You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Halitosis is an unpleasant, often offensive odor emanating from the mouth and/or nose. It is usually of intraoral origin and results from microbial degradation of organic substrates, thereby producing volatile sulfur compounds (VSCs) and other odor-producing byproducts.1 There are also other malodor-generating mechanisms, such as xerostomia and metabolic disease.1 For some individuals, halitosis is not a minor inconvenience; it is an issue they think about daily.2 Malodor may be a primary motivator for a first-time dental visit or a secondary (unspoken) concern during recall visits.3,4
Because this issue is of great dental and social importance, this article proposes a practical guide for management of halitosis. Based on etiology and clinical presentation, malodor has been reclassified encompassing eight types of halitosis: tongue biofilm, periodontal, peri-implant, xerostomia-related, airway/ear, nose, and throat (ENT), metabolic/systemic, pseudo-halitosis, and halitophobia. Using this classification as a framework, practical diagnostic and treatment algorithms are discussed.
Data for this narrative review were collected via an electronic search using PubMed, MEDLINE, and Google Scholar databases employing the following keywords: “halitosis” AND/OR “oral malodor” AND “etiology” AND “diagnosis” AND “treatment.”
Prevalence of Halitosis
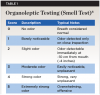
Occurrence estimates for halitosis vary widely depending on populations studied and methods used to detect malodor.5,6 Two fundamentally different types of investigations exist that provide different results: population-based epidemiologic surveys and clinical or dental-office–based studies. Large epidemiologic surveys note halitosis prevalence rates ranging from 2.4% to 55.38%.6 In a systematic review of 13 epidemiologic studies, Silva et al reported an organoleptic (smell test) halitosis worldwide frequency of 31.8%.6 This value is often misinterpreted as a mean prevalence, but it represents a pooled trend estimate derived from a meta-analysis in which study weights are adjusted for sample size.7 Furthermore, Silva et al’s analysis6 included patients’ self-reported data, assumed chemically detected odor levels, and mild or barely perceptible odor levels (organoleptic scores 0–1; Table 1),8 thereby inflating prevalence estimates relative to clinically relevant malodor.
Several review articles have suggested that approximately 5% of the population suffers from severe halitosis.9,10 This figure, however, did not originate from epidemiologic studies that stratified disease severity; it was derived from narrative synthesis and interpretation across heterogeneous studies.11 From another perspective, clinical and dental-office–based investigations report higher proportions of severe halitosis compared to epidemiologic studies (14% to 22%).12-14 This discrepancy reflects sampling bias, as clinical cohorts over-represent individuals seeking care for oral complaints and disproportionately include more severe cases. Consequently, based on currently available data, a precise prevalence of mild, moderate, or severe halitosis in the general population cannot be reliably defined.
Halitosis Vs Halitophobia
Malodor disorders are traditionally classified into three distinct categories15: “Genuine halitosis” is objectively detectable malodor confirmed by organoleptic assessment or VSC measurement. “Pseudo-halitosis” denotes a condition in which no objective malodor is detected, but the patient believes they have bad breath. “Halitophobia” is defined as persistent belief of bad breath despite successful treatment and repeated expert reassurance. This latter condition represents a psychological disorder.
Main Causes of Halitosis
An existing biological model lists four disease domains (ie, pathophysiologic origin) for halitosis: oral (comprising 85% of cases), airway/ENT, metabolic/systemic, and psychogenic.16 The proposed classification presented in this article further subdivides these domains into types of halitosis to enhance diagnosis and malodor treatment.
Intraoral Causes of Malodor
Tongue coating—Patients with halitosis frequently manifest a tongue coating, which may mirror the patient’s oral or systemic health.17 Coatings consist of a desquamated epithelial-bacterial matrix; it is not classic dental plaque. The surfaces of the tongue comprise both non-keratinized and keratinized epithelial cells and, typically, there is a balance between retaining and shedding cells from these surfaces.18 A thick, tenacious coating on the posterior dorsal surface of the tongue indicates a change in this equilibrium and is often associated with an increase in bacteria.18 Oral microbiome dysbiosis of the tongue is characterized by shifts in bacterial composition and increased anaerobic populations (eg, Porphyromonas gingivalis, Fusobacterium nucleatum).19,20 The bacteria accumulate in papillary crypts and produce VSCs by degrading sulfur-containing amino acids such as cysteine and methionine.18,21 Cysteine is converted to hydrogen sulfide (H2S, rotten egg smell), and methionine is degraded to methyl mercaptan (CH3SH, rotting cabbage smell).21 Other volatile compounds have also been implicated in malodor, including volatile aromatic compounds, short-chain and volatile fatty acids, alcohols, volatile aliphatic compounds, and aldehydes and ketones.21,22
Periodontal disease—Gingivitis and periodontitis create anaerobic environments that generate VSCs and other odorous metabolites.19,21-25 Individuals with periodontitis are three times more likely to have halitosis, increased VSC levels, and thicker tongue coatings than healthy individuals.19 It should be noted, however, that it is possible to have malodor without manifesting a thick tongue coating.22,24
Peri-implant disease—Direct evidence remains limited with respect to specifically isolating peri-implant disease as an independent cause of halitosis.26-28 However, its microbiological resemblance, structural tissue changes, and biofilm are similar to periodontitis. This makes it reasonable to consider implant infected sites as potential contributors to halitosis.
