You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Patients with edentulous arches traditionally replace their missing teeth with full-arch dentures. Although removable prostheses help to resolve several issues associated with edentulism (eg, lack of self-esteem, dissatisfaction with facial appearance), the instability of traditional dentures often introduces other challenges for the wearer, including speaking and chewing difficulties, pain and discomfort, and unnatural lip, tongue, and cheek muscle movements in order to keep the denture(s) in place.1,2
Fortunately, many patients with fully edentulous arches are candidates for implant-supported or -retained denture prostheses, which eliminate many of the issues experienced with traditional dentures.3 When full-arch prostheses are supported and/or retained by dental implants, they are more secure and stable, have greater support, and are more comfortable for patients.4
Technological advancements have contributed to more predictable diagnosis and treatment planning of implant-supported or -retained full-arch prostheses to restore edentulous arches. These have included 3D implant treatment planning software, precision surgical guides, and the imaging technologies that capture the necessary intraoral and anatomical data that help to direct implant and abutment placement (eg, cone beam computed tomography [CBCT]).5 While CBCT scans are very sophisticated and provide tremendous amounts of information, they do present limitations that may prevent a definitive prosthesis from being loaded at the surgical appointment.
For example, CBCT scans have been shown to underestimate jaw sizes (on average by about 0.5 mm) and bone height, and they may not visualize areas of thin bone.6 Additionally, when CBCTs are used to plan implant positions, a deviation between the surgical plan and the actual plan of the hex could range from 0.3 mm to 2.3 mm, and in the apex, between 0.3 mm to 2.4 mm.7 This may help to explain the frequency with which clinicians have tried to place a full-arch, screw-retained prosthesis according to a CBCT-based treatment plan, only to experience deviations in the implant/abutment position that resulted in a prosthesis that would not passively fit.
A number of approaches have therefore been taken to overcome and/or compensate for the deviation in positioning. Among them is planning the full-arch restoration and having the laboratory technician finish only one implant site, leaving the additional sites to be finished chairside immediately following implant placement. In recent years, a hybrid solution has been adopted that encompasses a cement-retainable prosthetic component that is placed on an abutment and combined with a screw-retained metal cylinder. In situations where angle correction is indicated, an angled abutment may be used in conjunction with the metal cylinder.
However, there are several caveats associated with implementing this abutment solution. First, consideration must be given to the potential for retained cement, which has been shown to be associated with peri-implant diseases and subsequent implant failure.8,9 Second, although this hybrid option enables realization of the ideal angulation for connecting the full-arch prosthesis to the supporting implant, the location of the screw-access hole also requires consideration and planning.10 In particular, the screw-retained component requires care when determining the exit point of the screw-access hole so that it is not on the facial aspect; angulation issues should be resolved by positioning the implant fixture so the screw-access hole can be redirected to either the occlusal or lingual aspect of the prosthesis.
Implant abutment jigs fabricated and provided by the laboratory are helpful when placing and correcting this type of angled abutment. Once all the abutments are placed, the screw-retained cylinders can be added and acrylic placed into the overdenture at the same time. After pick-up and finishing, the prosthesis is screwed into place, and the access holes filled with Teflon tape and light-cured restorative material. Few complications have been associated with this technique, but for some patients, whether due to their occlusion or diet, maintenance issues have been observed involving the restorative material used to seal the screw-access hole; the composite has either worn or dislodged, requiring replacement.11
A No-Screw, No-Cement Alternative
Although such techniques are not complicated or technically difficult, they can be extremely time consuming for the dentist, laboratory technician, and patient. An alternative to cement- or screw-retained implant attachments is a fixed locator attachment system for rigid connection of full-arch restorations onto endosseous dental implants (eg, LOCATOR F-Tx, Zest, www.zestlocator.com). Capable of being removed and reattached by the dentist as needed, such a system supports full-arch prostheses in the mandible or maxilla without prosthetic screws, screw-access channels, or cement.
Considering the discrepancies and deviations in the implant/abutment position that result in a prosthesis not fitting passively,6,7 the fact that the fixed locator attachment system includes a spherical abutment geometry allowing the denture attachment housing to pivot in any direction is significant. In fact, this pivoting ability enables alignment of the attachment housings to create a more parallel draw for the prosthesis, thereby contributing to a stress-free and passive fit. This also enables angulation correction up to 20° from the vertical, and 40° between implants, without the need for angled abutments.
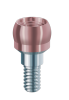
The spherical abutment itself is coated with titanium carbo-nitride (TiCN) and, as a result, demonstrates a hard, smooth, and wear-resistant exterior. Compared to abutments with titanium nitride (TiN) coatings, it is 32% harder, demonstrating 26% greater wear resistance and a 64% reduction in roughness. These characteristics may explain why a locator system showed superior clinical results in a study examining complications with attachments for implant-supported overdentures (eg, retention loss, attachment dislodgement).12
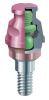
Aggressive grooves and flats on the denture attachment housing—which is passively picked up in the prosthesis during a chairside procedure—limit vertical and rotation movement, contributing to stability and essentially locking the prosthesis into place. Its degree of retention after placement is such that the prosthesis can only be removed by the dentist. Research has demonstrated that locator attachments could improve the stability of dentures dramatically, and that they have a stronger effect on preventing horizontal denture movement.13
This attachment housing is internally threaded to accept the polyether ether ketone (PEEK) retention balls and processing ball, which snap into the abutment. Combined, these components eliminate the need for abutment cylinder preparation, screw-access channels and filling composite, and intensive chairside procedures to ensure retention of the denture prosthesis. Compared to ball attachments, locator attachments have shown better retentive properties,14 and in terms of prosthodontic maintenance, cost, and ease of denture preparation, a locator system produced superior clinical results.15
During recall appointments and/or yearly maintenance appointments, the prosthesis can be quickly and easily removed using simple hydraulic displacement; only the retentive balls require replacement. This contrasts to the complexity associated with screw-retained full-arch prostheses, which require drilling out composite material, unscrewing all components, cleaning the access channels and components, and then refilling them.
