You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Implant dentistry has predictably provided a stable foundation to support implant prostheses, restoring function and esthetics to both failing and edentulous dentitions. This success has been predicated on the well-documented research by Bränemark1-4 and numerous reports over the past several decades substantiating osseo-
integration as the ideal predictable basis to support tooth replacement and thereby restore esthetics and establish function.5-8
Since its inception, implant dentistry has evolved with many enhancements, culminating in today's proven protocols of immediate implant surgery and immediate load.9-21 The prosthetic sequence has generally been consistent over the years. Transfer impressions have been used to capture implant location, and conventional prosthetic means have been used, resulting in the fabrication of cement- or screw-retained implant-supported prostheses that satisfy the dentition esthetically, functionally, and phonetically. This is typically preceded by a healing period of 4 to 6 months for
osseointegration, and then numerous prosthetic appointments are scheduled until delivery of the final prosthesis.
A Digital Process
A recently developed streamlined digital process, as demonstrated in the cases presented in this report, involves fabrication of an optimally esthetic and functional prosthesis that provides a precise and passive fit on multi-unit abutments screwed on the implants, establishing proper lip support and rejuvenating esthetic appearance. This protocol allows for same-day digital delivery of an in-house 3D-printed provisional prosthesis after implant placement surgery. In this manner the prosthetic sequence is significantly reduced, providing restoration of esthetics and function digitally in one day. The technology aims to optimize the accuracy of soft-tissue architecture and implant position capture while enabling the design and manufacture of the most ideal prosthesis for the selected dentition, taking into consideration patient photographs and digital scanning of the dentition and soft tissue.
An intraoral scanner is used presurgically and at the time of surgery to scan soft tissues and existing dentition with scan gauges. The scan gauges are placed on multi-unit abutments secured to the implants and scanned following a highly specific protocol to capture the exact position of the implants. From this information, using digital technology and a fully digital protocol, an STL file of the optimal provisional prosthesis is produced, taking into consideration the many algorithms in an artificial intelligence (AI) memory bank to generate a patient-specific prosthetic file. This file is then transmitted to the local drive via a proprietary web portal and sent to the in-office 3D printer for fabrication of a screw-retained provisional implant prosthesis.
To summarize, a series of predetermined intra-
oral scans are taken at the time of surgery that provide geometric information incorporating hard tissue, soft tissue, and highly precise seven-
sided scan gauges, which are screw-retained to the multi-unit abutments that are screwed onto the implants, capturing the exact position of the implants. These data serve as input for a digital impression. Computer algorithms then digitally calibrate the absolute abutment positions and ideal prosthetic design, taking into account vertical dimension, correct bite relationships, and dentition. Subsequently, a 3D STL file is produced intended for in-house production of a provisional prosthesis that fits precisely on the multi-unit abutments attached to the implants.
The sequence concludes with the delivery of a screw-retained provisional implant prosthesis on the day of surgery. After integration is confirmed, the digital workflow is also used to efficiently fabricate the final restoration. This protocol provides digital delivery of an esthetic provisional screw-retained implant prosthesis on the day of implant surgery without the need for any physical impressions or prosthetic conversions.
The following case reports delineate a fully digital restorative treatment protocol and document the particular steps in this treatment sequence.
Case Reports
Case 1
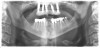
A 36-year-old male patient presented with a highly compromised maxillary dentition comprised of only teeth Nos. 4, 6, 7, 9, 10, 11, and 14 (Figure 1 and Figure 2). This poor condition was the result of only sporadic dental care with extractions and no teeth replacements. Soft tissues had normal contour, and bone profiles were generally sustained and favorable. The patient was excited about having the option to transform his compromised esthetics and function in one visit.
At the initial appointment, a panoramic x-ray and periapical x-rays were taken. As part of the protocol, photographs of the patient's head to shoulders were taken, and scans of the teeth and soft tissue were captured with an intraoral scanner. These images were then sent electronically to the implant designer and manufacturer. Five days later, a virtual smile design (VSD) was provided for review and approval.
At the following visit, the patient was anesthetized with xylocaine with 1:100,000 epinephrine. Teeth Nos. 4, 6, and 11 were extracted, and immediate implants with multi-unit abutments were placed prosthetically correctly with favorable insertion torques in sites Nos. 6 and 11 (Figure 3). Scan gauges were attached to the multi-unit abutments, and a scan was taken to capture the location of the implants with a reference to the remaining teeth with capture of the soft tissues.
