You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Among the most commonly used dental materials since their introduction in the 1960s,1 flowable resin composites are restorative materials with excellent esthetics, offering enamel shades that are highly similar to those of natural teeth, and which have an improved ability to bond with enamel and dentin compared with amalgam or glass ionomer, affording less loss of structure during tooth preparation.2Despite their advantages, flowable resin composites had for many years some limitations related to mechanical properties, including poly- merization shrinkage, shrinkage stress, and limited depth of cure,3 that limited their applicability. Consequently, these materials have generally been reserved for restorations with minimal occlusal loading, such as liners, small class I and II cavities, and class V lesions.4 However, in recent years, developments in filler technology, with enhanced polymers and fillers, have led to substantial improvements in the mechanical properties of flowable resin composites, particularly with regard to their wear resistance.5
In the same way that Buick needed to redesign their auto- mobiles to meet performance and esthetic demands of the younger buyer, dental manufacturers have found it necessary to reformulate flowable composites to overcome the image of poor physical properties. That image emerged with a product called "Paint On Resin" (Kuraray Corp) more than 40 years ago. Dubbed the "First Flowable", it was possible to utilize it to "weld" together sections of full-mouth temporary restorations intraorally, although it was not a good choice for use in a load-bearing, highly abrasive posterior area. Still, the attraction of being able to inject a light-cured polymer could not be diminished; the flowable composites needed to be enhanced with better polymers and fillers.
While improvements in the filler technology of flowable composites were emerging, heating of universal and bulk fill composite pastes (at 40°C to 50°C) was being utilized to facilitate the injection of these materials into cavities. One objective of this approach is to lower surface tension and thus potentially achieve better adaptation. With this process, packing after injection is necessary, which can be challenging. In addition, heaters can be costly. Compule heater guns work well, but their size and configuration can be ergonomically challenging, especially in the molar area. The "pause factor" creates a further problem; unless the clinician is using the self-heating compule heater gun, the heat and flowability are quickly lost when compules are out of the base heater. These challenges and concerns have made a room- temperature flowable composite with posterior occlusal accommodating physical properties desirable.
This article describes the various advancements made in flowable composites, particularly some of the new dual-cured bulk-fill composites, that have allowed for their applicability in load-bearing, highly abrasive areas, such as the posterior teeth.
BULK-FILL FLOWABLE COMPOSITES
Bulk-fill composites are direct restorative materials intended for use in 4- to 5-mm+ increments.6 These composites have been developed as both flowable and conventional/sculptable viscosities to help provide ease of application.7 Bulk-fill composites differ from traditional composites in that they are intended to overcome the time-consuming process of incremental layering as well as gaps formed between layered large restorations. Light-cure-only composites strive to accomplish this through low-shrink oligomers combined with greater light transmissibility (for depth of curing); however, there are limits to the ability to achieve this in a "fast" light polymerization kinetic reaction. Ideally, bulk-fill composites are able to achieve single-step filling of large restorations, without compromises such as increased polymerization shrinkage or inadequate depth of cure, while maintaining flowability sufficient to ensure filling of gaps and voids. Lastly, an ideal bulk-fill composite would possess good polishability and wear resistance, to achieve an esthetic and durable occlusal surface of the restoration.8
FILLER LOAD, VISCOSITY, AND POLYMERIZATION SHRINKAGE
Increased filler load can improve the resistance to functional wear, while viscosity increases with increased filler loading. Generally, flowable resin-based composites have filler loading reduced to 37% to 53% (volume) compared with 50% to 70% (volume) loading for paste types, less viscosity, and thus better adaptability with the cavity wall, albeit at the expense of wear resistance.9
Polymerization shrinkage, which is one of the most impor- tant causes of failure of composite restorations,10,11is reduced when structural fillers occupy space that would otherwise consist of polymerizable monomers/oligomers. The correlation between increased filler loading and viscosity limits the extent to which polymerizable components can be replaced while still having a material that is clinically usable for creating restorations. Recently, new filler types such as nanoclusters have provided a means of further increasing filler loading beyond what is achievable with traditional fillers (within the bounds of acceptable viscosity). By using multiple particle sizes, which are partially fused into clusters, manufacturers have been able to increase the total filler loading of flowables into the 65% range, comparable to sculptable composites, without the expected dramatic increase in viscosity (Nick Aralis, Director of Research and Development, Zest Dental Solutions/Danville Materials, Carlsbad, CA; written communication, February 2023).