Dental caries and defective restorations—These oral maladies can create food and plaque retention areas where bacteria can degrade deposits.25
Poor oral hygiene—Inadequate brushing and flossing allow plaque accumulation, bacterial overgrowth, and halitosis.29
Xerostomia (dry mouth)—Reduced salivary flow due to medications, aging, or systemic conditions limits natural cleansing and allows bacterial proliferation.17,19,30,31 This can contribute to persistent halitosis. Morning breath represents a transient and physiologic form of malodor caused by temporary nocturnal reduction in salivary flow and mild oral dysbiosis, whereas chronic halitosis is characterized by lingering microbial imbalance and sustained production of VSCs.17,19,32
Oral infections and ulcers—Abscesses or ulcerations may release malodorous compounds.19,33
Diet—Certain sulfur-containing foods, such as onions and garlic, are digested, absorbed into the bloodstream, and transported to the lungs.34 Metabolites are excreted with exhaled air and can contribute to enduring halitosis as they are released through both oral and nasal exhalation.34
Tobacco—Smoking and smokeless tobacco can exacerbate malodor.35
Airway/ENT and Metabolic/Systemic Sources
(Categories Denote Extraoral Halitosis)
Airway/ENT (ear, nose, and throat) and metabolic/systemic origins of halitosis share the same exit points: the oral cavity and the nose. Airway/ENT malodor is generated by local infection and/or protein degradation within the respiratory mucosa (tonsils, adenoids, sinuses, nasal cavity, pharynx, bronchi). Respiratory tract infections include tonsillitis, sinusitis, postnasal drip, and chronic bronchitis. These conditions can produce halitosis.22,36 In contrast, metabolic/systemic issues create malodor molecules (ketones, ammonia, dimethyl sulfide, amines, uremic compounds, indoles, sulfurous metabolites), which are present in blood and tissues due to metabolic failure, hepatic dysfunction, renal insufficiency, diabetes, inborn errors of metabolism, or gut microbial translocation and then passively exhaled through the lungs.22,36 It should be noted that a systemic disease affects multiple organs rather than being limited to one area (eg, diabetes). “Systemic” refers to how widespread the effects are, whereas the term “metabolic” connotes how the disease acts (mechanism). Metabolic disease is actually a subcategory of systemic disease.
Psychogenic Etiology
Clinical studies suggest that 20% to 30% of patients presenting with malodor concerns fall into pseudo-halitosis or halitophobia classifications, underscoring the importance of careful diagnosis and patient communication.37,38 Failure to distinguish genuine halitosis from halitophobia can lead to unnecessary treatment and persistent patient distress.
Proposed Disease-Based Clinical Classification System for Halitosis
Halitosis should be classified according to underlying pathophysiologic processes that generate malodor rather than by symptom perception alone.39 Table 2 presents a clinical classification system listing eight proposed types of halitosis and their defining features.15,17-28,30,31,36-38 While eight types are listed, only types I through VI represent biologic malodor-generating diseases; types VII and VIII are diagnostic endpoints reflecting psychiatric presentations rather than odor-producing pathosis. In this article, halitosis is classified by its dominant etiology and clinical presentation; however, overlap between categories may occur and clinical judgment remains essential for assigning a reason for malodor.
Several issues demand additional explanations. In this classification, xerostomia is considered a primary pathophysiologic mechanism rather than a secondary modifying factor, because reduced salivary flow directly alters oral microbial ecology and odor production. Another issue that requires discussion is the anatomic source of malodor beyond intraoral causes. While intraoral sources account for most cases of clinically encountered halitosis, an etiology-based classification must also accommodate extraoral and psychogenic conditions that present with odor complaints in dental settings. Types V and VI acknowledge well-documented airway, gastrointestinal, and metabolic disorders in which odor-producing compounds originate outside the oral cavity and are transmitted via nasal airflow or pulmonary exhalation. Types VII and VIII are included to distinguish patients with subjective odor perception from those with objectively verifiable malodor, thereby preventing unnecessary dental or medical treatment and facilitating appropriate reassurance or referral. Collectively, inclusion of these categories helps improve diagnostic accuracy and protect patients from over-treatment and reflects the multidisciplinary reality of halitosis evaluation.
