You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
More than 25 million endodontic procedures are performed every year in the United States.1 Even with the availability of successful implant restorative alternatives, many patients prefer a minimally invasive approach that allows them to keep their own teeth-one that does not require a treatment time that can be lengthy and a challenging period of provisionalization. In addition, treatment to retain a tooth usually costs less than implant therapy, which can be advantageous to patients during these challenging times. Ultimately, the diagnostic and restorative skills of the dentist are paramount to achieving long-term success, whichever mode of treatment is selected.
Advancements in the endodontic armamentarium have facilitated the trend toward more conservative, less invasive root canal protocols. Conservation of tooth structure has been shown to increase fracture resistance.2 As a result. access openings and flaring have been downsized, leaving narrow canal spaces. Most root canal treatments require an indirect restoration, and many also require an endodontic post to provide adequate retention of the core.
Indirect Cast Metal Posts
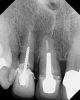
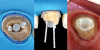
The use of custom cast metal posts (Figure 1), which were once considered the "gold standard," has greatly diminished in North America due to the additional time, expense, and loss of tooth structure associated with their fabrication and placement. In the past, many cast metal posts were cemented rather than bonded and thus have a higher likelihood of coming loose with the crown attached to the post and core (Figure 2).
Direct Prefabricated Metal Posts
Today, most post and core restorative treatments employ a prefabricated post made from either metal or fiber. Although the trend has been toward the use of fiber posts, early in the transition from indirect to direct post and core protocols, metal posts were primarily used. Prefabricated metal posts are available in two basic shapes: parallel and tapered. In addition to being highly radiopaque, metal posts are extremely rigid, possessing a high modulus of elasticity of 100 GPa to 200 GPa, and transfer more stress from the coronal aspect to the thinner apical segment.3 Because of the "wedge effect," tapered metal posts can be more threatening to the remaining tooth structure. This was especially true with the early threaded posts, which readily came loose (Figure 3) or resulted in a fractured root.
When compared with tapered posts, parallel metal posts fit well in the apical section of an endodontically treated tooth, but not in the coronal aspects of the canal. The only way to improve their fit is to remove additional deep internal dentin with a parallel drill.4 However, this removal of valuable tooth structure weakens the tooth. The ledge that is created at the end of the preparation predisposes the tooth to stress points, cracks, and fracture at that juncture (Figure 4). Metal posts are less effective than fiber posts at stabilizing the post and core structure in the absence of ferrule, which is evidenced by the development of more interfacial defects with either composite or dentin.5
Direct Prefabricated Fiber Posts
Fiber-reinforced composite posts are being increasingly used and offer an elastic modulus similar to dentin, noncatastrophic failure modes,6 better esthetics, reversibility,7 and improved biocompatibility due to their noncorrosive nature. In addition, the trend toward all-ceramic crowns necessitates the use of tooth-colored posts and cores so they do not show through and result in gray discoloration. Prefabricated fiber posts are usually bonded rather than luted with conventional cement, and they are available in a wide variety of shapes, sizes, and designs. Although ideal endodontic shaping creates gently tapered, narrow, and symmetrically round canals, a significant percentage of canals do not exhibit these characteristics.8 As a result, fiber posts have been developed to effectively treat oval-shaped, over-flared, and "c-shaped" configurations.
Fiber posts are offered in both parallel and tapered shapes. Just like parallel metal posts, parallel fiber posts require apical tooth removal, which creates a ledge in the canal that can lead to failures. Tapered fiber posts offer a significant advantage because they better reflect the overall shape and anatomy of the prepared root canal, and they do not transfer as much destructive force to the apex of the tooth due to their ability to better flex and absorb punishing energy. Long-term clinical studies have shown excellent overall clinical success rates with fiber-reinforced composite posts.9-11
Anatomical Double-Tapered Fiber Posts
A post that is tapered over its entire length is preferred over one that is only tapered at the apical tip because it will leave less space to fill in at the coronal aspect. However, double-tapered posts have been designed to more accurately mimic the shape of the typical root canal. These double-tapered posts, which have two separate tapers in the apical and middle sections, offer an anatomical improvement12 and are available in several sizes with specific instruments to better adapt the root canal to accommodate them while reducing the amount of dentin that is removed.