Subsequently, teeth Nos. 7, 9, and 10 were carefully extracted with retention of tooth No. 14 to maintain vertical dimension of occlusion with opposing tooth No. 19. An immediate implant with a multi-unit abutment was placed in site No. 4, and additional implants with multi-unit abutments were placed in sites Nos. 8 and 13. All multi-unit abutments were torqued to 30 Ncm.
Scan gauges were then attached to the multi-unit abutments on the remaining implants so that all the implants were now in place with scan gauges (Figure 4). A scan was taken to capture all of the implants and surrounding soft tissue. The scanning protocol calls for scanning left to right, and then a separate scan right to left. These files were then sent electronically to the proprietary web portal.
The computer software then calibrates based on a unique durable medical equipment (DME) file assigned with the scan gauge kit used for the left to right and right to left scan gauge data. The scan gauge data captured are used with proprietary AI software to establish exact multi-unit positioning. The facially driven VSD then is incorporated with the surgical scan data provided by the surgeon. The multiplicity of algorithms are accessed until an ideal file is established that contains an optimally designed prosthesis that will precisely fit, via screw retention, on the multi-unit abutments to secure a full-arch screw-retained provisional prosthesis.
The implant company then returned an STL design file electronically via email. The office staff sent this file to the practice's 3D printer, and the appropriate color nanoceramic resin was used to print the prosthesis at 100 microns. Next, metal titanium (ti)-base cylinders, made specifically for the multi-unit abutments, were inserted into the prosthesis, which was then stained and glazed, and gingival color was applied to establish optimum esthetics (Figure 5).
The completed provisional prosthesis was then screwed onto the multi-unit abutments with titanium screws and torqued to 20 Ncm. Screw-access holes were filled, and no occlusal adjustment was necessary. The fit of the prosthesis was precise and stable, and the patient's phonetics were ideal. The patient was overwhelmed by the significant esthetic improvement with this set of teeth in place (Figure 6 through Figure 8).
Home care was reviewed with the patient, which included use of a toothbrush and water flosser. An antibiotic, amoxicillin 500 mg three times a day, as well as ibuprofen 800 mg as needed, were prescribed. The patient was instructed to adhere to a soft diet and avoid hard food.
At 1 week postoperatively, it was noted that the patient sustained very little postoperative pain, and home care and dietary suggestions were reviewed.
Case 2
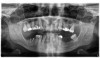
A 60-year-old female patient presented with many periodontally and restoratively hopeless teeth that severely compromised esthetics and function and were inadequate to retain a maxillary restoration. She declined to advance into a full maxillary denture or partial denture. Existing maxillary teeth included Nos. 2 and 4 through 14 (Figure 9 and Figure 10). The opposing dentition was stable. The patient was in good health with no allergies to medication.
At the initial visit, a panoramic x-ray (Figure 11) and periapical x-rays were taken. The patient was photographed to capture her full face and shoulders, and a digital scan of the maxillary dentition was obtained. This file was electronically sent to the implant company to complete the VSD.
A week later the patient presented for surgery for extraction and replacement of her existing maxillary dentition with implants and a screw-retained provisional implant restoration. Teeth Nos. 2, 4, and 6 through 11, 13, and 14 were carefully extracted with attention paid to retaining site dimensions. Immediate implants were inserted into sites Nos. 4, 6, 8, 11, and 13 with high insertion torques in excess of
40 Ncm. Subsequently, multi-unit abutments were placed on all the implants and torqued to 30 Ncm, and scan gauges were placed on implant Nos. 8 and 11 (Figure 12 and Figure 13).
A maxillary intraoral scan was obtained with a digital scanner capturing the two remaining teeth in sites Nos. 5 and 12 and the scan gauges on implants Nos. 8 and 11. Subsequently, teeth Nos. 5 and 12 were extracted. Scan gauges were placed on implants Nos. 4, 6, and 13. At this time, another intraoral scan was captured of all the scan gauges on the five implants with the surrounding soft tissues (Figure 14 and Figure 15).
These files were electronically sent to the implant company for AI calibration of the scan gauges, and then these files were incorporated into a VSD to create the ideal set of teeth for this patient that would precisely screw down onto the implants to restore the maxillary dentition. Restoration would encompass esthetics, function, and phonetics.
Several hours later the dental team received the STL file, from which they would print the maxillary prosthesis on a 3D printer using appropriately colored nanoceramic resin. The prosthesis was stained and glazed, and metal cylinders were inserted into the undersurfaces
of the screw-access holes, each of which was specifically located to fit on the multi-unit abutments (Figure 16 and Figure 17).