Detection of Halitosis: Professional Diagnostic Workflow
Accurate diagnosis is fundamental to effective halitosis management, because oral malodor can be generated by a variety of conditions. Empirical treatment often fails when the etiologic source is not identified. Halitosis evaluation, therefore, should follow a structured professional workflow to confirm genuine malodor, localize its origin, distinguish psychogenic complaint, and guide etiology-matched therapy.40,41 The following diagnostic protocol provides a standardized diagnostic approach.
1. Medical and dental history—Identify risk factors (diet, hygiene, xerostomia, medications, systemic disease).
2. Oral examination—Evaluate tongue coating, periodontal status, caries, salivary flow, and prostheses.
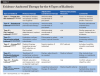
3. Organoleptic scoring—Perform a first-line clinical evaluation (methodology to be discussed later in this article). A separate evaluation is done for oral and nasal air to differentiate intraoral halitosis from extraoral causes (true metabolic/systemic halitosis is uncommon). Differentiating between oral and nasal exhalation is accomplished by pinching the nose to assess oral odor (oral halitosis) and checking nasal exhalations with the mouth closed. Once malodor is confirmed, the clinician can use the halitosis diagnostic algorithm (Table 3) to determine the type of halitosis present.42-65 For each type of halitosis, primary diagnostic findings, key patient assessments, and confirmatory clues are outlined to support accurate classification and targeted management.
In cases of persistent malodor without an identifiable oral source, further investigation is needed to exclude extraoral or psychogenic causes, with appropriate medical referral when indicated. Figure 1 demonstrates how to differentiate between airway/ENT and metabolic/systemic halitosis.22,33,36,40
4. Instrumental corroboration—A Halimeter (VSC measurement) or OralChroma (gas chromatography) device, or alternate verifying tests, may be used for odor (Table 4).18,19,66-68 When instrumental analysis is not available, additional biological correlates can be used to support the diagnosis, including visual scoring of tongue coating and assessment of odor from tongue scrapings.69,70 In most private practice settings, these simple adjunctive tests, along with a thorough history and organoleptic assessment, are sufficient in approximately 85% to 90% of cases.69,70
5. Genuine versus pseudo-halitosis—Distinguishing genuine halitosis from pseudo-halitosis and halitophobia is critical to avoid unnecessary treatment.37,38
Organoleptic Assessment (Subjective Gold Standard)
In an organoleptic assessment, a trained clinician smells the patient’s exhaled air and assigns a score based on odor intensity (Table 1)5,24,71 (scale: 0 [no odor] to 5 [severe malodor]).8 This method is simple, inexpensive, and allows for immediate feedback. It is, however, subjective, influenced by clinician sensitivity and patient factors (eg, recent food or drink).
To reduce bias during a patient assessment, the following precautions can be taken: The examiner should avoid coffee, perfume, and gum for at least 1 hour before testing; a neutral room with no strong ambient odors should be used; and the patient should refrain from eating, smoking, and performing oral hygiene for at least 2 hours before testing. An integral part of testing is having the patient hold their breath for 30 seconds.26,66,71,72 Then the examiner takes an index card and gently wafts exhaled air (breath waft test) laterally to validate or deny the presence of halitosis. An organoleptic score is then recorded.
Patient Self-Assessment Techniques
Patient self-evaluation methods for halitosis are listed in Table 5. Note that none of these tests provide an accurate or reproducible appraisal of true halitosis.66,73 However, as part of a follow-up program, patients can use the breath waft test discussed above and have someone assess their daily progress; this can provide some self-assurance that they are odor free.
Diagnostics: Summary
A diagnosis aligned with each type of halitosis allows for targeted therapeutic intervention. In general, clinicians can identify the underlying cause of halitosis using organoleptic testing coupled with clinical inspection. When needed, supplementary in-office assessments can be performed.
Halitosis Therapies
The management of malodor requires identification and elimination of its underlying causes rather than symptomatic masking alone. Because most cases originate intraorally, treatment strategies primarily focus on mechanical biofilm control and targeted antimicrobial therapy.
