Most occlusal splints have one primary function: to alter an occlusion to create an environment that will allow the condyles to completely seat in CR or ACP. The goal is to choose the correct appliance that will achieve condylar stability as efficiently as possible. There are three general categories of splints:
- Anterior Deprogrammer—This appliance allows the lower incisors to contact a flat surface in the maxillary anterior region.29-32 This separates the posterior teeth, eliminating all the mechanoreception from the posterior teeth. The lack of mechanoreception allows the lateral pterygoid to release, providing easy seating of the condyles into CR. Anterior deprogrammers are an excellent aid when attempting to move the “muscularly tight patient” from a Type II, IIa to a Type I, Ia.33-36 This appliance is contraindicated in patients with unhealthy joints because the lack of posterior contact will increase joint loading.
- Permissive Full-Coverage Orthotic—The permissive splint is a maxillary or mandibular full-coverage orthotic that provides flat equal intensity contacts around the arch, with shallow anterior guidance.37 It is often the splint of choice for patients who have unstable joints related to disc displacement, and those with degenerative changes to the articular surfaces of the condyle.38-41 With unstable TMJs, it is necessary to readjust the occlusal contact as changes occur in the joints.
- Directive Full-Coverage Orthotic—The directive maxillary or mandibular full-coverage orthotic will direct the mandible into a specific position in space. An anterior repositioning splint (ARS) is an example of a directive appliance.42,43 It is designed for short-term use after traumatic injury when edema is in the joint. Bringing the mandible forward for a short period will decrease the inflammation. Then the appliance can be adjusted to allow the condyle to completely seat to CR or ACP. Such treatment is typically combined with a soft diet and anti-inflammatory medications.
Splint Use and the Dawson Classification
The goal of the occlusal splint is to create a Type I or Type Ia condylar relationship between the occlusion and TMJs. The following conditions may warrant the use of specific splints:
Dawson Type I or Type Ia
In certain situations, some patients with Type I/Type Ia can experience episodic muscular symptoms even with a perfected occlusion. In these cases, the use of a clenching suppression appliance that involves isolated contact only on a single midline stop is an acceptable aid for periodic use to maintain comfort.44 Conjointly, in those parafunctioning Type I and Type Ia cases in the absence of any muscular symptoms, a complete coverage splint with CR contact on all teeth with an anterior ramp for posterior disclusion in all excursions can be an effective long-term risk management appliance. This mitigates the effects of excessive occlusal loading of the teeth and supporting structures. However, a more precise correction of the occlusion will often eliminate the need for an appliance if perfected to a Type I or Type Ia.
Dawson Type II or Type IIa
The Type II or Type IIa joint is most common. The slide that exists between maximum intercuspation and CR/ACP must be found and eliminated to establish an ideal occlusal relationship.
To choose the most appropriate method to eliminate the slide, study models should be mounted on an articulator in CR/ACP. Bimanual manipulation as described by Dawson in most instances can be used without an orthotic to find, verify, and record CR. If this can be accomplished, an orthotic will not be required to move on to Phase 2.
However, when dentists are learning this skill or patients are extremely tight, deprogramming appliances can help tremendously. Using a Lucia jig during the occlusal examination, fixed to the maxillary incisors with a compound, is often all that is required to relax the masticatory muscles. Allowing the patient to relax for about 15 mins with the jig in place, then trying again with bimanual manipulation (using firm load testing) will usually verify the ideal condylar position.
Occasionally, a patient will not respond to bimanual manipulation or short-term deprogramming. In the absence of a structural TMJ disorder, an anterior deprogramming appliance may be fabricated to be worn for 2 to 3 days. This longer-term deprogramming will allow the muscles to relax to the extent that even the most novice dentist can use bimanual manipulation to find, verify, and record CR.
There are three options to find, verify, and record CR/ACP:
- Use bimanual manipulation—for the patient who has a relatively easy-to-find CR/ACP.
