You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Characteristics and Comparisons
New technology has enhanced the durability and esthetics of bulk fill composites. Some have an unlimited depth of cure; others are limited. Some require a capping layer; others can be single increment fillings free of a cap. A variety of materials fit into the bulk fill category, but in general a bulk fill composite is placed in an increment greater than 4 mm and has a reasonable depth of cure. The benefit is that bulk fills are typically easy to use and save time compared to layering.
Traditional complaints against bulk fills were either depth of cure or improper curing, and marginal gaps leading to microleakage and secondary caries, due to polymerization shrinkage or poor adaptability of the composite into the cavity prep. Incremental layering therefore was advised for less stress and strain on the tooth, and avoidance of polymerization shrinkage resulting in better marginal adaptation, wear resistance, and shade matching.
In recent years, however, research by Veloso et al. shows there is no longer as much difference in polymerization shrinkage between layering and bulk fills, plus there is a greater chance of getting voids, knitting lines, and other deficits with layering composite.1
Maintaining proper isolation is critical when performing resin restorations, which can be achieved through the use of rubber dams, dry shields, and other isolation methods. The layering technique for resin restorations is more time-consuming and involves more steps, further emphasizing the importance of isolation. With significant recent changes in durability and improvements in bulk fills, some now outperform layering composites in terms of wear properties, polymerization shrinkage, compatibility with curing lights, and stress and strain on the tooth.
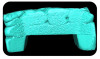
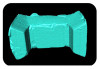
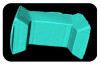
A 2020 Dental Advisor study compared incremental and bulk fill techniques.2 Figure 1a and Figure 1b show a poorly done incremental technique that resulted in knitting lines and voids within the composite. It is important that the resin is more radiopaque than the tooth structure, otherwise in this instance x-rays may appear to show interproximal carries but actually show a knitting line within the composite layer. With the bulk fill composite depicted in Figure 1c and Figure 1d, a snowplow technique was utilized, resulting in a more monolithic restoration where layers are homogenous with no gaps or voids.
The "snowplow" technique is when the practitioner applies a thin layer of flowable that serves as a liner on the dentin within the preparation but does not cure it. The practitioner then inserts bulk fill composite and sculpts, shapes, and cures it all at the same time, allowing for excellent marginal adaptation and a restoration that is free of voids and more structurally sound.
Regardless of the restorative technique and material, it is very important to select and use a proper matrix system to provide the contour, contact, and adaptation of the restoration. When performing the snowplow technique to restore a Class 2 cavity preparation, the fit and seal of the matrix system is critical to ensure that the material does not extrude out excessively and result in overhangs and too much flash.
Low Viscosity Flowables vs. High Viscosity Sculptables
Bulk fills fall mainly into two varieties: low viscosity flowables and high viscosity sculptables. A third option provided by one manufacturer is a unique, in-between composite with a mixed viscosity; a sonic handpiece vibrates and agitates the particle network to create a more flowable medium that has a fluffy, whipped cream kind of consistency that settles back into a more packable type composite.
While many bulk fill composites rely on curing lights for polymerization, some are dual or self-curing. Those that are either dual or self-curing require some type of activation, such as a dual barrel syringe/mixing gun, trituration, pre-placement of a catalyst primer/conditioner, etc. A benefit to these self-curing or dual-curing bulk fills is an unlimited depth of cure, however sometimes the delivery system may not be as ideal or precise as the clinician may prefer.
Low viscosity flowables are typically highly filled, tend to be more translucent, and have a self-leveling characteristic or ability. Most require a capping layer for improved durability and wearability of the overall restoration. A benefit to a flowable is excellent adaptation to the preparation walls and margins. Depth of cure could be greater for some bulk fill flowable resins but is usually limited to around 4 mm to reduce the amount of polymerization shrinkage and stress. Due to the filler content, low viscosity flowable bulk fills generally have a more limited depth of cure than high viscosity sculptables, which are firmer and can be "packed in."
Low viscosity flowables are often used for deep bases. The advantages are fast and easy placement, good marginal adaptation, and low modulus to reduce shrinkage during curing. The disadvantages are high volumetric shrinkage, lower filler load resulting in low wear resistance and high translucency, limited depth of cure
(4 mm on average), and a capping layer usually required for the final occlusal layer.