Oval-Shaped Fiber Posts
For oval-shaped canals, posts with an oval-shaped coronal two-thirds and a tapered, round apical one-third have been introduced. The oval-shaped section reduces the amount of coronal space that needs to be filled in and increases the flexural strength of the post in that region (Figure 5). These posts are useful adjuncts, providing better adaptation13 and increased fracture resistance.14 Similar to other available systems, oval-shaped post systems require separate, specific instruments to accommodate and fit the various sizes.
Accessory Fiber Posts
Also referred to in the literature as auxiliary posts, accessory posts are thin fiber tendrils or, in essence, "mini" fiber posts (eg, Fibercone®, RTD Dental; Reforpin®, Angelus; UniCore®, Ultradent). They are designed to be used alongside a master post to displace the cement with a precured, factory-made composite material. Similar to auxiliary gutta percha cones, they can be inserted into the cement as needed (Figure 6). Studies show that accessory fiber posts minimize cement thickness,15 reduce stress on internal surfaces,16 and increase the tooth's resistance to fracture.17 This is a versatile and effective technique, but it requires the ability to conscientiously and rapidly place posts and adds to the cost of the restoration.
Adjustable Post-Sleeve
An adjustable post and sleeve system has been recently introduced comprised of a single-size post and a tapered sleeve of the same material. The sleeve can be utilized, when necessary, to customize the post in cases involving flared or overprepared canals. After the post is inserted, the sleeve slides down onto it and into the flared canal to whatever depth is required for the best fit (Figure 7). The sleeve significantly reduces the volume of cement required to fill the coronal area of the pulp chamber and is much stronger than many resins that have been previously used for this purpose.
Relined Fiber Posts
Fiber posts have been developed that can be used a direct/indirect technique. In this technique, after the post is tried into the canal, it is removed, and a light-cure composite is placed around it to fill in the voids inside the tooth. Once reseated in the canal, the composite is preliminarily light cured, removed, and then further cured extraorally to ensure optimal polymerization. The result is a strong core mass, which has been shown to help save remaining tooth structure.15 As with the traditional custom cast post technique, relined fiber posts require that all undercuts be eliminated in order to ensure a clear path of insertion. This method has been shown to improve fracture resistance of the restored root.18
Fiber-Augmented Posts
Techniques involving the use of "bundled" fibers (eg, Interlig®, Angelus; Quartz Splint®, RTD Dental; Ribbond®, Ribbond) to fabricate a customized post or to improve the fit of a prefabricated fiber post have been in the literature since the mid-1990s (Figure 8). Placing fibers oriented with the long axis of the fibers in the post has been shown to improve failure modes and fracture resistance.19 This direct/indirect process is effective; however, it can be technique-sensitive, and the fibers are not radiopaque.
CAD/CAM Fiber-Reinforced Composite Post/Cores
Several companies (eg, Angelus, Bioloren, Itena, RTD Dental, Shofu) offer fiber-reinforced composite in blocks and/or discs that facilitate the milling of a "custom fit" one-piece post/core. Some of these are made from unidirectional fibers, and others are made from multidirectional ones. Ceramic blocks are also available for this technique. Generally, the flared canal is prepared to eliminate any potential undercuts in the same manner as for a cast post or a relined post. The preparation, or a model analog of it, is scanned to create an STL file that is sent to the milling machine for fabrication (Figure 9). Although this technique has only recently been introduced, early in-vitro results are promising, especially regarding low cement film thickness and higher flexural properties.20-21
Conclusion
Conservation of natural tooth structure has become the standard of care in all aspects of dentistry, including the preparation of root canals and their access openings. As root canal preparations have become narrower, so too have the sizes of fiber posts. This can create challenges when restoring flared or unusually shaped canals. It is important to fill the coronal areas that are in contact with the post with a strong structural material. Excess cement (resin or otherwise) may not have enough filler or cross-linking to provide adequate strength in a mass of this size. Resin cements perform well in low film thicknesses of less than 100 µm, but a post swimming in a sea of cement should be avoided. Displacing cement with a biocompatible and mechanically compatible material with superior properties is the goal to improve the overall fracture resistance and survival rate of the restoration.
Queries regarding this course may be submitted to authorqueries@aegiscomm.com
Acknowledgement
The author would like to thank Abelardo Báez Rosales, DDS; Alejandro Bertoldi Hepburn, DDS; Richard Bohay, DMD, MSc; Leendert Boksman, DDS; and Daniel Torassa, DDS, for contributing photography to this article.