The prosthesis fit precisely on the multi-unit abutments, and multi-unit screws were used to secure the prosthesis in place at 20 Ncm (Figure 18 through Figure 20). The screw-access holes were filled, and the patient was instructed on dietary restrictions and adherence to a soft diet. Instructions for oral hygiene were given, and the patient was advised to use a water flosser daily. Analgesics included ibuprofen 800 mg, and for antibiotics, amoxicillin 500 mg three times a day was prescribed.
Postoperative x-rays documented the full seating of the prosthesis on the multi-unit abutments (Figure 21 and Figure 22). The patient returned at 1 week postoperatively for a follow-up visit and to review home care. She remarked that the restoration was comfortable and that she was free of discomfort and extremely pleased with the makeover she received in one day.
Case 3
A 67-year-old female patient presented with a highly compromised maxillary and mandibular dentition, including teeth Nos. 2 through 15, 17, 21 through 24, and 27 through 30. Soft tissues were of normal contour, and bone profiles were generally sustained and favorable. The patient was excited about the prospect of transforming both her maxillary and mandibular compromised esthetics and function in one visit. (Case 3 is depicted in Figure 23 through Figure 42.)
At the initial appointment, a panoramic x-ray and periapical x-rays were taken. As part of the protocol, photographs of the patient from head to shoulders were taken and scans of the teeth and soft tissue were captured with an intra-
oral scanner. These images were then sent electronically to the implant manufacturer, and three days later a VSD was provided for review and approval.
At the next visit, the patient was anesthetized with xylocaine with 1:100,000 epinephrine. Teeth Nos. 22, 27, and 28 were retained and all other mandibular teeth were extracted. Immediate implants were placed in prosthetically correct positions and multi-unit abutments were torqued to 30 Ncm. This was followed by insertion of screw-retained scan gauges in positions Nos. 18, 24, and 30.
In the maxillary arch, teeth Nos. 3, 7, 10, and 15 were retained and all other maxillary teeth were extracted. Immediate implants were placed prosthetically correctly with favorable insertion torques. Multi-unit abutments were placed on the implants, and scan gauges were secured to these multi-unit abutments in sites Nos. 6, 8, and 11. An intraoral scan following the protocol captured the location of the implants, with a reference to the remaining teeth and soft tissues. These files were then sent electronically to the proprietary web portal.
At the completion of surgery for the mandibular arch, teeth Nos. 17, 21 through 24, and 27 through 30 had been carefully extracted. Immediate implants with multi-unit abutments were placed in sites Nos. 21, 24, 28, and 30, and an additional implant with a multi-unit abutment was placed in site No. 18. All multi-unit abutments were torqued to 30 Ncm. In the maxillary arch, at the completion of surgery, teeth Nos. 2 through 15 had been carefully extracted. Immediate implants with multi-unit abutments were placed in sites Nos. 4, 6, 8, 11, and 13, and all multi-unit abutments were torqued to 30 Ncm.
The computer software then calibrated the precise implant position based on a unique DME file that was assigned with the scan gauge kit used for this procedure. The scan gauge data captured was used with proprietary AI software to establish exact multi-unit abutment positioning. The VSD designed presurgically was then incorporated with the surgical scan data provided by the surgeon. The multiplicity of algo-
rithms were accessed until an optimum file was established that contained the prosthesis design for this dentition that would precisely fit, via screw retention, on the multi-unit abutments to secure a full-arch screw-retained provisional prosthesis.
This file was then electronically returned to the dental team via the proprietary web portal. The office staff then sent the STL design file to the practice's 3D printer software, and the appropriate color nanoceramic resin was used to print the prosthesis at 100 microns. Once this was accomplished, the prosthesis was stained and glazed and gingival color was applied to establish optimum esthetics.
The completed prosthesis was then screwed directly onto the multi-unit abutments with Rosen screws with no ti-bases and torqued to 20 Ncm. Screw-access holes were filled, and no occlusal adjustment was necessary. The fit of the prosthesis was precise and stable and the phonetics of the patient was ideal. The patient was overwhelmed by the significant esthetic improvement with this set of teeth in place.
Home care was reviewed and included use of a toothbrush and water flosser. For an antibiotic, amoxicillin 500 mg three times a day was prescribed, along with ibuprofen 800 mg as needed as an analgesic. The patient was instructed to adhere to a soft diet and avoid hard food.