In small conservative preparation designs they can do quite well without a capping layer, but if they are going to be subjected to heavy load or incisal shearing forces, a capping layer is required. At a minimum, the capping layer needs to be approximately 2 mm in thickness to withstand occlusal forces.
Because low viscosity flowable bulk fills tend to be translucent, the transition from the flowable bulk fill to the capping layer may be seen. This needs to be taken into consideration in situations where the filling will be visible in a patient's smile, such as the mesial surface of a maxillary premolar. Practitioners should also be mindful of the following situation: When a patient is reclined, gravity can cause flowable material to sag backward, leading the practitioner to believe there is enough space for a
2 mm capping layer. However, upon adjusting the occlusion, they may discover that the layer is too thin, which could result in restoration failure.
Flowable composites are susceptible to having air bubbles and voids within the material, but some manufacturers manage to avoid this by centrifuging their composites so that any trapped air does not appear until the end.
Sculptable bulk fill composites on average have a higher depth of cure of about 4 mm or greater. They usually have better esthetics and wear because they are not as translucent and have a higher filler content. But they usually do not have as good adaptation as flowable composites, which could result in marginal gaps and decay, so the practitioner would have to use a liner or base to avoid this.
Manufacturers of composites have simplified shade matching, allowing practitioners to reduce overhead; in general these materials are easy to work with and are good looking, durable, and work and wear well.
Extensive data has been compiled on bulk fill composites.3-6 Not all are created equal due to particle size and shape and filler content, which play a part in esthetics, handling, durability, and wear. When there is proper depth of cure and curing, hardness of the restoration and the polymerization are increased.
Proper curing with a curing light is a crucial step in adhesive dentistry, and tools are available to help ensure this is being achieved. Depending on the practitioner's curing light, its power, and materials' depth of cure, curing times can range significantly.
The wear rate also is vital, and some manufacturers' products have better longevity than others. And while initial gloss and long-term gloss retention may not seem important, particularly for posterior teeth, gloss still should be attended to as it can be compromised through a patient's diet, chewing, and brushing, diminishing its appearance. Choose a bulk fill composite that has a good natural look with blendability and staining resistance as well as good wear characteristics and functionality.
Additional studies also compared bulk fill composites concerning flexural strength, shrinkage stress, and fracture toughness.3-6 Different composites, even those from the same manufacturer, can have varying shrinkage and stress percentages, flexural strengths, fracture toughness, and wear resistance. Composites also have different depths of cure and can be sensitive to the duration and power output of the curing light, all of which may ultimately impact the integrity of the restoration. The type of curing light may result in greater or lesser depth of cure, and quicker or slower cure as well. Choose a composite and a curing light that do not lead to too much polymerization shrinkage and not enough curing.
Radiopacity is also an important quality in a composite. When looking at a radiograph, the practitioner must be able to determine what is tooth structure, what is restorative material, and what is decay. Materials that are radiolucent or not radiopaque are not recommended. If there was a knitting line without increased radiopacity, the practitioner might think that there is a Class 2 lesion. Or if the composite is radiolucent, it will be difficult for the clinician to determine the presence of decay.
Restorative Cases Utilizing Advanced Bulk-Fill Technology
Bulk fills that do not require a capping layer are available from several companies, including 3M, DMG, Kerr, Kulzer, and Tokuyama. This article will focus on three that the author is most familiar with. 3M offers a bulk fill that does not require a capping layer and has a 5 mm depth of cure and increased opacity for better esthetics.7-9 Many bulk fills can be too translucent, so if a practitioner has to do a restoration behind an amalgam in a tooth or is replacing it, and if there is staining from decay or the previous restoration, if a bulk fill is not opaque enough, there could be shadows and inferior aesthetics. This company reports its bulk fill has a unique monomer to reduce shrinkage and shrinkage stress, which is why it allows for a 5 mm depth of cure. It comes in five shades and can be warmed up to 70 degrees F or 158 degrees C for up to one hour. Warming can make it more adaptable and sculptable for good marginal adaptation, but it should not be warmed to too high of a temperature, nor for more than one hour.
