You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Approximately 1.1 million infants die due to prematurity and 15 million more are born preterm, according to reports from the Joint European Federation of Periodontology and the American Academy of Periodontology.1 Preterm birth has been identified worldwide as the second most common cause of death in children under the age of five.1 Multiple risk factors, including behavioral, psychosocial, environmental, medical, nutritional, and biological, have been associated with adverse pregnancy outcomes.1,2 Evidence suggests that periodontitis is a risk factor for adverse pregnancy outcomes, including low birthweight babies (<2500 g), preterm birth (<37 weeks), pre-eclampsia, and miscarriage.2-3,5-10 Research investigating periodontitis as a risk factor has shown that a number of adverse pregnancy outcomes increase significantly in the presence of periodontal disease.1,2,8
Complex physiological changes occur during pregnancy, resulting in a heightened risk of gingivitis in the oral cavity.2,3 Gingivitis during pregnancy is common, affecting from 30 to 86% of all pregnant women.3,4 Left untreated, gingivitis can progress to periodontitis, resulting in attachment loss and permanent damage to the supporting structures of teeth.3,4 The American College of Obstetricians and Gynecologists (ACOG) reports that approximately 40% of pregnant women have some form of periodontal disease,5 which is not only detrimental to the oral cavity, but could potentially impact the health of the developing fetus.1 Despite the evidence supporting the importance of oral health, the ACOG reports that over half (59%) of all women do not receive oral health counseling during their pregnancy.5 In an additional study, the vast majority (96%) of pregnant women surveyed reported being unaware of the impact of oral health on pregnancy outcomes.11
Preventive, diagnostic, and restorative dental treatment has been shown to be safe during any trimester of pregnancy and essential to maintaining optimal oral health.5 The American Dental Association (ADA) supports the importance of oral health care during pregnancy and recommends a semiannual dental examination and prophylaxis.5 Oral health prevention requires a larger taskforce than dental professionals alone; therefore, physicians, midwives, nurse practitioners, and all prenatal health professionals play an equally important role in promoting oral health.12 Professional organizations have launched web portals, toolkits, and guidelines targeting the promotion of women's oral health during pregnancy.12 Oral health is such an important component of overall health that the ACOG developed suggested guidelines to include assessment of oral health at the first prenatal visit with subsequent prenatal visits providing opportunity for oral health promotion.5 While numerous research studies have been published in the literature suggesting periodontal disease may be a risk factor for adverse pregnancy outcomes,1-10 medical providers, who are ideally positioned to disseminate this information, may have gaps in their education. The purpose of this study was to assess prenatal health care professionals' levels of knowledge regarding oral health and its effect on pregnancy outcomes, examine their current practices in evaluating oral health, and determine their attitudes towards a multidisciplinary approach to providing comprehensive prenatal care.
Methods
A convenience sample of prenatal health professionals (n=208) from a healthcare organization in the Midwestern United States were invited to participate in a voluntary, web-based survey administered by Qualtrics™ (Provo, UT). Participants were given six weeks to complete the survey; non-responders were sent an email reminder four weeks after the initial request. Survey questions utilized for this study were modified from existing survey instruments used by Schramm et al,13 Bamanikar et al,14 and Sharif et al15 targeting dental hygienists, nurses, physicians and pregnant women. Target subjects in this study were the health care providers (midwives, nurse practitioners, physicians and residents) in a prenatal specialty practice within a healthcare organization. The survey included participants' demographic information, including gender, ethnicity and years of experience. Six questions addressed participants' knowledge, three questions addressed attitude, and six questions addressed participants' current clinical practice using a Likert Scale of 5 = strongly agree, 4 = somewhat agree, 3 = neither agree nor disagree, 2 = somewhat disagree, and 1 = strongly disagree. Experts in the field reviewed the survey questions for face validity; Institutional Review Board approval was granted for the study.
Responses were summarized with frequencies and percentages. A "knowledge score" was computed as the sum of the following items: I consider oral health care to be an important part of prenatal care; Pregnancy increases the tendency for the gingiva to bleed, swell, or be red; Pregnant mothers should be advised to stop brushing/flossing their teeth if their gingival tissues bleed; and Periodontal disease can be treated safely during pregnancy. The third item was reversed prior to calculating the score as a "disagree" response reflected more knowledge. Knowledge scores ranged from 4 (low knowledge) to 20 (high knowledge) and were compared between midwives and nurse practitioners versus physicians and residents using Wilcoxon Rank-Sum tests. Associations between this score and ordinal survey items were quantified with Spearman Correlations. All analyses were performed using SAS version 9.4™ (SAS Institute Inc; Cary, NC).