At the 1 week postoperative visit, it was noted that the patient sustained very little postoperative pain, and home care and dietary suggestions were reviewed.
Case 4
A 71-year-old female patient presented with a maxillary complete denture and a failing mandibular dentition. The patient wore an ill-fitting mandibular acrylic removeable partial denture to supplement her periodontally compromised mandibular teeth. She expressed a desire to improve the esthetics and function of her teeth and to replace her removeable partial denture with a fixed prosthesis. (Case 4 is depicted in Figure 43 through Figure 52.)
An initial appointment included a complete oral examination as well as a panoramic x-ray, CBCT scan, and intraoral surface scans of her maxilla and mandible. A comprehensive treatment plan included extraction of her mandibular teeth with immediate implant placement and insertion of a mandibular full-arch immediate fixed provisional restoration followed by a final mandibular full-arch fixed zirconia restoration.
The treatment began by addressing the patient's immediate concern, which was her mandibular situation. Her mandibular teeth were extracted, and immediate implants were placed and immediately provisionalized using a screw-retained PMMA provisional, which sat on multi-unit abutments.
After 6 months of healing (the patient delayed her final restorative treatment), the mandibular final restorative procedure was begun. A fully digital restorative protocol and workflow were followed. The first appointment for the final restoration workflow consisted of a series of intraoral scans and full-face photo-
graphy. The scans included the patient's maxillary denture, the mandibular temporary restoration that was seated in the patient's mouth, and the patient's bite.
The patient's mandibular temporary restoration was then removed from her mouth. A scan was taken of the mandibular multi-unit abutments and the surrounding soft tissue. Only the fixed soft tissue needed to be recorded, as only fixed tissue is repeatable. This type of intraoral scan is also known as the emergence profile scan.
Three implant scan bodies designed to replicate the multi-unit abutment position in the temporary were affixed to the fixed provisional restoration in the multi-unit positions with multi-unit screws. The positions were chosen to create a wide anterior-to-posterior spread. The provisional restoration with the implant scan bodies was then scanned 360 degrees.
The scan gauges were then placed onto the mandibular multi-units in the patient's mouth and retained with multi-unit screws. The choice of scan gauge height and lengths was per the fully digital restorative protocol. Two intraoral scan gauge scans were taken. The first was done in a right to left pass over the scan gauges, with care exercised to move forward in an arc so as not to go back over already-scanned segments. A second independent scan was done in a left to right arc, again with care taken not to scan any segment twice in the same scan. This completed the series of intraoral scans required to produce the restoration.
A full-face photograph was taken with the patient's upper and lower prostheses in place. This completed all the data required for the final prosthesis design.
This series of intraoral scans with the full-face photograph was uploaded to the proprietary portal with all questions regarding the case requirements answered. The provisional prosthesis had been carefully designed, and the request in the prescription was to duplicate the provisional design. The patient had been wearing this provisional for several months, so phonetics, esthetics, function, and occlusion had been well tested. This completed the prescription phase of the case, including sending the required data.
Four days later, the clinician received an email from the implant manufacturer requesting approval of the prosthesis design. Upon opening the email, a tool showing the proposed 3D design of the prosthesis was activated. All aspects of the prosthesis design were analyzed in three dimensions. Upon review of the design proposal and confirmation of the duplication of the provisional prosthesis design, approval was given to move forward with the final prosthesis fabrication.
Two weeks after design approval was given, the dental office received the final prosthesis. Included in the packaging were the final prosthesis, new multi-unit screws, oral hygiene aids appropriate for patient use with this type of prosthesis, and a warranty card.
When the patient presented for insertion of the final prosthesis, the provisional prosthesis was removed and the final prosthesis was inserted onto the multi-unit abutments. One multi-unit screw was placed with hand-tightening in the most distal position on the patient's left side. Periapical radiographs were taken paralleling the multi-unit abutment to the final prosthesis joint to confirm complete passive seating of the restoration. After confirming that the restoration sat passively and completely on the multi-unit abutments, the remainder of the multi-unit screws were inserted, and all were torqued to 20 Ncm using a torque driver. The occlusion was then evaluated; this included checking centric contact points as well as for lateral excursive and protrusive guidance.
The patient was then shown her new smile, and she approved of the comfort and esthetics of the restoration. Screw-access holes were filled with Teflon tape and covered with a flowable composite resin, completing the insertion visit. The final prosthesis fulfilled the needs for passive fit, favorable esthetics, occlusion, and phonetics.