Mechanical Oral Hygiene
Brushing and flossing—Brushing and flossing of teeth removes plaque and food debris and reduces bacterial load.74
Tongue cleaning—Tongue scrapers or toothbrushes can be used to reduce tongue coating, as the tongue is the primary site for VSC production.75-77 In the author’s experience, tongue cleansing in the morning is usually sufficient to reduce halitosis, and twice daily cleaning may benefit patients with persistent malodor or heavy tongue coating. Patients should clean from posterior to anterior of the tongue and reach the posterior tongue dorsum as tolerated without causing a gag reflex. Three to five strokes are usually required to cleanse the tongue.78 Patients should avoid aggressive scraping to prevent irritation and rinse the tongue after cleaning to remove loose debris. Tool choice (scraper versus brush) matters less than consistency and coverage of the tongue.76 Tongue cleaning may be adequate to eliminate halitosis if the periodontium is healthy, saliva flow is normal, and there are no nasal/sinus or other medical contributions.79
With consistent daily tongue cleaning as part of an oral hygiene regimen, tongue coating can typically begin to decrease by the second week, and continued adherence is associated with further reduction in coating and halitosis indicators over several weeks.78 This is attributed to fewer bacteria remaining that seed renewed biofilm formation and the establishment of a new equilibrium of the tongue microbiome. However, removal of tongue deposits may not be sufficient to reduce halitosis in some patients and adjunctive therapies may be needed (see Chemical/Antimicrobial Therapy below). If the coating on the tongue cannot be removed with oral hygiene, an underlying health disorder (eg, gastritis) may exist.11,17
Prosthesis care—Dentures, bridges, and orthodontic appliances must be cleaned thoroughly with commercially available prosthesis cleaners.
Chemical/Antimicrobial Therapy
Adjunctive chemotherapeutic agents are especially useful when halitosis, tongue coating, and periodontal disease persist despite mechanical hygiene.
Antimicrobial mouthwashes—Chlorhexidine, cetylpyridinium chloride, or essential oil–based rinses reduce oral bacterial load.80 Other touted products contain chlorine dioxide. Evidence suggests that chlorine dioxide–based rinses function primarily via chemical neutralization rather than masking of odors.81-83 Chlorine dioxide oxidizes hydrogen sulfide, methyl mercaptan, and dimethyl sulfides to odorless sulfates.81-83 Table 6 provides a comparison of benefits regarding chlorine dioxide versus chlorhexidine.81-83
Zinc-containing rinses—These rinses bind and neutralize VSCs.84
Periodontal Therapy (Gingivitis, Periodontitis, Peri-implant Disease)
An integral part of halitosis therapy is management of periodontal disease.24,26,28,50,61 Scaling, root planing, or periodontal surgery should be initiated as necessary, as these procedures help reduce periodontal pathogens and malodor. Routine periodontal maintenance should also be part of ongoing therapy.1,85
Salivary Flow Management
For patients with xerostomia, hydration increases saliva flow and mechanical cleansing. A patient’s fluid intake should include six to eight glasses of water per day.86 For nighttime oral dryness, use of a humidifier may be beneficial, and to enhance nasal patency, a saline spray can be used. Many patients are on medications that may cause dry mouth, such as antihypertensives, antidepressants, antihistamines, and anticholinergics.87 With regard to these medications, before altering prescriptions, dentists should consult with the patient’s physician. Saliva substitutes or stimulants, such as sugar-free chewing gum, lozenges, or sialagogues (pilocarpine in selected cases), can help in xerostomia-related malodor.33,52-54
Additional Treatments for Halitosis
Emerging therapies have been investigated as adjuncts for the management of halitosis, including probiotics, lasers, photodynamic therapy, and ozone treatment.88-94 Current clinical data, however, remains limited and of low quality, and insufficient evidence exists to support a significant or consistent benefit of these interventions in routine halitosis treatment. These adjunctive therapies, therefore, were intentionally excluded from therapeutic recommendations in this review.
Lifestyle and Dietary Modifications
Tobacco cessation reduces odor and periodontal disease risk.35 Dietary adjustments, such as limiting intake of garlic, onions, and highly protein-rich meals, can reduce transient halitosis.34
Treatment of Extraoral (Airway/ENT, Metabolic/
Systemic) Causes
Respiratory infections, to include sinusitis, tonsillitis, and postnasal drip, may require an ENT consultation to eliminate these potential causes of malodor.22,36,55-58 Similarly, medical consultation may be needed for gastrointestinal disorders (eg, Helicobacter pylori infection, selected motility or metabolic conditions).22,36,45,59-61
Management of Pseudo-Halitosis and Halitophobia
Patient education and reassurance may be needed to clarify that objective malodor is absent. With respect to pseudo-halitosis, patients’ emotional concerns typically improve after they receive explanation and professional reassurance. In cases of long-standing halitophobia, however, referring the patient for behavioral or psychiatric therapy may be warranted.15,38,62-65 Clear communication regarding diagnosis and prognosis is essential, particularly for patients with pseudo-halitosis and halitophobia.
Therapeutic Implications
Table 7 summarizes usual therapy for the eight halitosis types described in Table 1 and Table 2.15,22,24,26-28,32,36,38,49-65,75-77,80-87,95-99 Because these groupings reflect fundamentally different sources of malodor, effective management depends on aligning treatment with the origin of odor production, the likelihood of extraoral involvement, and the risk of unnecessary treatment.