About the Author
Daniel H. Ward, DDS
Diplomate
American Board of Aesthetic Dentistry
Fellow
Academy of General Dentistry
Private Practice
Columbus, Ohio
References
1. Data provided by American Academy of Endodontics communications specialist. 2020.
2. Zogheib LV, Pereira JR, do Valle AL, de Oliveira JA, Pegoraro LF. Fracture resistance of weakened roots restored with composite resin and glass fiber post. Braz Dent J. 2008;19(4):329-333.
3. Sirimai S, Riis DN, Morgano SM. An in vitro study of the fracture resistance and the incidence of vertical root fracture of pulpless teeth restored with six post-and-core systems. J Prosthet Dent. 1999;81(3):262-269.
4. Rosenstiel SF, Land MF, FujimotoJ. Contemporary Fixed Prosthodontics. 4th ed. Mosby; 2006: 343.
5. Dietschi D, Ardu S, Rossier-Gerber A, Krejci I. Adaptation of adhesive post and cores to dentin after in vitro occlusal loading: evaluation of post material influence. J Adhes Dent. 2006;8(6):409-419.
6. Barjau-Escribano A, Sancho-Bru JL, Forner-Navarro L, et al. Influence of prefabricated post material on restored teeth: fracture resistance and stress distribution. Oper Dent. 2006;31(1):47-54.
7. Cormier CJ, Burns DR, Moon P, In vitro comparison of the fracture resistance and failure mode of fiber, ceramic, and conventional post systems at various stages of restoration. J Prosthodont.2001;10(1):26-36.
8. Weine FS. Endodontic Therapy. 6th ed. Elsevier; 2004.
9. Cagidiaco MC, Goracci C, Garcia-Godoy F, Ferrari M. Clinical studies of fiber posts: a literature review. Int J Prosthodont. 2008;21(4):328-336.
10. Bitter K, Noetzel J, Stamm O, et al. Randomized clinical trial comparing the effects of post placement on failure rate of postendodontic restorations: preliminary results of a mean period of 32 months. J Endod. 2009;35(11):1477-1482.
11. Cerny D, Eckert S, Mounajjed R. Retrospective 9-year clinical outcome report on adhesive post-endodontic treatment of anterior teeth using prefabricated fiber posts. Int J Prosthodont. 2019:32(1):14-16.
12. Boudrias P, Sakkal S, Petrova Y, Anatomical post design applied to quartz fiber/epoxy technology: a conservative approach. Oral Health. 2001;91(11):9-16.
13. Coniglio I, Carvalho CA, Magni E, et al. Post space debridement in oval-shaped canals: the use of a new ultrasonic tip with oval section. J Endod. 2008;34(6):752-755.
14. Kılınç H, Aslan T, Kılıç K, et al. Fracture resistance of teeth with oval canal morphology restored using oval and circular posts. J Oral Sci. 2016;58(3):339-345.
15. Maceri F, Martignoni M, Vairo G. Mechanical behaviour of endodontic restorations with multiple prefabricated posts: a finite-element approach. J Biomech. 2007;40(11):2386-2398.
16. Li Q, Xu B, Wang Y, Cai Y. Effects of auxiliary fiber posts on endodontically treated teeth with flared canals. Oper Dent. 2011;36(4):380-389.
17. Martelli H Jr, Pellizzer EP, Rosa BT, et al. Fracture resistance of structurally compromised root filled bovine teeth restored with accessory glass fibre posts. Int Endod J. 2008;41(8):685-692.
18. Dal Piva AMO, Tribst JPM, Borges ALS, et al. Do mechanical advantages exist in relining fiber posts with composite prior to its cementation? J Adhes Dent. 2018;20(6):511-518.
19. Mortazavi V, Fathi M, Katiraei N, et al. Fracture resistance of structurally compromised and normal endodontically treated teeth restored with different post systems: An in vitro study. Dent Res J (Isfahan).2012;9(2):185-191.
20. Borzangy SS, Saker SM, Al-Zordk WA. Effect of restoration technique on resistance to fracture of endodontically treated anterior teeth with flared root canals. J Biomed Res. 2019;33(2):131-138.
21. Ruschel GH, Gomes ÉA, Silva-Sousa YT, et al. Mechanical properties and superficial characterization of a milled CAD-CAM glass fiber post. J Mech Behav Biomed Mater. 2018;82:187-192.