You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Institutional racism, a form of racism embedded through laws and regulations within society; White privilege, the societal privilege benefitting white people over non-white people in some societies; and unconscious or conscious biases have become increasingly important topics in the United States (US). The effects of these types of constructs contribute to racial inequality and can be seen in many different sectors including employment and health care.2 In addition, the US population is experiencing a demographic shift towards increased diversity. Currently, the US Census Bureau estimates that of 328 million American inhabitants, approximately 13% are African American, 6% Asian, 0.2% Native Hawaiian or Other - Pacific Islander, 3% two or more races, and 19% Latino or Hispanic.3 While the population diversifies, 64% of health care providers are predominately White.4 Moreover, research suggests, in the future, caregiver/patient interactions will be in cross racial/cultural dyads.5 These demographic shifts highlight a need for the delivery of ethnically and culturally competent health care, including oral health care, to meet the needs of a diversifying population.
The Institute of Medicine (IOM) publication, Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,investigated health care disparities and the role of bias and stereotyping at the patient, institutional, and health care system level.6 In this report, the IOM found minority groups were less likely to receive cardiac medications or be given proper treatment following a cardiac event,7 less likely to receive testing, screening, or pain medication for cancer,6,8 less likely to receive kidney dialysis or transplant,9 and less likely to receive antiviral HIV drugs,10 among other care issues. The report also identified differences in delivery of care to minority populations at a disproportionate rate.6 This has been a historical trend, with African American populations receiving lower quality of care compared to White counterparts.6,7,10-15 Research has also found that some of these disparities extend beyond treatment and care decisions such as minority groups receiving different communication from health care providers.11,13 Health care providers may spend less time during appointments with minority patients, infrequently ask patient opinions about treatment decisions, and use a more verbal dominant tone, all contributing to minority patients finding their care to be less patient-centered.11,13 Ultimately, the findings of this report support that implicit bias and discrimination were contributing factors affecting health care providers and their patient care decisions.6
Implicit biases may manifest in non-verbal behaviors such as eye contact and posture or proximity, and often represent a dissociation between what a person outwardly believes and what is deeply-seated in their thoughts/actions.16,17 Implicit biases are different than overt or explicit racism, they are often an automatic, unconscious, unknown negative thought or attitude toward a minority group and can profoundly affect clinical decision-making.18,19 The presence of these biases among health care providers and the effects on quality of care are concerning, as a clinician may not recognize these deeply seeded thoughts or actions and how they affect their ability to deliver impartial care. Additionally, these biases may operate at a disadvantage to an already vulnerable patient population.18 Implicit biases have been researched extensively in health care; however, there is a lack of literature in the dental profession. For example, one study examined inherent biases related to race and the effects on dentists' decisions to restore teeth.20 Dentists were given a clinical scenario along with photographs of a Black and White patient and a decayed tooth. Biases were measured though an explicit questionnaire related to how they would treat the patient as well as Implicit Associations Tests (IAT) to measure inherent biases. The study found that overall, dentists were significantly more likely to recommend root canal therapy (RCT) to White patients and significantly more likely to recommend extraction for Black patients instead of a restoration.20 Additionally, 91% of participants scored high on the race preference IAT test and 79% scored high on the race dental cooperative IAT test demonstrating pro-White biases for both IAT tests, and indicating that racial biases might influence the quality of dental care received by Black patients.20
A type of contemporary implicit bias, color-blind racial attitudes, may explain current research findings related to differing care and implicit biases. Color-blind racial ideology can be described as a set of beliefs used to make sense of social categories involving race that emphasizes sameness and does not implicate individuals who are White in racism.1,21,22 Moreover, a color-blind ideology focuses on the belief that racism is a concept of the past and all persons have equal opportunities in contemporary society.1,21 Those who subscribe to this ideology hold the belief that the color of a person's skin is not seen, everyone is equal, and further opposes the view that racism is an ongoing societal problem.21 This ideologic perspective is further explained as one that assumes class and culture, not institutional racism, are responsible for social inequities.23 Research suggests when evaluated, health care providers with higher color-blind racial ideology scores may engage in racially insensitive behavior and exhibit an increase in negative emotions and a lack of ethnocultural empathy.21,24-27 Additionally, research suggests individuals subscribing to color-blind habits may show higher levels of biases on implicit and explicit measures of racism such as IATs.25 All health care should be delivered objectively while taking into consideration the unique characteristics of each patient; however, it is possible some health care providers may exhibit high color-blindness that may be linked to a lack of impartial care.