Results
A total of 208 questionnaires (n=208) were emailed to prenatal health care professionals including nurse practitioners, midwives, physicians and residents; 76 participants (n=76) consented to complete the survey, resulting in a 37% response rate. Of those participants, 3 were ineligible as they were not currently providing prenatal care. An additional 4 participants were excluded as they only answered the first survey question; a total of 69 survey responses were analyzed.
The majority of the participants were physicians (58%), identified as being female (78%) and white (93%). Participants reported a range of years of prenatal care experience, with one third of the respondents having fewer than 5 years of experience (33%), followed by one quarter (26%) with 16 or more years of experience. Demographic characteristics are shown in Table I.
Clinical practice characteristics of prenatal health professionals towards identifying oral health needs are displayed in Table II. Only 6% of the respondents "always" included an interview of the oral health history and 7% "always" included a dental screening to check the mouth for swollen or bleeding gingival tissue, mucosal lesions or signs of infection. Approximately 60% "never" or "rarely" performed an interview regarding the patient's oral health history and approximately 60% "never" or "rarely" included a dental screening during prenatal care. The most common reasons cited by the respondents who indicated not "always" including dental screenings were related to lack of time (64%), feeling this is the responsibility of dental professionals (48%), lack of patient request (47%), and lack of a current dental referral system (42%).
Respondents reported that they advise or refer a patient to see a dentist during pregnancy at least most of the time (39%) or sometimes (35%). However, the majority (84%) never advise a patient to delay their dental visits until after pregnancy. Over half of the respondents (61%) stated that oral health topics are rarely or never integrated into prenatal classes. Eight respondents skipped this question, perhaps due to lack of knowledge regarding all the topics covered in prenatal classes.
Over 80% of the respondents considered oral health to be an important part of prenatal care. A majority (84%) agreed that pregnancy increases the tendency of gingival inflammation and strongly disagreed (67%) regarding advising pregnant mothers to stop brushing or flossing if their gingival tissues bleed. Most agreed (90%) that gingival problems can be treated safely during pregnancy. Responses were more variable when questioned regarding the correlation between periodontal disease and adverse pregnancy outcomes. However, more than half agreed (61%) that gingival problems could result in low birthweight babies and that gingival problems may result in preterm birth (71%). The oral health knowledge of prenatal health professionals is shown in Table III.
Attitudes towards oral health by the respondents were positive with over half (60%) agreeing that they should be trained to perform oral health screenings and over 80% agreeing that they should update their knowledge regarding oral health during pregnancy. Only about 25% felt that it was not their responsibility to look into the patient's mouth to detect oral health problems (Table IV).
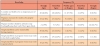
Respondent's average knowledge score was 17.4 (SD 1.8, range 11-20). Midwives and nurse practitioners had higher knowledge scores as compared to physicians and residents (average 18.6 vs 17.1, p=0.002). The oral health knowledge of the prenatal health professional groups and comparisons between midwives and nurse practitioners versus physicians and residents is shown in Table V. A moderate correlation was found between the knowledge score and frequency of including oral health history interviews during prenatal care visits (correlation = 0.36, p=0.002). A small correlation was found between the knowledge score and frequency of including a dental screening during prenatal care visits.
Results presented are largely descriptive, with the frequency and percentage in each response category reported. Between 7% and 16% of the responses were in the "neither agree nor disagree" category. In general, physicians and residents were more likely to select "neither agree nor disagree" option as compared to midwives and nurse practitioners. It is not possible to determine how the respondents interpreted this option, whether it indicates a lack of knowledge or a neutral attitude.
Discussion
Key inconsistencies in prenatal health professionals oral health knowledge and current clinical practice were found in this study as compared to previous studies.15,16,17 Comparable to this study, a previous survey of obstetricians found that a majority (84%) reported that periodontal disease may have an adverse effect on pregnancy outcomes.17 However, less than half (46%) performed an oral health screening as part of prenatal care and fewer than one-fourth (22%) looked into a woman's mouth at their prenatal examination.17 Discussing the patient's oral health history and evaluating the oral health status of a pregnant woman should be a critical component of prenatal care, yet only 6% of the providers in this study "always" interviewed the patient about their oral health history and 7% "always" conducted a dental screening.17 Prenatal health professionals play a pivotal role in identifying potential oral health conditions which may ultimately pose a risk on the developing fetus or pregnancy outcome. Conducting a visual screening of the oral cavity should be a required component of the prenatal health professionals' clinical practice routine.