- Employ a Lucia jig with bimanual manipulation—for the dentist who is learning or a patient with tight muscles.
- Use a longer-term deprogrammer with bimanual manipulation—for the patient who is extremely tight and does not respond to short-term deprogramming.
Dawson Type III
With Type III, CR/ACP cannot been verified. Some aspect of the TMJ–occlusal evaluation prevents the clinician from concluding that an orthopedically stable condylar position can be achieved at that time. Type III poses the greatest diagnostic challenge. The following is a general description of the diagnostic possibilities and the correctly aligned occlusal therapy.
- Occluso-muscle problems: The source of pain may be confusing in a patient with very sore muscles (particularly the lateral pterygoid). Anterior deprogrammers can be an excellent tool for differential diagnosis. If a deprogrammer appliance is given to a patient who has pain, it should be with the explicit instructions to remove the appliance if the pain increases. Should pain increase, then further imaging (MRI) should be considered to verify the specific pathologic condition of the joint. If the pain remits, then the CR/ACP should be able to be established and treatment for Type II/IIa should be employed.
- Lateral pole displacements: If the joint derangement is determined to involve only the lateral pole of the condyle (Piper II, IIIa, IIIb—the joint can accept full loading in the most superior position, the medial pole is intact), then the problem can be treated like a Type IIa.
- Medial pole problems: When the articular disc is displaced off the medial pole (Piper IVa, IVb) and the joint has not adapted to the point of stability. The goal of treatment may be to use an orthotic to help create an environment that would allow the condyle disc assembly to adapt and heal. Employing a full-coverage permissive splint (maxillary or mandibular) is often the treatment of choice. This can be a long process that may also involve anti-inflammatory medications and physical therapy.
Whenever the medial pole is displaced, surgical correction may be a consideration. Chronic conditions that do not respond to conservative means or certain acute situations may be best managed with surgery.
- Edema/swelling: When trauma has occurred to the TMJ, edema can cause pain and prevent the joint from seating. A directive splint can be used to bring the mandible forward for a short period until the joint can accept loading. The appliance is then adjusted to a permissive splint designed to allow condylar seating. At that time, protocols for Type II and Type IIa joint may be used.
- Active TM joint degeneration: See Dawson Type IV.
Dawson Type IV
The Type IV joint is the most complicated to treat because as the condyle deteriorates, the occlusion is in a constant state of flux (Piper Va, Vb). The goal of splint treatment is to design an appliance to spread the load evenly throughout the system, minimize joint loading, and decrease muscle activity. The full-coverage permissive splint (maxillary or mandibular) is often the appliance of choice for this patient. The Piper Va will be degrading rapidly, while Vb is a slower, more chronic process. The appliance will need to be adjusted continually until the occlusion stabilizes. CBCT technology can help in determining whether the regressive remodeling has ceased or slowed to a manageable degree.
Phase 2 Treatment
Phase 2 involves occlusal equilibration, orthodontics, restorative dentistry, orthognathic surgery, or a combination of these. These treatments are specifically used to shift the Dawson Type II to a Type I, or a Type IIa to a Type Ia. Once the condylar position has been verified, the case is studied using mounted diagnostic models, photographs, and radiographs/imaging. Then, the appropriate treatment is planned. The occlusal end point is to establish the previously described five requirements of stability, using the most conservative approach possible.
CONCLUSION
Solving complex occlusal problems can be tremendously rewarding. The key to successful treatment outcomes is to develop a process of programmed diagnosis and treatment. Focusing on a thorough diagnostic work up and aligning the appropriate diagnosis with time-tested treatment options is the key to success.
REFERENCES
1. Ash MM Jr, Ramfjord SP. Reflections on the Michigan splint and other intraocclusal devices. J Mich Dent Assoc. 1998;80(8):32-46.
2. Lucia VO. A technique for recording centric relation. J Prosthet Dent. 1964;14:492-505.
3. Tanner HM. The Tanner Mandibular Appliance. J Colo Dent Assoc. 1996;75(2):14-18.
4. Dawson PE. A classification system for occlusions that relates maximal intercuspation to the position and condition of the temporomandibular joints. J Prosthet Dent. 1996;75(1):60-66.