Conclusion
Halitosis has historically been approached as a single clinical symptom rather than as a group of distinct disease entities with specific etiologies and therapeutic requirements. This has led to inconsistent diagnostic practices, empiric treatment strategies, and frequent therapeutic failure. The proposed classification is grounded in clinically defined etiological categories and clinical presentation. The accompanying diagnostic and therapeutic algorithms translate this classification into a practical chairside tool that enables targeted treatment. It is the first classification to explicitly integrate xerostomia, peri-implant disease, and psychogenic entities into a unified clinical diagnostic algorithm. This disease-based approach reduces unnecessary interventions, facilitates appropriate medical referral, and allows effective management in most settings without mandatory reliance on gas-analysis instrumentation. This represents a clinically meaningful shift in halitosis care—moving the field from nonspecific symptom suppression toward mechanism-based diagnosis and precision therapy.
ABOUT THE AUTHOR
Gary Greenstein, DDS, MS
Adjunct Professor, Department of Periodontology, College of Dental Medicine, Columbia University, New York, New York
Queries to the author regarding this course may be submitted to authorqueries@conexiant.com.
REFERENCES
1. Cortelli JR, Barbosa MD, Westphal MA. Halitosis: a review of associated factors and therapeutic approach. Braz Oral Res. 2008;22 suppl 1:44-54.
2. Olszewska-Czyz I, Sozkes S, Dudzik A. Clinical trial evaluating quality of life in patients with intra-oral halitosis. J Clin Med. 2022;11(2):326.
3. Settineri S, Mento C, Gugliotta SC, et al. Self-reported halitosis and emotional state: impact on oral conditions and treatments. Health Qual Life Outcomes. 2010;8:34.
4. Kahraman EN, Erensoy Ş, Dikilitaş A, et al. Awareness and knowledge of halitosis among students at two different dental universities in Turkey: a cross-sectional survey. BMC Oral Health. 2025;25(1):194.
5. van den Broek AM, Feenstra L, de Baat C. A review of the current literature on aetiology and measurement methods of halitosis. J Dent. 2007;35(8):627-635.
6. Silva MF, Leite FRM, Ferreira LB, et al. Estimated prevalence of halitosis: a systematic review and meta-regression analysis. Clin Oral Investig. 2018;22(1):47-55.
7. Barendregt JJ, Doi SA, Lee YY, et al. Meta-analysis of prevalence. J Epidemiol Community Health. 2013;67(11):974-978.
8. Rosenberg M, Kulkarni GV, Bosy A, McCulloch CAG. Reproducibility and sensitivity of oral malodor measurements with a portable sulfide monitor. J Dent Res. 1991;70(11):1436-1440.
9. Rösing CK, Loesche WJ. Halitosis: an overview of epidemiology, etiology and clinical management. Braz Oral Res. 2011;25(5):466-471.
10. Renvert S, Noack M, Lequart C, et al. The underestimated problem of intra-oral halitosis in dental practice: an expert consensus review. Clin Cosmet Investig Dent. 2020;12:251-262.
11. Faveri M, Trindade SC, Teles RP, et al. Halitosis: aetiology, diagnosis and management. Braz Oral Res. 2020;34(suppl 1):e087.
12. Salik A, Shaikh A, Gore A, et al. Prevalence of halitosis and its correlation with various intraoral etiological factors: a cross-sectional study. Ann Int Med Dent Res. 2016;2(5):20-24.
13. Hammad MM, Darwazeh AMG, Al-Waeli H, et al. Prevalence and awareness of halitosis in a sample of Jordanian population. J Int Soc Prev Community Dent. 2014;4(suppl 3):S178-S186.
14. Hussein H. Prevalence and risk factors of halitosis (oral malodor) among patients attending a dental school clinic in Egypt: a cross-sectional study. Advanced Dental Journal. 2022;4(3):207-215.
15. Yaegaki K, Coil JM. Genuine halitosis, pseudo-halitosis, and halitophobia: classification, diagnosis, and treatment. Compend Contin Educ Dent. 2000;21(10A):880-889.
16. Aydin M, Harvey-Woodworth CN. Halitosis: a new definition and classification. Br Dent J. 2014;217(1):E1.
17. AlBeshri S. Perspectives on tongue coating: etiology, clinical management, and associated diseases – a narrative review. Saudi Dent J. 2025;37(7-9):41.
18. Kleinberg I, Codipilly DM. Biology of the tongue coating and its role in oral malodor. Int Dent J. 2002;52(suppl 3):189-195.
19. Yaegaki K, Sanada K. Biochemical and clinical factors influencing oral malodor in periodontal patients. J Periodontol. 1992;63(9):783-789.
20. Haraszthy VI, Zambon JJ, Sreenivasan PK, et al. Identification of oral bacterial species associated with halitosis. J Am Dent Assoc. 2007;138(8):1113-1120.
21. Tonzetich J. Production and origin of oral malodor: a review of mechanisms and methods of analysis. J Periodontol. 1977;48(1):13-20.