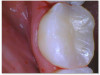
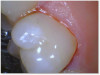
Figure 2 shows what is seen when the bulk fill is used to replace amalgams; while it sculpted well, there was a little bit of show-through from a previous amalgam discoloration, and one can see a white line possibly due to polymerization stress shrinkage or it is a bit of flash; perhaps a deeper bevel was needed to avoid this. Sometimes with the more simplified shade composite systems, if a bit of flash overlays the enamel after polishing, a white line can form. Not knowing the exact cause of the white line-flash or polymerization shrinkage-can be a source of concern for the practitioner as it could result in microleakage and failure if it is due to shrinkage.
Another company, Kerr Dental, has a bulk fill packable and bulk fill flow one-shade composite system that offers improved rheological properties, handling, durability, and lower shrinkage stress. With one-shade adaptive color blending, the bulk fill, in the author's experience, blends well and looks natural. It comes in both unidose carpules and reusable syringes, and it offers a 5 mm cure. The bulk fill flow does require a capping layer, which can be the company's packable bulk fill or another composite of the practitioner's choosing. It is up to the practitioner to decide which bulk fill technique they prefer to use, flowable and/or packable bulk fill composite, which allows flexibility for different case scenarios. The bulk fill flow has a self-leveling effect that easily adapts to the preparation walls and does not slump. The third generation of proprietary technology in the packable composite,
in the author's experience, allows for better handling and essentially offers two viscosities in one. If the practitioner has a light touch and brushes the composite it will spread well, but if the practitioner likes to condense it the composite will provide firm feedback, allowing it to be packed into the tooth and sculpted without having to heat it up and without needing a special handpiece. In the author's experience, it offers superior shade matching and esthetics, adaptability, and durability.
Figure 3a and Figure 3b show a failing composite with stress fractures and interproximal decay. The patient was not in a situation to do an indirect restoration, so the practitioner did a direct composite with good strength and wear characteristics until an indirect restoration could be performed. The composite used in this case is the Kerr SimpliShade Bulk Fill Packable, which in the author's experience also offers good blendability and polishability with good adaptation. Some of the discoloration interproximally is from the bleeding after the rubber dam was removed-which quickly self-resolved.
Figure 4a through Figure 4e show the technique using a bulk fill flow with a bulk fill capping layer. There was a carious lesion on tooth No. 19 requiring a deep excavation of decay close to the pulp and cotton roll isolation. Practitioner did an indirect pulp cap using a light curable bioactive syringeable flowable that can be used for direct and indirect pulp capping, and then applied a layer of the bulk fill flow, which offered a good glossy appearance without polishing. Kerr SimpliShade Bulk Fill Flow and Bulk Fill Packable were used. Although most bulk fill flows are transparent, this one successfully blocks the white opaque resin-modified calcium silicate filled liner (Bisco TheraCal LC). The practitioner used bulk fill packable (Kerr SimpliShade Bulk Fill) as the capping layer in a single increment. In the author's opinion, this single shade bulk fill system offers excellent esthetics and gives an outcome similar to layering. The patient reported no post operative sensitivity or discomfort after the restoration was performed.
In another case, bulk fill work was done on a Class 5 restoration with a single shade system (Figure 5a and Figure 5b). While one expects more ideal characterization in a system that has more than one shade, this one-shade composite worked very well to blend and match the natural characteristics of the tooth.
Figure 6a through Figure 6d show a procedure using a bulk fill packable as an interproximal Class 2, without using a bulk fill flow and not done with the snowplow technique to see how well the composite adapted to the margin. A light curable resin-modified calcium silicate liner (Bisco TheraCal LC) was used to perform an indirect pulp cap. A packable bulk fill composite was applied as a single increment layer to successfully restore the tooth. The material (Kerr SimpliShade Bulk Fill Packable) provided good adaptation to the tooth without gaps or polymerization stress lines and demonstrated great polishability and blendability. The patient reported no post operative sensitivity or discomfort in the 9 months after the restoration was performed. Sensitivity can be a concern if a composite is subjected to too much polymerization shrinkage.
Also shown is a conservative Class 2 prep (Figure 7a through Figure 7c). Even though the restorative material is a single shade composite, it still managed to block out the amalgam from showing through from the adjacent tooth.