Discussion
There continues to be a substantial North American population in need of full-arch dental
implant-supported rehabilitation for both edentulous and partially edentulous dentitions.22,23Techniques used to treat these patients begin at the diagnostic stage, continue through the surgical stage, and are finalized in the definitive prosthetic restoration.
There are multiple approaches to the surgical phase. The surgical approach used will influence the progression sequence of the case and the trauma sustained by the patient. Flapless immediate implant surgery was the protocol used in the cases documented here.
In this immediate implant surgical protocol, remaining teeth are extracted as atraumatically as possible, preserving bone and soft-tissue landmarks. This approach is key to site preservation.8,11,19Implant placement resulting in high insertion torques of 35 Ncm to 50 Ncm and, in some sites, 70 Ncm is accomplished by judicious site preparation and titration of insertion torque of the implants until high insertion torques are achieved.19 In some sites, milling of the bone is done to ensure accurate and full seating of multi-unit abutments. In all sites, the implants are placed in the best available bone and are prosthetically correct to the existing opposing or planned opposing dentition.
In conventional prosthetic procedures, upon completion of the surgery, multiple visits are typically required over many months, during which time the patient may be in a removeable prosthesis.24 Immediate implant provisionalization in full-arch restorations has been well documented to be highly successful with good clinical outcomes and is patient preferred.25,26Conventional prosthetic workflows may require analog impressions at the time of surgery with the pouring of stone models. The immediate provisional restoration may need direct relining of a conversion prosthesis intraorally immediately following implant surgery.27 These procedures require considerable expertise to achieve precise fit and proper occlusion and demand significant patient chairside time and intraoral manipulation.28 This approach can be challenging for both the clinician and patient after a tedious surgical procedure.29
A simple expeditious digital workflow as described here allows accurate digital recording of implant position and delivery of the provisional restoration in a timely manner on the day of surgery with minimal involvement
intraorally. Accurate digital capture of implant position for full-arch implant-supported restorations had previously been reported to be less than precise.30,31The protocol described in this article provides a predictable means for fabrication of the provisional restoration on the day of implant surgery and shortens treatment time and chairside challenges for both the clinician and patient.
The benefit of the digital workflow is even more pronounced in the fabrication of the final restoration. Commonly required steps for conventional fabrication and delivery of a final restoration include accurately recording the implant position, opposing arch, vertical dimension, and centric occlusal record. The model (analog or virtual) must be accurate to a level that can predictably produce a passively seated restoration. To assure accuracy and passive fit, a verification step and verification jig are frequently utilized. The clinician then must transfer the esthetic, phonetic, and restorative requirements for the final prosthesis to the laboratory. This is usually followed by final prosthesis fabrication and clinical insertion. Conventional techniques today require five to six patient appointments to produce an accurate, passively fitting prosthesis.32-34
The solution for prosthetic rehabilitation of the full-arch implant patient discussed here addresses the complexity of full-arch restoration by using a simple repeatable digital workflow. As few as two appointments may be needed to restore a full arch of implants with a fixed
implant-supported restoration. If a prosthesis
design try-in is required, it can be done by downloading and 3D printing the STL file of the designed final prosthesis. A three-appointment protocol is then required to incorporate the try-in of the printed prosthesis design. Phonetics, esthetics, and occlusion can be evaluated, and if there are any adjustments made, a simple scan of the modified try-in prosthesis is recorded and uploaded to the manufacturer portal. An immediate provisional as well as a try-in prosthesis can be implemented in the same day with 3D printing technology.
This protocol overcomes the difficulties of producing accurate passive restorations through novel AI-empowered geometric scan abutment designs, optimization of manufacturing tolerances to eliminate errors in the rendering of virtual implant position, implant position optimization software algorithms, and AI analy-
sis and design software for prosthesis design. The final prosthesis has a milled titanium bar to support the veneering material, which may be monolithic zirconia, monolithic zirconia layered with porcelain, or a milled bar veneered with acrylic. The restoration design, including the titanium milled bar and veneering material, may be as small as 6 mm in height from the soft tissue to the incisal edge.35
Having the ability to fabricate a full-arch prosthesis with a vertical thickness requirement reduced to 6 mm36 may eliminate the need for bone reduction for the purpose of structural integrity of the final prosthesis and, thus, eliminate the trauma of ridge reduction surgery. Occasionally, bone reduction may still be necessary to move the transition zone out of the smile line. However, if bone reduction is not necessary for restoration strength, the number of esthetic-zone transition issues is significantly reduced. Many cases that would have needed pink aprons to manage excessive tooth length and esthetic transition zones can now be managed with a crown-and-bridge style prosthesis with esthetic dimensioned teeth emerging from the patient's natural soft tissue. The prosthesis design that allows this minimal restoration thickness and good restoration strength is accomplished through a software design program that incorporates AI that applies structural mechanical engineering principles to dental restoration design.