22. Tangerman A, Winkel EG. Intra- and extra-oral halitosis: finding of a new form of extra-oral blood-borne halitosis caused by dimethyl sulphide. J Clin Periodontol. 2007;34(9):748-755.
23. Lee YH, Shin SI, Hong JY. Investigation of volatile sulfur compound level and halitosis in patients with gingivitis and periodontitis. Sci Rep. 2023;13(1):13175.
24. Nini W, Chen L, Jinmei Z, et al. The association between halitosis and periodontitis: a systematic review and meta-analysis. Clin Oral Investig. 2024;28(6):341.
25. Ratcliff PA, Johnson PW. The relationship between oral malodor, gingivitis, and periodontitis. A review. J Periodontol. 1999;70(5):485-489.
26. de Campos Kajimoto N, de Paiva Buischi Y, Mohamadzadeh M, Loomer P. The oral microbiome of peri-implant health and disease: a narrative review. Dent J (Basel). 2024;12(10):299.
27. Souza JPDV, Romero GDA, Melo Neto CLM, et al. Halitosis and pain threshold of peri-implant tissues: an observational cohort study. Braz Dent J. 2023;34(6):1-9.
28. Poli PP, Cicciu M, Beretta M, Maiorana C. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnosis, clinical implications, and a report of treatment using a combined therapy approach. J Oral Implantol. 2017;43(1):45-50.
29. Khounganian RM, Alasmari ON, Aldosari MM, Alghanemi NM. Causes and management of halitosis: a narrative review. Cureus. 2023;15(8):e43742.
30. Izidoro C, Botelho J, Machado V, et al. Revisiting standard and novel therapeutic approaches in halitosis: a review. Int J Environ Res Public Health. 2022;19(18):11303.
31. Tanasiewicz M, Hildebrandt T, Obersztyn I. Xerostomia of various etiologies: a review of the literature. Adv Clin Exp Med. 2016;25(1):199-206.
32. Popa M, Dinu S, Luca MM, et al. Salivary flow, tongue-coating burden, and morning breath odor: a cross-sectional study. J Clin Med. 2025;14(17):6072.
33. Memon MA, Memon HA, Muhammad FE, et al. Aetiology and associations of halitosis: a systematic review. Oral Dis. 2023;29(4):1432-1438.
34. Aguiar J, Gonçalves JL, Alves VL, Câmara JS. Relationship between volatile composition and bioactive potential of vegetables and fruits of regular consumption–an integrative approach. Molecules. 2021;26(12):3653.
35. Suzuki N, Nakano Y, Yoneda M, et al. The effects of cigarette smoking on the salivary and tongue microbiome. Clin Exp Dent Res. 2021;8(1):449-456.
36. Mokeem SA. Halitosis: a review of the etiologic factors and association with systemic conditions and its management. J Contemp Dent Pract. 2014;15(6):806-811.
37. Quirynen M, Dadamio J, Van den Velde S, et al. Characteristics of 2000 patients who visited a halitosis clinic. J Clin Periodontol. 2009;36(11):970-975.
38. Falcão DP, Vieira CN, Batista de Amorim RF. Breaking paradigms: a new definition for halitosis in the context of pseudo-halitosis and halitophobia. J Breath Res. 2012;6(1):017105.
39. Hucklenbroich P. “Disease entity” as the key theoretical concept of medicine. J Med Philos. 2014;39(6):609-633.
40. Aylıkcı BU, Colak H. Halitosis: from diagnosis to management. J Nat Sci Biol Med. 2013;4(1):14-23.
41. Coelho Dal Rio AC, Danielli Nicola EM, Franchi Teixeira AR. Halitosis—an assessment protocol proposal. Braz J Otorhinolaryngol. 2007;73(6):835-842.
42. Takeuchi H, Machigashira M, Takeuchi N, et al. The association of periodontopathic bacteria levels in saliva and tongue coating with oral malodor in periodontitis patients. Oral Health Prev Dent. 2017;15(3):285-291.
43. Rosenberg M, Septon I, Eli I, et al. Halitosis measurement by an industrial sulphide monitor. J Periodontol. 1991;62(8):487-489.
44. Seerangaiyan K, Jüch F, Winkel EG. Tongue coating: its characteristics and role in intra-oral halitosis and general health – a review. J Breath Res. 2018;2(3):034001.
45. Zhang Y, Lo KL, Liman AN, et al. Tongue-coating microbial and metabolic characteristics in halitosis. J Dent Res. 2024;103(5):484-493.
46. Amou T, Hinode D, Yoshioka M, Grenier D. Relationship between halitosis and periodontal disease – associated oral bacteria in tongue coatings. Int J Dent Hyg. 2014;12(2):145-151.