DEGREE OF CONVERSION AND DEPTH OF CURE
A lower degree of conversion achieved during polymerization is associated with inferior mechanical properties and poor wear resistance of composites.11
Depth of cure depends on filler type, size, and loading, among other factors.8 Polymerization kinetics and their depth variation for dual-cured bulk-fill composites are material dependent.12In Wang et al's study of polymerization kinetics in dual-cured and light-cured bulk-fill composites, two dual-cured composites exhibited faster polymerization kinetics at the 0.5 mm depth than at the 5.0 mm depth, whereas another dual- cured bulk-fill composite possessed moderately paced kinetics at both the 0.5 mm and 5.0 mm depths.12This could account for its uniform depth of conversion, as shown in Figure 1 (J. Ferracane Oregon Health & Science University School of Dentistry; unpublished data, 2022).
Another study revealed that dual-cured bulk-fill composites did not reduce gaps in margins compared with light-cured bulk-fills.6However, in a presentation at the IADR general session in San Francisco in 2017, Dr Michael Miller showed that with one bulk-fill composite, gap reduction was accomplished simply by using a 19-gauge needle as opposed to a 17-gauge needle. The percent of voids at margins went from 0.168 to 0.017, a significant reduction.13 In an additional report, Dr. Alireza Sadr used optical coherence tomography analysis to determine gap formation of five composites (Sadr A. Performance of an improved dual cure bulk-fill composite in adaptation under high C-factor. University of Washington School of Dentistry; unpublished data, 2022). The dual-cured bulk-fill composite had 100% adaptation to the cavity floor and no gap formation in a high C-factor preparation (Figure 2 and Figure 3). A light-cured bulk-fill composite, on the other hand, had 100% separation, most likely due to its self-etching/self-adhesive light- cured formulation (Figure 4).
Windle et al studied the effect of light on the dual-cured bulk-fill composite's self-cure aspect.14The dual-cured composites were also compared with a purely light-cured bulk-fill and universal incremental composite. The composites were irradiated in one direction in an opaque mold. In addition, the dual-cured composites were left to self-cure without irradiation. Vickers Hardness (VHN) was measured up to 6 mm of depth. Hardness dropped significantly with depth in light-cured composites and in all but one of the dual-cured composites. Self-cured dual-cured composites achieved constant hardness throughout their depths. Only one of the dual-cured composites was unaffected by curing mode, whereas in two other dual-cured composites, low- density light levels interfered with self-polymerization. Among the dual-cured composites that received photoactivation, higher surface hardness was a shared characteristic, but depth of cure was product-dependent in this study.14Irradiation grossly affected the middle sections of two dual-cured bulk-fill composites, but one dual-cured bulk-fill flowable composite was unaffected in the middle section.