5. Angle EH. Classification of Malocclusion of the Teeth. 7th ed. Philadelphia, PA: S.S. White Dental Manufacturing Company;1907:35-59.
6. Dawson PE. Functional Occlusion: From TMJ to Smile Design. St. Louis, MO: Mosby, Inc; 1985:103-111.
7. Dawson PE. Centric relation. Continuum (N Y). 1980:49-60.
8. Dawson PE. New definition for relating occlusion to varying conditions of the temporomandibular joint. J Prosthet Dent. 1995;74(6):619-627.
9. Okeson JP. Fundamentals of Occlusion and Temporomandibular Disorders. St. Louis, MO: Mosby; 1985:185-189.
10. Okeson JP. Fundamentals of Occlusion and Temporomandibular Disorders. St. Louis, MO: Mosby; 1985:200-203.
11. Konin JG, Wiksten DL, Isear JA Jr, et al. Special Tests for Orthopedic Examination. 3rd ed. Thoroughfare, NJ: Slack Inc; 2006.
12. Sano T, Widmalm SE, Westesson PL, et al. Amplitude and frequency spectrum of temporomandibular joint sounds from subjects with and without other signs/symptoms of temporomandibular disorders. J Oral Rehabil. 1999;26(2):145-150.
13. Honda K, Natsumi Y, Urade M. Correlation between MRI evidence of degenerative condylar surface changes, induction of articular disc displacement and pathological joint sounds in the temporomandibular joint. Gerodontology. 2008;25(4):251-257.
14. Garcia AR, Madeira MC, Paiva G, et al. Joint vibration analysis in patients with articular inflammation. Cranio. 2000;18(4):272-279
15. Leader JK, Robert Boston J, Rudy TE, et al. Quantitative description of temporomandibular joint sounds: defining clicking, popping, egg shell crackling and footsteps on gravel. J Oral Rehabil. 2001;28(5):466-478.
16. Honda K, Natsumi Y, Urade M. Correlation between MRI evidence of degenerative condylar surface changes, induction of articular disc displacement and pathological joint sounds in the temporomandibular joint. Gerodontology. 2008;25(4):251-257.
17. Motoyoshi M, Sadowsky PL, Kamijo K et al. Studies of temporomandibular joint sounds; part 4. Phase relations of TMJ sounds and jaw movement. J Nihon Univ Sch Dent. 1996;38(3-4):155-160.
18. Widmalm SE, Williams WJ, Adams BS. The wave forms of temporomandibular joint sound clicking and crepitation. J Oral Rehabil. 1996;23(1):44-49.
19. Olivieri KA, Garcia AR, Paiva G, et al. Joint vibrations analysis in asymptomatic volunteers and symptomatic patients. Cranio. 1999;17(3):176-183.
20. Okeson JP. Fundamentals of Occlusion and Temporomandibular Disorders. St. Louis, MO: Mosby. 1985:191-199.
21. Dawson PE. Functional Occlusion: From TMJ to Smile Design. St. Louis, MO: Mosby, Inc; 2007:18-26.
22. Bamgbose BO, Adeyemo WL, Ladeinde AL, et al. Conebeam computed tomography (CBCT): the new vista in oral and maxillofacial imaging. Nig Q J Hosp Med. 2008;18(1):32-35.
23. Fu KY, Zhang WL, Liu DG, et al. Cone beam computed tomography in the diagnosis of temporomandibular joint osteoarthrosis. Zhonghua Kou Qiang Yi Xue Za Zhi. 2007;42(7):417-420.
24. Stratemann SA, Huang JC, Maki K, et al. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol. 2008;37(2):80-93.
25. Honey OB, Scarfe WC, Hilgers MJ, et al. Accuracy of cone-beam computed tomography imaging of the temporomandibular joint: comparisons with panoramic radiology and linear tomography. Am J Orthod Dentofacial Orthop. 2007;132(4):429-438.