47. Rosenberg M, McCulloch CA, Bercy P, et al. Periodontal pockets and VSC production. J Periodontol. 2016;87:1234-1240.
48. De Geest S, Laleman I, Teughels W, et al. Periodontal diseases as a source of halitosis: a review of the evidence and treatment approaches for dentists and dental hygienists. Periodontol 2000. 2016;71(1):213-227.
49. Bollen CM, Beikler T. Halitosis: the multidisciplinary approach. Int J Oral Sci. 2012;4(2):55-63.
50. Fathi A, Rismanchian M, Dezaki SN. Effectiveness of different antimicrobial agents on malodor prevention in two-stage dental implants: a double-blinded randomized clinical trial. Eur J Dent. 2023;17(2):524-529.
51. Sreebny LM, Valdini A. Xerostomia. A neglected symptom. Arch Intern Med. 1987;147(7):1333-1337.
52. Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc. 2003;134(1):61-69.
53. Villa A, Connell CL, Abati S. Diagnosis and management of xerostomia and hyposalivation. Ther Clin Risk Manag. 2014;11:45-51.
54. Millsop JW, Wang EA, Fazel N. Etiology, evaluation, and management of xerostomia. Clin Dermatol. 2017;35(5):468-476.
55. Tangerman A, Winkel EG. Extra-oral halitosis: an overview. J Breath Res. 2010;4(1):017003.
56. Gokdogan O, Catli T, Ileri F. Halitosis in otorhinolaryngology practice. Iran J Otorhinolaryngol. 2015;27(79):145-153.
57. Singh VP, Malhotra N, Apratim A, Verma M. Assessment and management of halitosis. Dent Update. 2015;42(4):346-353.
58. Tangerman A, Winkel EG. Extra-oral halitosis: an overview. J Breath Res. 2010;4(1):017003.
59. Li Z, Li J, Fu R, et al. Halitosis: etiology, prevention, and the role of microbiota. Clin Oral Investig. 2023;27(11):6383-6393.
60. Lo K, Liman AN, Zhang Y, Ye W. Tongue coating metabolic profiles of intra-oral halitosis patients. Oral Dis. 2025;31(1):298-309.
61. Scully C, Porter S. Diabetes-associated halitosis. Oral Dis. 2018;24:456-462.
62. Oyetola OE, Owotade FJ, Fatusi OA, Olatunji S. Pattern of presentation and outcome of routine dental interventions in patients with halitosis. Niger Postgrad Med J. 2016;23(4):215-220.
63. Toyofuku A. Psychosomatic problems in dentistry. Biopsychosoc Med. 2016;10:14.
64. Quirynen M, Zhao H, van Steenberghe D, et al. Pseudo-halitosis: diagnosis and management. J Clin Periodontol. 2017;44:345-351.
65. Yaegaki K, Coil JM, Ooshima T, et al. Halitophobia: clinical evaluation. Oral Surg Oral Med Oral Pathol. 2016;122:210-216.
66. Aydin M, Bollen CM, Özen ME. Diagnostic value of halitosis examination methods. Compend Contin Educ Dent. 2016;37(3):174-178.
67. Szalai E, Tajti P, Szabó B,et al. Organoleptic and halitometric assessments do not correlate well in intra-oral halitosis: a systematic review and meta-analysis. J Evid Based Dent Pract. 2023;23(3):101862.
68. Froum SJ, Shi Y, Reis N, Asvaplungprohm T. A narrative review of the diagnosis, etiology, and treatment of halitosis over the past three decades. Compend Contin Educ Dent. 2022;43(5):E5-E8.
69. Laleman I, Dadamio J, De Geest S, et al. Instrumental assessment of halitosis for the general dental practitioner. J Breath Res. 2014;8(1):017103.
70. Seemann R, Conceicao MD, Filippi A, et al. Halitosis management by the general dental practitioner—results of an international consensus workshop. J Breath Res. 2014;8(1):017101.
71. Baharvand M, Maleki Z, Mohammadi S, et al. Assessment of oral malodor: a comparison of the organoleptic method with sulfide monitoring. J Contemp Dent Pract. 2008;9(5):76-83.
72. Greenman J, Lenton P, Seemann R, Nachnani S. Organoleptic assessment of halitosis for dental professionals—general recommendations. J Breath Res. 2014;8(1):017102.
73. Al-Qaydi SN, Saqan R, Al-Bluwi N, et al. Self-assessed and clinical halitosis among patients in the UAE: agreement and associated risk factors. Oral Health Prev Dent. 2025;23:785-792.
74. Löe H. Oral hygiene in the prevention of caries and periodontal disease. Int Dent J. 2000;50(3):129-139.
75. Pedrazzi V, Sato S, de Mattos Mda G, et al. Tongue-cleaning methods: a comparative clinical trial employing a toothbrush and a tongue scraper. J Periodontol. 2004;75(7):1009-1012.