Indicated for full-arch prostheses, the removable fixed attachment system is not appropriate for single tooth restorations, unilateral bridges, or cases that require a resilient connection. It is also not appropriate for use on implants with a divergence greater than 20° from the vertical.
The system can be used to stabilize newly fabricated full-arch restorations (eg, all-ceramic, prosthetic acrylic) or a patient’s existing full denture if the position of the teeth is acceptable. A metal frame around acrylic, PBNA, or porcelain can be used, or original dentures can be realigned.
Treatment Planning
The basic prosthodontic principles that are followed for most cases are applicable for the removable fixed attachment system (Figure 1). In the following case, the author used a guided surgical technique, as is his preference. An analysis of the patient’s anatomy is performed using CBCT scans. Using implant treatment planning software, the CBCT data is converted to enable visualization, planning, and precise preoperative selection of the correct implant position as it relates to available bone. Adjustments can also be made to the site prior to ordering the surgical guide.
The implant planning software is then used to design the full-arch implant-retained prosthesis in the context of where the implants will be placed, ensuring there will be adequate space for the planned attachments. This enables correction of any angle issues preoperatively so that the implants can be placed ideally through the surgical guide. Upon receipt, the surgical guide can be forwarded to the laboratory for use in fabricating a bite to help stabilize the surgical guide during implant placement, as well as in designing the full-arch prosthesis and fabricating an immediate load prosthesis.
Following implant placement (Figure 2), the spherical abutments are screwed into place (Figure 3 and Figure 4), which enables the denture attachment housings to pivot in any direction for better alignment of the full-arch prosthesis. The denture attachment housing—including the processing balls—are then placed and pivoted into the correct position and angulation (Figure 5 through Figure 7), creating an easily drawn path of insertion and removal for the prosthesis.
When an immediate denture is made, the inside is hollowed out to create recess holes wide enough to accept the denture attachment housings. The prosthesis is tried in to ensure midline alignment (Figure 8), after which it is removed. Chairside acrylic material (eg, dual/light-cured syringeable material) is placed to enable pick-up of the denture attachment housing, after which it is returned to the mouth and the patient instructed to close into proper occlusion. The material is light-cured, removed, and allowed to sit, and then finished with laboratory burs to cut-back excess acrylic and polished.
Conclusion
As the technologies and techniques for providing implant-supported and -retained prostheses have advanced, dentists now are able to provide edentulous patients with sophisticated options that are simultaneously simpler to place, more precise, and easier to maintain. Using a removable attachment system for fixed full-arch prostheses eliminates the need for cement, screw-access channels, screws, and composite filling materials. It also helps to resolve the issues that can result from deviations in implant/abutment location after placement.
REFERENCES
1. Bilhan H, Geckili O, Ergin S, et al. Evaluation of satisfaction and complications in patients with existing complete dentures. J Oral Sci. 2013;55(1):29-37.
2. Hogenius S, Berggren U, Blomberg S, et al. Demographical, odontological, and psychological variables in individuals referred for osseointegrated dental implants. Community Dent Oral Epidemiol. 1992;20(4):224-228.
3. Tanner T. Treatment planning for dental implants: considerations, indications, and contraindications. Dent Update. 1997;24(6):253-260.
4. Melilli D, Rallo A, Cassaro A. Implant overdentures: recommendations and analysis of the clinical benefits. Minerva Stomatol. 2011;60(5):251-269.
5. Nickenig HJ, Eitner S. Reliability of implant placement after virtual planning of implant positions using cone beam CT data and surgical (guide) templates. J Craniomaxillofac Surg. 2007;35(4-5):207-211.
6. Ferrare N, Leite AF, Caracas HC, et al. Cone-beam computed tomography and microtomography for alveolar bone measurements. Surg Radiol Anat. 2013;35(6):495-502.
7. Van Assche N, van Steenberghe D, Guerrero ME, et al. Accuracy of implant placement based on pre-surgical planning of three-dimensional cone-beam images: a pilot study. J Clin Periodontol. 2007;34(9):816-821.
8. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80(9):1388-1392.
9. Linkevicius T, Puisys A, Vindasiute E, et al. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin Oral Implants Res. 2013;24(11):1179-1184.
10. Wadhwani C, Piñeyro A, Avots J. An esthetic solution to the screw-retained implant restoration: introduction to the implant crown adhesive plug: clinical report. J Esthet Restor Dent. 2011;23(3):138-143.
11. Pjetursson BE, Thoma D, Jung R, et al. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res. 2012;23 Suppl 6:22-38.
12. Cakarer S, Can T, Yaltirik M, Keskin C. Complications associated with the ball, bar and Locator attachments for implant-supported overdentures. Med Oral Patol Oral Cir Bucal. 2011;16(7):e953-e959.
13. Yang X, Rong QG, Yang YD. Influence of attachment type on stress distribution of implant-supported removable partial dentures. Beijing Da Xue Xue Bao. 2015;47(1):72-77.
14. Türk PE, Geckili O, Türk Y, et al. In vitro comparison of the retentive properties of ball and locator attachments for implant overdentures. Int J Oral Maxillofac Implants. 2014;29(5):1106-1113.
15. Zou D, Wu Y, Huang W, et al. A 3-year prospective clinical study of telescopic crown, bar, and locator attachments for removable four implant-supported maxillary overdentures. Int J Prosthodont. 2013;26(6):566-573.