26. El-Essawy MT, Al-Nakshabandi NA, Al-Boukai AA. Magnetic resonance imaging evaluation of temporomandibular joint derangement in symptomatic and asymptomatic patients. Saudi Med J. 2008;29(10):1448-1452.
27. Larheim TA. Role of magnetic resonance imaging in the clinical diagnosis of the temporomandibular joint. Cells Tissues Organs. 2005;180(1):6-21.
28. Güler N, Yatmaz PI, Ataoglu H, et al. Temporomandibular internal derangement: correlation of MRI findings with clinical symptoms of pain and joint sounds in patients with bruxing behaviour. Dentomaxillofac Radiol. 2003;32(5):304-310.
29. Hunter BD 2nd, Toth RW. Centric relation registration using an anterior deprogrammer in dentate patients. J Prosthodont. 1999;8(1):59-61.
30. Yustin D, Neff P, Rieger MR, et al. Characterization of 86 bruxing patients with long-term study of their management with occlusal devices and other forms of therapy. J Orofac Pain. 1993;7(1):54-60.
31. Jokstad A, Mo A, Krogstad BS. Clinical comparison between two different splint designs for temporomandibular disorder therapy. Acta Odontol Scand. 2005;63(4):218-226.
32. McKee JR. Comparing condylar positions achieved through bimanual manipulation to condylar positions achieved through masticatory muscle contraction against an anterior deprogrammer: a pilot study. J Prosthet Dent. 2005;94(4):389-393.
33. Skinner CE, Neff PA. The effect of non-surgical management of TM disorders. NDA J. 1994;45(1):14-18.
34. Stapelmann H, Türp JC. The NTI-tss device for the therapy of bruxism, temporomandibular disorders, and headache - where do we stand? A qualitative systematic review of the literature. BMC Oral Health. 2008;8:22.
35. Jokstad A. The NTI-tss device may be used successfully in the management of bruxism and TMD. Evid Based Dent. 2009;10(1):23.
36. Magnusson T, Adiels AM, Nilsson HL, et al. Treatment effect on signs and symptoms of temporomandibular disorders—comparison between stabilisation splint and a new type of splint (NTI). A pilot study. Swed Dent J. 2004;28(1):11-20.
37. Wiygul JP. Maxillary full-coverage appliance. Cranio Clin Int. 1991;1(2):39-53.
38. Bumann A, Kopp S, Stangohr M, et al. Value of bite-guard splints for dysfunctions of the masticatory system. Dtsch Zahnarztl Z. 1989;44(11 spec no):S14-S16.
39. Gray RJ, Davies SJ. Occlusal splints and temporomandibular disorders: why, when, how? Dent Update. 2001;28(4):194-199.
40. Major PW, Nebbe B. Use and effectiveness of splint appliance therapy: review of literature. Cranio. 1997;15(2):159-166.
41. Murakami K, Kaneshita S, Kanoh C, et al. Ten-year outcome of nonsurgical treatment for the internal derangement of the temporomandibular joint with closed lock. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(5):572-575.
42. Tecco S, Caputi S, Teté S, et al. Intra-articular and muscle symptoms and subjective relief during TMJ internal derangement treatment with maxillary anterior repositioning splint or SVED and MORA splints: A comparison with untreated control subjects. Cranio. 2006;24(2):119-129.
43. Tecco S, Festa F, Salini V, et al. Treatment of joint pain and joint noises associated with a recent TMJ internal derangement: a comparison of an anterior repositioning splint, a full-arch maxillary stabilization splint, and an untreated control group. Cranio. 2004;22(3):209-219.
44. Baad-Hannsen L, Jadidi F, Castrillon D, et al. Effect of a nociceptive trigeminal inhibitory splint on electromyographic activity in jaw closing muscles during sleep. J Oral Rehabil. 2007;34(2):105-111.