76. Seemann R, Kison A, Bizhang M, Zimmer S. Effectiveness of mechanical tongue cleaning on oral levels of volatile sulfur compounds. J Am Dent Assoc. 2001;132(9):1263-1267.
77. Choi HN, Cho YS, Koo JW. The effect of mechanical tongue cleaning on oral malodor and tongue coating. Int J Environ Res Public Health. 2021;19(1):108.
78. Aung EE, Ueno M, Zaitsu T, et al. Effectiveness of three oral hygiene regimens on oral malodor reduction: a randomized clinical trial. Trials. 2015;16:31.
79. Veeresha KL, Bansal M, Bansal V. Halitosis: a frequently ignored social condition. J Int Soc Prev Community Dent. 2011;1(1):9-13.
80. Brookes ZLS, McCullough M, Kumar P, McGrath C. Mouthwashes: implications for practice. Int Dent J. 2023;73(suppl 2):S98-S101.
81. Peruzzo DC, Jandiroba PF, Nogueira Filho Gda R. Use of 0.1% chlorine dioxide to inhibit the formation of morning volatile sulphur compounds (VSC). Braz Oral Res. 2007;21(1):70-74.
82. Yeturu SK, Acharya S, Urala AS, Pentapati KC. Effect of aloe vera, chlorine dioxide, and chlorhexidine mouth rinses on plaque and gingivitis: a randomized controlled trial. J Oral Biol Craniofac Res. 2016;6(1):54-58.
83. Kim JS, Park JW, Kim DJ, et al. Direct effect of chlorine dioxide, zinc chloride and chlorhexidine solution on the gaseous volatile sulfur compounds. Acta Odontol Scand. 2014;72(8):645-650.
84. Porciani PF, Perra C, Grandini S. Effect of three different zinc lactate-added tablets on volatile sulfur compounds – a comparative study. Indian J Dent Res. 2025;36(3):299-302.
85. Manresa C, Sanz-Miralles EC, Twigg J, Bravo M. Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev. 2018;1(1):CD009376.
86. Manz F, et al. Hydration and health outcomes: evidence and review. Eur J Nutrition. 2020;60:1167-1180.
87. Torsten M, Gómez-Moreno G, Aguilar-Salvatierra A. Drug-related oral malodour (halitosis): a literature review. Eur Rev Med Pharmacol Sci. 2017;21(21):4930-4934.
88. Giannini L, Stella G, Cattaneo G, et al. Clinical applications of probiotics in pediatric dentistry and orthodontics – a systematic review. Nutrients. 2025;17(19):3153.
89. Yang Y, Ge J, Chen Y, Liu H. Efficacy and safety of probiotic therapy for halitosis: a systematic review and meta-analysis of randomized controlled trials. J Breath Res. 2025;20(1).
90. Wiench R, Fiegler-Rudol J, Zięba N, Misiołek M. Laser interventions for intraoral halitosis: a systematic review of randomized controlled trials. Pharmaceutics. 2025;17(8):1046.
91. Waikar VR, Pankey N, Lohe V. Laser therapy: an alternative approach for the management of halitosis. Cureus. 2024;16(7):e65911.
92. Mandetta ARH, Gallo JMAS, Ribeiro CDPV, et al. Comparative study of photodynamic therapy with LED and probiotics in the treatment of halitosis: protocol for a randomised controlled clinical trial. BMJ Open. 2025;15(4):e095544.
93. Motta PB, Gonçalves MLL, Gallo JMAS, et al. Short term effect of antimicrobial photodynamic therapy and probiotic L. salivarius WB21 on halitosis: a controlled and randomized clinical trial. PLoS One. 2024;19(7):e0297351.
94. Suh Y, Patel S, Kaitlyn R, et al. Clinical utility of ozone therapy in dental and oral medicine. Med Gas Res. 2019;9(3):163-167.
95. Van der Sleen MI, Slot DE, Van Trijffel E, et al. Effectiveness of mechanical tongue cleaning on breath odour and tongue coating: a systematic review. Int J Dent Hyg. 2010;8(4):258-268.
96. Erovic Ademovski S, Mårtensson C, Persson GR, Renvert S. The effect of periodontal therapy on intra-oral halitosis: a case series. J Clin Periodontol. 2016;43(5):445-452.
97. Boccia G, Di Spirito F, D’Ambrosio F, et al. Local and systemic antibiotics in peri-implantitis management: an umbrella review. Antibiotics (Basel). 2023;12(1):114.
98. Iranitalab M, Ouanounou A. Drug-related halitosis: a narrative review. Int Dent J. 2026 Jan 9:109332. 10.1016/j.identj.2025.109332.
99. Stoopler ET, Villa A, Bindakhil M, et al. Common oral conditions: a review. JAMA. 2024;331(12):1045-1054.