Tokuyama offers a bulk fill flowable within its Omnichroma line of composites. It does not require a capping layer, but its depth of cure is limited to 3.5 mm, so the practitioner must be very aware of this measurement to avoid problems. This product can be used as a bulk fill, but multiple layers might be required depending on the size of the cavity preparation. It has one shade, low viscosity, good opacity, and can be used in all cavitie classifications in the anterior or posterior and can be used as a base or a liner.
Nonetheless, at this time it is widely understood that flowable bulk fill composites when used without capping layers do not perform well in large cavity preparations that involve replacing cusps or incisal edges, and therefore should be utilized within their limits or avoided in such situations.
Tokuyama has put together some comparative data on its product, which exhibits a slightly higher degree of shrinkage compared to its Omnichroma packable composite, but less than its Omnichroma flowable (non-bulk fill). Additionally, this product boasts a higher compressive strength than both.10-12 The product tends to have a milkier, opaque look, and is convenient to use where a packable, or a capping layer, are contraindicated, allowing use of a flowable in small cavity preparations.
Figure 8a and Figure 8b show a terminal abutment with proximal decay from a removable cast metal partial denture. The tooth had an existing large resin restoration that was otherwise stable and the decay was isolated to the mesial surface. The patient had limited funds, and while a crown was presented as a restorative option, the patient elected to restore the tooth with a direct restoration at the time. The composite used was the Tokuyama Omnichroma. The practitioner excavated the decay and much of the filling. In this scenario, using a flowable bulk fill with self-settling and blendable properties that also does not require a capping layer, proved advantageous in restoring the tooth's contour, making it easy to retrofit the RPD.
Wear, Curing Light Use, and Polishability
The August 2023 issue of Inside Dentistrycontains much information about bulk fill wear and curing light use.13,14 Tariq and Sulaiman looked at bulk fill total wear and mechanical stress, experimenting with adding heat and moisture to emulate the oral cavity environment, and compared various restorative resin materials to natural enamel. Price and Sullivan examined curing lights and expanded on the core principles to light curing; Price also earlier did a similar examination in the Dental Advisor.2
As mentioned earlier, with bulk fills or any composites, depth of cure is crucial. A high-powered curing light is necessary but produces heat, and excessive heating of the pulp is contraindicated. Therefore, depending on the curing light, it is advised to break up curing cycles into 10-second intervals, waiting a few seconds in between. Moreover, aim the curing light not just from the occlusal but from the buccal and lingual surfaces as well, and cure all the way through. Have a direct, straight-on beam of light to avoid shadows, especially in Class 2 situations.
The optical lens diameter and beam collimation of the curing light dictate the homogenous energy distribution for a more complete and deeper cure. The output from the curing light should be consistent, stable, and uniform throughout the tip. It is recommended to use a 10- to 12-mm active optical diameter when curing larger bulk fill composite restorations and curing beneath indirect restorations, as the entire tooth is being cured at one time. Whereas a 7- to 8-mm active optical diameter for layered composite restorations is sufficient, because the tooth is being repeatedly cured with each incremental application of composite. Good beam collimation that can deliver high radiance up to 10 mm away from the tip is vital, because the light should not touch the tooth or resin.15
Once the restoration has been properly placed, the practitioner shifts focus to contouring, finishing, and polishing. The Dental Advisor did a study on one-step, two-step, and three-step polishers.16 Some one-step polishers do nearly as good a job as two-step or three-step polishers. This is due to many factors-for example, some polishers are impregnated with polishing paste that makes it easier to achieve a high final shine in fewer steps.
Many of the new spiral polishers work really well at adapting to the contours of the tooth to provide a nice polish; however, thicker spiral polishers do not do this as well but do provide much greater durability. Single-use and multi-use polishers are available to meet the various wants and needs of practitioners. Several options exist for polishing composite, ceramic, as well as other substrates. It is important to match the polishing system to the surfaces and substrates to which it will be applied, so that the polisher will be abrasive enough to polish the surface without damaging it. Clinician's Choice offers A.S.A.P. polishers, a two-step polishing system that can be used on any surface and substrate. (Other companies offering polishers include 3M, Brasseler, Ivoclar, Meisinger USA, and SS White.) Polishers are used up more quickly on ceramic, so if a lot of ceramic polishing is required, an indirect polisher is indicated.