Reasons for not consistently evaluating oral health during prenatal care included "need more training to specifically know what to look for," "unclear and not well-defined referral process," "no knowledge of teeth," "not adequately trained," and "currently not part of the routine exam." In general, while prenatal health professionals consider oral health to be an important part of prenatal care; a minimal number of prenatal health professionals actually evaluate oral health as part of their prenatal evaluations.5,16,17 Support for a more comprehensive approach to oral care during prenatal visits comes from the National Maternal and Child Oral Health Resource Center recommending that prenatal health care professionals take an oral health history, check the mouth for problems such as swollen or bleeding gingival tissue or tooth decay, and encourage women to seek dental care during the initial prenatal evaluation.18,19
While prenatal health professionals have expressed an interest in updating their oral health knowledge in a number of studies, they may be reluctant to ask about oral symptoms or screen for disease if they do not have a structured framework.15,16,17,20 Dental hygienists are well prepared to collaborate with prenatal health professionals, provide continuing education sessions on oral health during pregnancy, and conduct hands-on training designed to develop the skills necessary to identify oral conditions of concern. Guidelines recommended in the white paper on oral health and primary care commissioned by the National Interprofessional Initiative describe five essential components of an oral health delivery framework in health care settings.20 Health care providers should ask about oral health risk factors and symptoms of oral disease, look for signs that indicate oral health risk or active oral disease, decide on the most appropriate response, act by offering preventive interventions and/or referral for treatment, and document as structured data for decision support and population management.20 Utilization of this framework can serve to routinely address oral health as well as create a multidisciplinary relationship between health professionals and dental professionals.
Future studies could explore a multidisciplinary approach to providing comprehensive care to women with dental professionals collaborating with primary care providers and gynecologists to implement oral health education along with professional dental and dental hygiene care as part of the preconception period. In a study by Hashim and Akbar, the majority of gynecologists surveyed were shown to be highly knowledgeable about the relationship between oral health and pregnancy outcomes, and advised their pregnant patients to visit a dentist during their pregnancy.21 While gynecologists in the Hashim and Akbar study appeared to be very knowledgeable about the importance of oral health during pregnancy, there were misconceptions regarding the safety of dental treatments during pregnancy particularly in regards to the use of vasoconstrictors in local anesthetics and limiting dental treatment to the second trimester.21 Dental hygienists can play a key role in education of gynecologists as well as all other medical colleagues regarding the importance and safety of oral health before, during, and after pregnancy. Increasing the awareness of oral health among all women, whether during preconception or pregnancy, may also influence better oral health for their children.
Education of pregnant women is also a critical component to prenatal care. Habashneh et al found less than half of the women surveyed reported a visit to the dentist during their most recent pregnancy.22 One of the factors contributing to this low rate was the lack of knowledge of the possible connection between oral health and pregnancy outcomes.22 Institutions should consider synchronizing oral health promotion with prenatal care visits, requiring women to view educational videos and provide informational brochures discussing the link between oral health and pregnancy outcomes and other topics related to pregnancy. Additional factors associated with the Habashneh et al findings were cost of care and lack of an established dentist.
Prenatal health care providers should develop contact information lists for non-profit dental clinics to serve those who may be faced with financial barriers. Increasing oral health awareness among pregnant women may ultimately reduce the risk of adverse pregnancy outcomes.
Limitations of this study included the use of a self-administered questionnaire versus direct observations of the prenatal health professionals in real time. There was no way to verify whether the prenatal health professional actually obtained an oral health history, provided a dental screening, or recommended dental treatment to their pregnant patients. An additional limitation of this study was the small sample size from one health care system, and the low response rate, limiting the generalization of the results.
Conclusion
The majority of prenatal health care professionals surveyed were knowledgeable about oral health and its importance as it relates to prenatal care; however, a deficit was identified in current practice in regard to oral health history interviewing and conducting dental screenings. There is a need to implement best practice guidelines for prenatal care to include routine dental screenings as well as to engage pregnant women in oral health prevention. Optimal oral health requires a multidisciplinary approach in which dental hygienists can play a significant role by educating women's healthcare providers and raising awareness of the connection between oral health and pregnancy outcomes.
About the Authors
Sarah B. Hoerler, RDH, MS is a registered dental hygienist in the Department of Dental Specialties, Division of Periodontics; Sarah Jenkins, MS is a statistician in the Department of Health Sciences Research, Division of Biomedical Statistics and Informatics; Daniel Assad, DDS, MA is a periodontist and the residency director in the Department of Dental Specialties, Division of Periodontics; all at the Mayo Clinic, Rochester, MN.
Corresponding author: Sarah B. Hoerler, RDH, MS; hoerler.sarah@mayo.edu
References
1. Sanz M, Kornman K. Periodontitis and adverse pregnancy outcomes: consensus report of the Joint EFP/AAP Workshop on periodontitis and systemic diseases. J Periodontol 2013 Apr;84(4 Suppl.):S164-S169.