With this protocol, the restorations are seated on multi-unit abutments and are available for most commonly used multi-unit systems. The restoration interface to the multi-unit abutment is through the titanium bar milled directly to the multi-unit abutment interface. No ti-bases are used, so potential errors from cementing a ti-base improperly, or the ti-base becoming uncemented, are eliminated.
Implant capture accuracy is predictably accomplished in this fully digital workflow. Previously, the digital capture of implant position for full-arch implant-supported restorations had reported limitations in accuracy.30,31 Many variables affect the production of an accurate virtual model, including the type of intraoral scanner used, geometric design of the scan body, scan body material, whether the scan body is one-piece or two-piece, position of the scan bodies, manufacturing tolerances of the scan bodies, scanning strategy, and operator experience.36-46 The full-arch solution described here uses a complete digital workflow that addresses accuracy issues of intraoral scanner type, scanning strategies, manufacturing tolerances of intraoral scan bodies, effect of implant and scan body position, scan body material, novel scan body design, and clinician experience. The manufacturer has demonstrated an average implant-to-implant linear discrepancy of sub-10 microns, which meets the requirement for a passively seating restoration.34,47-49 As a total solution, the recording of centric relation, vertical dimension, and transfer of prosthesis design parameter is accomplished within the scanning protocol. The use of AI algorithms, innovative design, careful clinical workflow strategies, and rigorous manufacturing procedures supports both the full-arch immediate implant provisionalization procedures as well as the final restorative solution.
The simple workflow uses basic intraoral scans for the fabrication of the immediate full-arch implant-supported provisional restoration, thereby eliminating the steps of intraoral manipulation required for immediate provisional restoration fabrication during implant surgery. The efficiency of this solution continues with the production of a highly accurate, predictable final restoration in two to three appointments.
Conclusion
A digital workflow was presented using highly accurate scan bodies, an innovative clinical protocol, and AI software resulting in the delivery of a passively fitting screw-retained 3D-printed provisional prosthesis on the day of implant surgery. This is followed by a fully digital restorative protocol resulting in efficient fabrication and insertion of the final prosthesis. These sequences represent a new standard of care in implant dentistry.
Acknowledgment
The authors acknowledge Donald Boyd and Dr. Michael Klein for their educational leadership; Melker Nilsson for selecting the author (DAG) in the initial launch of this discipline; Dr. Jonathan J. Gelb for his initiative and participation in the integration of this protocol into the author's (DAG) office; Christian Villar-
roel for equipment procurement; Terry Spaulding, Alexis Pantaleo, Donald Boyd, Dana Tatta, Vince Lancenese, and Tim Steinglass for their assistance in delivery of surgical and prosthetic care; Drs. Jeffrey Burns, Scott Merkelson, and Peter Sawka for their collaboration in Cases 1 through 3. Surgery and prosthetics were provided by Dr. David A. Gelb in Cases 1 through 3 and Dr. Michael Klein in Case 4.
About the Authors
David A. Gelb, DDS
Diplomate, American Academy of Periodontology; Fellow, Academy of Osseointegration; Fellow, American College of Dentists; Fellow, International College of Dentists; Fellow, Pierre Fauchard Academy; Private Practice, West Hartford, Connecticut
Michael Klein, DDS
Chief Technology Officer, Keystone Dental Group, Burlington, Massachusetts; Former Clinical Associate Professor, Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, New York; Diplomate, American Board of Oral Implantology/Implant Dentistry; Diplomate, International Congress of Oral Implantology; Fellow, Academy of Osseointegration; Private Practice, Cedarhurst, New York
Michael Tuckman
Founder, President, Osteon Medical, Melbourne, Australia
Queries to the author regarding this course may be submitted to authorqueries@broadcastmed.com.
References
1. Adell R, Lekholm U, Rockier B, Bränemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10(6):387-416.
2. Laney WR, Tolman DE, Keller EE, et al. Dental implants: tissue-integrated prosthesis utilizing the osseointegration concept. Mayo Clin Proc. 1986;61(2):91-97.