Dr. Lawson of the University of Alabama at Birmingham studied the gloss of composites with the use of several spiral polishers and found that while there was not much difference in the level of the gloss achieved in the pre-polish phase, there was a big difference in the level of the final high-shine polish phase, as well as a significant difference in the time needed to achieve these various levels of gloss.3 Practitioners should remember not to run the polisher at too high a speed and to use intermittent water to avoid heating the tooth as well as avoid buildup of residue from the polishers.
Conclusion
Shade matching bulk fill composites simplify the shade selection process and inventory needed by seamlessly blending to a wide range of tooth shades. Bulk fill composites save time and are an efficient way to fill and cure large restorations. Their versatility allows them to be used in a variety of dental applications, from direct restorations to core buildups. While these composites simplify shade matching and are convenient to use, it is important to understand their long term esthetics, wear resistance, and durability. Esthetics no longer need to be compromised for convenience, and utilizing bulk fill resins promotes efficiency and allows for less inventory without compromising care.
About the Author
Matthew R. Miller, DDS
Reimels, Miller, Paterra Family and Cosmetic Dentistry
13605 Reese Blvd. West
Huntersville, NC 28078
(704) 948-1111
drmiller@dentaladvisor.com
References
1. Veloso SRM, Lemos CAA, de Moraes SLD, do Egito Vasconcelos BC, Pellizer EP, de Meolo Monteiro GQ. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: a systematic review and meta-analysis. Clin Oral Invest.2019;23(1):
221-223.
2. Price R. Curing lights. Dental Advisor. https://www.dentaladvisor.com/issues/v-37-n-02/. 2020;37(2).
3. Lawson N. Gloss of Composites With the Use of Several Polishers. Birmingham: University of Alabama at Birmingham, School of Dentistry; 2022.
4. Sengupta A, Naka O, Mehta SB, Banerji S. The clinical performance of bulk-fill versus the incremental layered application of direct resin composite restorations: a systematic review. Evid Based Dent.2023;24(3):143.
5. Yazici AR, Kutuk ZB, Ergin E, et al. Six-year clinical evaluation of bulk-fill and nanofill resin composite restorations. Clin Oral Invest. 2022;26:417-426.
6. Atabek D, Aktaş N, Sakaryali D, Bani M. Two-year clinical performance of sonic-resin placement system in posterior restorations. Quintessence Int. 2017;48(9):
743-751.
7. Opdam NJM, Roeters JJM, Peters TCRB, Burgersdijk RCW, Teunis M. Cavity wall adaptation and voids in adhesive Class I restorations. Dent Mater.1996;12(4):230-235.
8. Opdam NJM, Roeters JJM, Joosten M, Veeke OV. Porosities and voids in Class I restorations by six operators using a packable or syringable composite. Dent Mater.2002;18(1):58-63.
9. Bouschlicher M, Rueggeberg FA, Wilson BM. Correlation of bottom-to-top surface micro hardness and conversion ratios for a variety of resin composite compositions. Oper Dent.2004;29(6):698-704.
10. Paravina RD, Westland S, Imai FH, Kimura M, Powers JM. Evaluation of blending effect of composites related to restoration size. Dent Mater.2006;22(4):299-307.
11. Sanchez NP, Powers JM, Paravina RD. Instrumental and visual evaluation of the color adjustment potential of resin composites. J Esthet Restor Dent.2019;31(5):465-470.
12. Lee YK, Lu H, Oguri M, Powers JM. Changes in gloss after simulated generalized wear of composite resins. J Prosthet Dent. 2005;94(4):370-376.
13. Tariq A, Sulaiman T. Wear behavior of contemporary direct resin-based restorative materials. Inside Dentistry. 2023;19(8):16-18.
14. Price R, Sullivan B. Selecting a Dental Light Curing Unit. Inside Dentistry. 2023;19(8):30-37.
15. Strassler H. Light Curing 101. Incisal Edge.https://www.incisaledgemagazine.com/mag/article/light-curing-101/. Accessed February 9, 2024.
16. Translating the science: comparison of gloss of zirconia finished and polished with various popular polishing systems. Dental Advisor. https://www.dentaladvisor.com/pdf-download/?pdf_url=wp-content/uploads/2016/06/TTS30-Gloss-Measurements-1A-B-06-03-16_V2.pdf. Published April 2016 No. 30a. Accessed February 9, 2024.