Wang et al looked at three new dual-cured bulk-fill resin- based composites compared with light-cured bulk-fill composites.15The clinically relevant depths of 0.5 mm and 5.0 mm were used as the two levels of measurement. Irradiation for 20 and 40 seconds was utilized to ascertain degree of conversion (DC) and VHN. Self-cure was also evaluated for the dual-cured resin-based composites. All specimens showed significantly higher values at the 0.5 mm level than the 5.0 mm depth, with the exception of one of the dual-cured bulk-fill flowable composites, which showed similar DC and VHN values at both levels, indicating that it is a more forgiving material. All three dual-cured composites showed higher DC and VHN than the three pure light-cured composites under the same conditions. Twenty- versus 40-second curing made no difference for the three dual-cured materials at either depth. There was a significant difference in DC and VHN with two of the light-cured composites at the 5.0 mm depth with the 40-second irradiation versus the 20-second cure. In terms of uniformity in the bottom layer, dual-cured were superior to light-cured composites. The authors concluded that the new dual-cured bulk-fill flowable composites show promise for uniform degree of conversion and microhardness throughout the depth of direct restorations.15
COMPOSITION OF BULK-FILL COMPOSITES
Some bulk-fill composites contain zirconia and silica particles. One bulk-fill composite includes nano-zirconia in its formulation. Utilizing nanoclusters of zirconia in an agglomeration process has been found to greatly enhance the physical properties of composites16; plucking of large particles can be eliminated without compromising the anti-crack propagation afforded by large particles (J Ferracane. Oregon Health & Science University School of Dentistry; unpublished data, 2022). In this bulk-fill composite, 4-nm zirconia particles are electrostatically fused to 80-nm silica particles, which are then clustered and ground through a high-precision grinder to form more uniform cluster sizes. This process and the specific fillers used in this composite allow for higher filler load than in other composites using different zirconia nanoclusters,17 as well as higher wear resistance and gloss retention compared with traditional fillers (Nick Aral- is, Director of Research and Development, Zest Dental Solutions/Danville Materials, Carlsbad, CA; personal communication, February 2023).18 Zirconia nanoclusters have also been shown to produce better blending with surrounding tooth structure in composites.19
APPLICATION OF THE BULK-FILL COMPOSITE: SPECIAL CONSIDERATIONS
When applying the dual-cured bulk-fill composite, a slight overfill of the cavity prep is important, as stress relief of bonded walls and pulpal floor occurs at the expense of the nonbonded occlusal surface. Auto- and dual-cured composites can be used to mitigate polymer stress in high C-factor restorations and thus prevent pain from pulpal floor gapping postoperatively as well as recurrent caries due to micro-gapping at margins. Dual-cured flowable composites have limited ability to hold a matrix band closely apposed to an adjacent tooth. Consequently, it is critical in developing tight proximal contacts to wedge the teeth prior to preparation of the cavity. This is called prewedging (depicted in Figure 5). Another important consideration is the type of ring, wedge, and matrix employed. The wedge must close off the base of the well-fitting matrix band to prevent overhangs. The separation force of the ring is critical to ensure a good contact with the adjacent tooth. Nate Lawson at UAB found that 28 N was the best measured by Instron, while other researchers claim that 8 pounds measured by removal of ring with forceps is the optimal separation force. Another consideration in selection of the ring and wedge is the amount of separation force generated by these devices. Dr David Clark has discussed that "tack welding" the band to the buccal and lingual of the tooth with flowable composite can be accomplished by holding the band in close opposition to the adjacent tooth with either a matrix adjusting instrument (Bioclear™ Push-Pull, Bioclear Matrix Systems) or contact-forming instrument (Contact Pro, CEJ Dental) (alternatively: Perform Contact Former, Practicon Dental) (David Clark, DDS, personal communication, December 7, 2022). This does involve using an assistant to light-cure the tack weld; however, it is guaranteed to generate a tight contact (Figure 6 and Figure 7).
CASE REPORTS
Case Study 1
A 77-year-old male patient presented in the author's AEGD Residency Program clinic with a chief complaint of sensitivity in the maxillary right posterior area. He had an unremarkable health history, and after a thorough examination, he was presented with several treatment options: minimally invasive drill access, performed laterally, filled with glass ionomer (poor prognosis); distal occlusal composite resin with an occlusal approach (preexisting occlusal resin apparent); or a distal occlusal ceramic onlay. The patient chose the first option of restoration with glass ionomer.