3. Bränemark PI, Hansson BO, Adell R, et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977;16:1-132.
4. Bränemark PI. Osseointegration and its experi-
mental background. J Prosthet Dent. 1983;50(3):
399-410.
5. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria for success. Int J Oral Maxillofac Implants. 1986;1(1):11-25.
6. van Steenberghe D. A retrospective multicenter evaluation of the survival rate of osseointegrated fixtures supporting fixed partial prostheses in the treatment of partial edentulism. J Prosthet Dent. 1989;61(2):217-223.
7. Pylant T, Triplett RG, Key MC, Brunsvold MA. A retrospective evaluation of endosseous titanium implants in the partially edentulous patient. Int J Oral Maxillofac Implants. 1992;7(2):195-202.
8. Zarb GA, Schmitt A. Osseointegration and the edentulous predicament. The 10-year Toronto study. Br Dent J. 1991;170(12):439-444.
9. Barzilay I, Graser GN, Caton J, Shenkle G. Immediate implantation of pure titanium threaded implants into extraction sockets [abstract]. J Dent Res. 1988;67:234.
10. Gelb DA. Immediate implant surgery: three-year retrospective evaluation of 50 consecutive cases. Int J Oral Maxillofac Implants. 1993;8(4):388-399.
11. Gelb DA, Lazzara RJ. Hierarchy of objectives in implant placement to maximize esthetics: use of pre-angulated abutments. Int J Periodontics Restorative Dent. 1993;13(3):277-287.
12. Gelb DA. Immediate implant surgery: ten-year clinical overview. Compend Contin Educ Dent. 1999;20(12):1185-1192.
13. Schnitman PA, Wöhrle PS, Rubenstein JE, et al. Ten-year results from Brånemark implants immediately loaded with fixed prostheses at implant placement. Int J Oral Maxillofac Implants. 1997;12(4):495-503.
14. Tarnow DP, Emtiaz S, Classi A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: ten consecutive case reports with 1- to 5-year data. Int J Oral Maxillofac Implants. 1997;12(3):319-324.
15. Grunder U. Immediate functional loading of immediate implants in edentulous arches: two-year results. Int J Periodontics Restorative Dent. 2001;21(6):545-551.
16. Gapski R, Wang HL, Mascarenhas P, Lang NP. Critical review of immediate implant loading. Clin Oral Implants Res. 2003;14(5):515-527.
17. Balshi SF, Wolfinger GJ, Balshi TJ. A prospective study of immediate functional loading, following the Teeth in a Day protocol: a case series of 55 consecutive edentulous maxillas. Clin Implant Dent Relat Res. 2005;7(1):24-31.
18. Bergkvist G, Nilner K, Sahlholm S, et al. Immediate loading of implants in the edentulous maxilla: use of an interim fixed prosthesis followed by a permanent fixed prosthesis: a 32-month prospective radiological and clinical study. Clin Implant Dent Relat Res. 2009;11(1):1-10.
19. Gelb DA. Unique benefits of immediate implants with immediate provisional restoration: outcome analytics from 26 years of documentation. Inside Dentistry. 2016;12(4):35-41.
20. Gelb DA. Benchmark for tooth replacement: immediate implant with immediate provisional restoration. Outcome analytics from 29 years of documentation. Compend Contin Educ Dent. 2018;39(7):469-481.
21. Yao CJ, Cao C, Bornstein MM, Mattheos N. Patient-reported outcome measures of edentulous patients restored with implant-supported removable and fixed prostheses: a systematic review. Clin Oral Implants Res. 2018;29 suppl 16:241-254.
22. Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health. Int J Dent. 2013;2013:498305.
23. Al-Rafee MA. The epidemiology of edentulism and the associated factors: a literature review. J Family Med Prim Care. 2020;9(4):1841-1843.
24. Howe L, Barrett V, Palmer P. Dental implants. 7. Basic restorative techniques. Br Dent J. 1999;187(9):473-479.
25. Santosa RE. Provisional restoration options in implant dentistry. Aust Dent J. 2007;52(3):234-242.
26. Cordaro L, Torsello F, Ercoli C, Gallucci G. Transition from failing dentition to a fixed implant-supported restoration: a staged approach. Int J Periodontics Restorative Dent. 2007;27(5):481-487.
27. Kammeyer G, Proussaefs P, Lozada J. Conversion of a complete denture to a provisional implant-supported, screw-retained fixed prosthesis for immediate loading of a completely edentulous arch. J Prosthet Dent. 2002;87(5):473-476.