2. Turton M, Africa C. Further evidence for periodontal disease as a risk indicator for adverse pregnancy outcomes. Int Dent J 2017 Jun;67(3):148-56.
3. Teshome A, Yitayeh A. Relationship between periodontal disease and preterm low birth weight: systematic review. Pan Afr Med J 2016 Jul;24:215-224.
4. Lohana MH, Suragimath G, Patange RP, et al. A prospective cohort study to assess and correlate the maternal periodontal status with their pregnancy outcome. J Obstet Gynaecol India 2017 Feb;67(1):27-32.
5. American College of Obstetricians and Gynecologists. Committee Opinion No. 569: oral health care during pregnancy and through the lifespan. Obstet Gynecol. 2013 Aug;122 (2Pt1):417-22.
6. Vanterpool SF, Tomsin K, Reyes L, et al. Risk of adverse pregnancy outcomes in women with periodontal disease and the effectiveness of interventions in decreasing this risk: protocol for systematic overview of systematic reviews. Syst Rev 2016 Feb;5:16-21.
7. Schwendicke F, Karimbux N, Allareddy V, et al. Periodontal treatment for preventing adverse pregnancy outcomes: a meta and trial sequential analysis. PLoS One 2015 Jun;10(6):1-12.
8. Ide M, Papapanou PN. Epidemiology of association between maternal periodontal disease and adverse pregnancy outcomes - systematic review. J Clin Periodontal 2013 Apr;40(Suppl14):S181-S194.
9. Uppal A, Uppal S, Pinto A, et al. The effectiveness of periodontal disease treatment during pregnancy in reducing the risk of experiencing preterm birth and low birth weight: a meta-analysis. J Am Dent Assoc 2010 Dec;141(12):1423-34.
10. Lopez N, Uribe S, Martinez B. Effect of periodontal treatment on preterm birth rate: a systematic review of meta-analyses. Periodontal 2000 2015 Feb;67(1):87-130.
11. Gupta S, Jain A, Mohan S, et al. Comparative evaluation of oral health knowledge, practices, and attitude of pregnant and non-pregnant women, and their awareness regarding adverse pregnancy outcomes. J Clin Diagn Res 2015 Nov;9(11):26-32.
12. Hartnett E, Haber J, Krainovich-Miller B, et al. Oral health in pregnancy. J Obstet Gynecol Neonatal Nurs 2016 April;45: 565-73.
13. Schramm S, Jacks M, Prihoda T, et al. Oral care for pregnant patients: A survey of dental hygienists' knowledge, attitudes, and practice. J Dent Hyg 2016 Apr;90(2):121-7.
14. Bamanikar S, Kee LK. Knowledge, attitude, and practice of oral and dental healthcare in pregnant women. Oman Med J 2013 Jul;28(4):288-91.
15. Sharif S, Saddki N, Yusoff A. Knowledge and attitude of medical nurses toward oral health and oral health care of pregnant women. Malays J Med Sci. 2016 Jan;23(1):63-71.
16. Al-Habashneh R, Aljundi SH, Alwaeli HA. Survey of medical doctors' attitudes and knowledge of the association between oral health and pregnancy outcomes. Int J Dent Hygiene 2008 Aug;6(3):214-20.
17. George A, Shamim S, Johnson M, et al. How do dental and prenatal care practitioners perceive dental care during pregnancy? Current evidence and implications. Birth 2012 Sep;39(3):238-47.
18. Oral Health Care During Pregnancy Expert Workgroup. Oral health care during pregnancy: a national consensus statement. [Internet] Washington, DC: National Maternal and Child Oral Health Resource Center; 2012 [cited 2018 Oct 1]. Available from https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf.
19. Kumar J, Iida H. 2008. Oral Health Care During Pregnancy - A Summary of Practice Guidelines. Washington, DC. National Maternal and Child Oral Health Resource Center.
20. Hummel J, Phillips KE, Holt B, et al. Oral Health: An Essential Component of Primary Care [Internet]. Seattle, WA: Qualis Health; 2015 [cited 2018 Oct 1] available from: http://www.niioh.org/sites/default/files/Oral_Health_white_paper_final.pdf
21. Hashim R, Akbar M. Gynecologists' knowledge and attitudes regarding oral health and periodontal disease leading to adverse pregnancy outcomes. J Int Soc Prev Community Dent 2014 Dec; 4(Suppl 3):S166-S172.
22. Habashneh R, Guthmiller M, Levy S, et al. Factors related to utilization of dental services during pregnancy. J Clin Periodontol 2005 Jul;32(7):815-21.