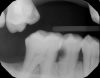
Figure 8A is a radiograph revealing deep root caries previously restored temporarily by a resident at the AEGD Residency Program clinic with glass ionomer utilizing a lateral rather than occlusal approach. After the glass ionomer failed to adhere, another resident again attempted a lateral approach that resulted in the restoration shown in Figure 8B. A third resident had success with an occlusal approach, removing a failed occlusal composite to access the distal (Figure 9). This attempt was successful both in the preparation of the lesion and in the placement of a dual- cure bulk-fill flowable (Bulk EZ Plus, Zest Dental Solutions; alternatively: HyperFIL®, Parkell; Fill-Up!, Coltene) extruded through a bendable needle (Figure 10). Figure 11 shows the final preparation after tissue removal was accomplished with rotary gingitage; note that this was performed with the rubber dam in place. An air abrasion device (Groman Etchmaster, Groman Dental; alternatively: PrepStart™ H2O, Zest Dental Solutions; Bioclear Blaster, Bioclear) was used with potassium bicarbonate to remove biofilm prior to acid etching (Figure 12). Phosphoric acid 37% was utilized in a total etch fashion (Fig- ure 13 and Figure 14) for 20 seconds. Figure 15 shows the universal bond (Scotchbond™ Universal, 3M; alternatively: All-Bond Universal®, BISCO; Prelude One, Danville Materials) with metha- cryloyloxydecyl dihydrogen phosphate (MDP) being scrubbed into the cavity for 20 seconds. After air thinning for 20 seconds, the adhesive was light cured for 40 seconds at 1,200 mw/cm2power density (Figure 16).
Respecting the inverse square law, the resident doubled the light-curing time to ensure good adhesive polymerization in the deep box. To facilitate the matrix band providing deep access (Paraband, Practicon; alternatively: Greater Curve matrix band; Greater Curve), the clinicians needed to remove the dam. Assurance of a dry field was accomplished by placement of bilateral dry angles that stem saliva flow from Stensen's ducts. A swedopter device was placed under the tongue to suction saliva from the sublingual and submandibular glands. Figure 17 shows the gingival area closure accomplished with the Paraband "Elizabethan collar effect"; no wedging is possible, so this Tofflemire type band provides a tight gingival seal by virtue of the band's unusual geometry. In Figure 18, the comfort of injection of the dual- cured bulk-fill flowable utilizing the bendable 20-gauge needle can be noted; it would not be possible to fill this with a paste-type universal composite. Subsequent to a 90-second self-cure phase during which the surface cannot be disturbed, the resident placed starting pits in the mesial central and distal pit areas with the medium acorn of the Occlusinator PRO bur system (StraussUSA; alternatively: R.A.P.T.O.R. Acorn, Henry Schein) (Fig- ure 19). Figure 20 shows the pits created at uniform depth facilitated by the limit stops on the burs. The acorn now is moved in a pit-to-pit pattern that created the planes that form the triangular and oblique ridges as well as the marginal ridges (Figure 21). After the planes were formed, a X-mas tree-shaped diamond bur was used to refine and prepolish the planes formed by the acorn (Figure 22). Refinements such as secondary anatomy can be placed using the mini-acorn (Figure 23). Figure 24 shows a Brownie polisher reshaped to a straight-sided X-mas tree bur that is used to polish the planes, pits, and ridges. In Figure 25, a Greenie polisher is shown that also has been reshaped to be a straight-sided X-mas tree polisher. Both are used at 50,000 to 100,000 rpm and with a copious water spray. Final polish is accomplished with a latch bristle brush coated with TopDotz polishers (Dental Ventures of America; alternatively: Shammy Bright™ Composite Polishing Paste, Kerr Dental) (Figure 26). As shown in Figure 27, the pure diamond comes in pellet form to facilitate good asepsis. The last polish is applied with a dry latch-type cotton buff (Figure 28). In Figure 29, note the anatomy formed by this technique. It is apparent that this resident accomplished a more than satisfactory result, as evidenced by the post-treatment radiograph (Figure 11).
Case Study 2
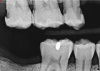
A 42-year-old male patient with a unremarkable health history presented in the AEGD Residency Program clinic with a chief complaint of pain in the mandibular right posterior area. Fig- ure 30 shows an unremarkable occlusal view of tooth No. 29; however, the radiograph showed deep distal caries near the root canal (Figure 31). Several treatment options were discussed with the patient, including extraction, root canal therapy, post and crown, and a distal occlusal composite that would later serve as a "margin elevation" material following endodontic therapy and preparation for a distal occlusal ceramic inlay or onlay. The patient chose the latter option.