28. Benting D. A step-by-step guide to converting denture to interim hybrid prosthesis. Spear Education website. April 30, 2018. https://www.speareducation.com/spear-review/2015/11/a-step-by-step-guide-to-converting-denture-to-interim-hybrid-prosthesis. Accessed March 24, 2023.
29. Dixon RD. A predictable immediate denture conversion technique. Dentistry Today website. November 1, 2017. https://www.dentistrytoday.com/a-predictable-immediate-denture-conversion-technique/. Accessed March 24, 2023.
30. Mangano FG, Hauschild U, Veronesi G, et al. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: a comparative in vitro study. BMC Oral Health. 2019;19(1):101.
31. Knechtle N, Wiedemeier D, Mehl A, Ender A. Accuracy of digital complete-arch, multi-implant scans made in the edentulous jaw with gingival movement simulation: an in vitro study. J Prosthet Dent. 2022;128(3):468-478.
32. Todescan FF, Hayashi MM, Giugni LR, et al. From denture to the final implant-supported prosthesis using a full-digital protocol: a dental technique. Oral. 2021;1(4):332-339.
33. Ashurko I, Trofimov A, Tarasenko S, Mekhtieva S. Full-mouth screw-retained implant-supported rehabilitation with multiunit abutments using virtual guided surgery and digital prosthetics protocol. Case Rep Dent. 2020;2020:3585169.
34. Jemt T, Rubenstein JE, Carlsson L, Lang BR. Measuring fit at the implant prosthodontic interface. J Prosthet Dent. 1996;75(3):314-325.
35. El-Haddad H, Judge RB, Abduo J, Palamara J. Laboratory evaluation of novel implant metal-acrylic prosthesis design: influence of monolithic acrylic veneer. Int J Oral Maxillofac Implants. 2020;35(1):100-106.
36. Arcuri L, Pozzi A, Lio F, et al. Influence of implant scanbody material, position and operator on the accuracy of digital impression for complete-arch: a randomized in vitro trial. J Prosthodont Res. 2020;64(2):128-136.
37. Mangano FG, Admakin O, Bonacina M, et al. Trueness of 12 intraoral scanners in the full-arch implant impression: a comparative in vitro study. BMC Oral Health. 2020;20(1):263.
38. Çakmak G, Yilmaz H, Trevino Santos A, et al. Effect of scanner type and scan body location on the accuracy of mandibular complete-arch digital implant scans: an in vitro study. J Prosthodont. 2022;31(5):419-426.
39. Mizumoto RM, Yilmaz B. Intraoral scan bodies in implant dentistry: a systematic review. J Prosthet Dent. 2018;120(3):343-352.
40. Motel C, Kirchner E, Adler W, et al. Impact of different scan bodies and scan strategies on the accuracy of digital implant impressions assessed with an intraoral scanner: an in vitro study. J Prosthodont. 2020;29(4):309-314.
41. Mizumoto RM, Alp G, Özcan M, Yilmaz B. The effect of scanning the palate and scan body position on the accuracy of complete-arch implant scans. Clin Implant Dent Relat Res. 2019;21(5):987-994.
42. Schmidt A, Billig JW, Schlenz MA, et al. Influence of the accuracy of intraoral scanbodies on implant position: differences in manufacturing tolerances. Int J Prosthodont. 2019;32(5):430-432.
43. Lerner H, Nagy K, Luongo F, et al. Tolerances in the production of six different implant scanbodies: a comparative study. Int J Prosthodont. 2021;34(5):591-599.
44. Mizumoto RM, Yilmaz B, McGlumphy EA Jr,
et al. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J Prosthet Dent. 2020;123(1):96-104.
45. Imburgia M, Kois J, Marino E, et al. Continuous scan strategy (CSS): a novel technique to improve the accuracy of intraoral digital impressions. Eur J Prosthodont Restor Dent. 2020;28(3):128-141.
46. Dias Resende CC, Quirino Barbosa TA, Moura GF, et al. Influence of operator experience, scanner type, and scan size on 3D scans. J Prosthet Dent. 2021;125(2):294-299.
47. Full Mouth Digital Implant Impressions - A New Novel Approach [white paper]. Osteon Medical; August 5, 2020. Version 1.2.
48. Buzayan MM, Yunus NB. Passive fit in screw retained multi-unit implant prosthesis understanding and achieving: a review of the literature. J Indian Prosthodont Soc. 2014;14(1):16-23.
49. Brånemark PI, Zarb GA, Albrektsson T. Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry. Quintessence Publishing; 1985:99-115.