A deep distal occlusal preparation was performed and a matrix band (Paraband, Practicon) was placed again, such that no wedge needed to be placed (Figure 32). The Groman Etchmaster was utilized to remove biofilm as previously shown in Figure 12. A total etch technique with 37% phosphoric acid was employed (Figure 33), and after thorough rinse and damp dry, a universal adhesive (Scotchbond™ Universal, 3M) with MDP was applied and light-cured 40 seconds at 1,200 mw/cm2 due to the depth of the box form (Fig- ure 34). Figure 35 shows the dual-cure bulk-fill flowable composite (Bulk EZ Plus, Zest Dental Solutions) being injected into the deep box with a 20-gauge bendable needle. It is important to keep extrusion pressure on the plunger while withdrawing the needle to prevent bubbles or voids in the composite interface with the tooth structure. Overfilling by approximately 10% and smoothing the surface only with brushes promotes good marginal seal (Fig- ure 36). It is critical to not disturb the occlusal surface of any dual-cure bulk-fill flowable with an attempt to "soft sculpt," as that may create marginal voids.
After this dual-cure flowable's obligatory 90-second self-cure, hard sculpting with burs can begin. The Occlusinator PRO bur set (StraussUSA) was used to rapidly sculpt in planes after anatomical pits are placed at the depth of the limit stops on the burs; the clinician will appreciate the safe edges of the acorns and the safe zones on the X-mas tree burs. Figure 37 shows the medium acorn with a 50-micron diamond placing a pit where the distal marginal pit should be. It is apparent in Figure 38 that the limit stop on the acorn prevents cutting starting pits too deeply.
The safe-zoned X-mas tree with 15-micron diamond now completed the angles of the triangular and marginal ridge (Figure 39). Brownies and Greenies have convex sides requiring reshaping to a flat side so as not to create a concave surface when they are being used to final sculpt and finish (Figure 40). The straight-sided Brownie is used at 50,000 to 100,000 rpm with a copious water spray to final-shape what the diamond-coated acorn and X-mas tree bur have created (Figure 41). Brownies cut and polish composite but will only polish enamel, and are thus a true asset at a reasonable cost. Figure 42 shows the X-mas tree-shaped Greenie used at 100,000 rpm and with a copious water spray. TopDotz polisher on the latch bristle brush run at 20,000 rpm and without water will create a very high luster (Figure 43). Last, the cotton buff run dry at 20,000 rpm will afford a very high gloss (Fig- ure 44). The finished restoration is anatomic and high gloss (Figure 45 and Figure 46), and is ready for endodontic access with distal caries removed for an impervious seal. The post-treatment radiograph shows the root lesion restored and ready for endodontic treatment in this patient (Figure 47). Subsequent to endodontic therapy, margin elevation was planned to be accomplished using the dual-cure bulk-fill flowable and its requisite seal for the basement layer. Either a quartz fiber post or a Nayyar technique, again using the dual-cure flowable as the core, will provide truly minimal invasion.
Conclusion
Developments in filler technology, with enhanced polymers and fillers, have led to substantial improvements in the mechanical properties of resin composites, particularly with regard to their wear resistance. Heating of bulk-fill composite pastes has been utilized to facilitate the injection of these materials, but challenges with heating have made it desirable to have a cold flowable composite with posterior occlusal accommodating physical properties. New dual-cured bulk-fill resin-based composites have shown promise for uniform degree of conversion, depth of cure, and microhardness throughout the depth of direct restorations. Advances in polymer chemistry as well as in delivery systems allow all clinicians, regardless of hand size or strength, to deliver the new bulk-fill composites accurately and safely, without the need for heating, cumbersome compule guns, or "topping off" with universal composite. Dual-cured flowable composites have truly undergone great advancements in recent years.
About the Author
Patrick Roetzer, DDS, FACD, FICD Associate Professor AEGD Residency Program at Union City, California University of the Pacific, Arthur A. Dugoni School of Dentistry San Francisco, California
References
1. Lorincz H, Bardocz-Veres Z, Strnad G, Kerekes-Máthé B. In vitro study of mechanical properties of teeth restored with bulk-fill and universal composites using different detin adhesives. J Int Med.2022;7(2)-38-43.
2. Chan KHS, Mai Y, Kim H, Tong KCT, Ng D, Hsiao JCM. Review: resin composite filling. Materials (Basel). 2010;3(2):1228-1243.
3. Lim K, Yap AU, Agarwalla SV, Tan KB, Rosa V. Reliability, failure probability, and strength of resin-based materials for CAD/CAM restorations. J Appl Oral Sci. 2016;24(5):447-452.
4. Dukić W, Majić M, Prica N, Oreški I. Clinical evaluation of flowable composite materials in permanent molars small Class I restorations: 3-year double blind clinical study. Materials (Basel). 2021;14(15):4283.
5. Fugolin APP, Pfeifer CS. New resins for dental composites. J Dent Res. 2017;96(10):1085-1091.
6. Fraga MAM, Correr-Sobrinho L, Coelho Sinhoreti MA, Carletti TM, Correr AB. Do dual-cured bulk-fill resin composites reduce gaps and improve depth of cure. Braz Dent J. 2021;32(5):77-86.
7. Fugolin APP, Pfeifer CS. New resins for dental composites. J Dent Res. 2017;96(10):1085-1091.
8. Aggarwal N, Jain A, Gupta H, Abrol A, Singh C, Rapgay T. The comparative evaluation of depth of cure of bulk-fill composites - An in vitro study. J Conserv Dent. 2019;22(4):371-375.
9. Baroudi K, Rodrigues JC. Flowable resin composites: a systematic review and clinical considerations. J Clin Diagn Res. 2015;9(6):ZE18-ZE24.
10. Abbasi M, Moradi Z, Mirzaei M, Kharazifard MJ, Rezaei S. Polymerization shrinkage of five bulk-fill composite resins in comparison with a conventional composite resin. J Dent (Tehran). 2018;15(6):365-374.
11. Ribeiro BC, Boaventura JM, Brito-Gonçalves JD, Rastelli AN, Bagnato VS, Saad JR. Degree of conversion of nanofilled and microhybrid composite resins photo-activated by different generations of LEDs. J Appl Oral Sci. 2012;20(2):212-217.
12. Wang R, Liu H, Wang Y. Different depth-related polymerization kinetics of dual-cured, bulk-fill composites. Dent Mater. 2019;35(8):1095-1103.
13. Miller M. Bulk fill composites, average voids. Presented at the 2017 IADR/AADR/CADR General Session; April 2017; San Francisco, CA.
14. Windle CB, Hill AE, Tantbirojn D, Versluis A. Dual-cured dental composites: can light curing interfere with conversion? J Mech Behav Biomed Mater. 2022;132:105289.
15. Wang R, Wang Y. Depth-dependence of degree of conversion and microhardness for dual-cured and light-cured composites. Oper Dent. 2020;45(4):396-406.
16. Yang D-L, Sun Q, Niu H, Wang R-L, Wang D, Wang J-X. The properties of dental resin composites reinforced with silica col- loidal nanoparticle clusters: effects of heat treatment and filler composition. Composites Part B: Engineering. 2020;186(10):107791.
17. Angeletakis C, Aralis N. A new nanocomposite restorative containing alumina-silica nanoparticles. Abstract presented at the 2012 IADR/LAR General Session; June 22, 2012; Iguaçu Falls, Brazil.
18. Chung D, Aralis N, Li Y, Gu W. Property assessments of newly developed dual-cured bulk fill versus previous generation. Abstract presented at the 2022 AADOCR/CADR Annual Meeting; March 24, 2022; Atlanta, Georgia.
19. Gu W, Li Y, Chung D, Aralis N. Shade match study of dual-shaded universal nanocomposites. Abstract presented at the IADR/AADR/CADR General Session; 2020; Washington, DC.