Although color-blind racial attitudes have been researched in other disciplines, minimal data is available in the dental profession, with only one study in dental hygiene on a student population from one institution in Virginia.28-30 Ludwig et al. examined the prevalence of color-blind racial attitudes in dental hygiene students (n=70).30 The results revealed over one-half (65%) of the study participants possessed moderate levels of color-blind racial attitudes, indicating a lack of awareness of White privilege and cultural competence.30 The researchers recommended expanding the sample size to more fully conceptualize color-blind racial attitudes in dental hygienists. Awareness of color-blindness is an important first step in promoting equities in health care and combatting social injustices which may affect dental hygiene care delivery to diverse populations. Therefore, the purpose of this study was to investigate color-blind racial attitudes in a national sample of dental hygienists in the US.
Methods
This study was determined to be exempt (1673546-2) by the Old Dominion University Institutional Review Board (IRB). A convenience sample of dental hygienists who were recruited via social media sites and a non-probability sampling technique was used for a cross-sectional survey. Snowballing was used to enlist participants in the study. The 24-item survey was administered online (Qulatrics; Provo, UT, USA). Administrators/moderators of dental hygiene Facebook groups were asked for approval to post the survey invitation. Upon approval, a link to the survey instrument was posted on an array of dental hygiene related social media sites. All responses were collected anonymously; voluntary informed consent was understood upon return of the survey. Data collection was performed over a six-week period.
Survey Instrument
The 20-item Color-Blind Racial Attitudes Scale (CoBRAS), a valid and reliable instrument developed by Neville et al.,22 was used to measure color-blind racial ideology in three subcategories. The first category, Racial Privilege, is comprised of seven items and assesses the blindness of persons to the existence of White Privilege. The seven-item second category, Institutional Discrimination, determines recognition of the implications of institutional forms of racial discrimination, and third category, Blatant Racial Issues, consists of the six questions designed to measure awareness of general pervasive racial discrimination. Participants used a 6-point Likert scale ranging from strongly disagree (1) to strongly agree (6), to determine level of agreement or disagreement with the 20 statements. Responses were added to obtain subscale and overall scores with total scores on CoBRAS ranging from 20-120 and subscale scores ranging from 7-42. Higher scores indicate higher levels of denial or unawareness of racism. Overall scores ranging from 20-53.3 indicate low unawareness, 53.4-83.7 moderate unawareness, and 83.3-120 high unawareness. Subscale scores ranging from 7-18.6 indicate low unawareness, 18.7-30.3 moderate unawareness, and 30.4-42 high unawareness. In addition to the CoBRAS, five demographic questions were also included (age, gender, ethnicity, geographic location, and education level) in the survey.
Statistical Analysis
A statistical power analysis and effect size (medium effect size; =0.25) was performed.31 The projected sample size needed for an alpha =.05, power =.80, and a medium effect size (G*Power 3.1), was approximately n=231. Descriptive statistics were used to evaluate the means between groups. Separate one-way between subject's ANOVA were used to determine statistically significant differences (p<0.05)among dental hygienist participants based on age, ethnicity, geographic location, and level of education. If Levene's statistic was significant and violated the assumption of homogeneity of variance, the F-statistic was adjusted and reported using Welch's F,and Games-Howell post hoc tests were utilized to find significant differences between groups.
Results
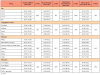
Two hundred and seventy-two dental hygienists participated in the study; 39 surveys were not used due to incomplete data, yielding a participation rate of 86% (n=233). Most respondents (96%, n=224) were women, one-third of participants (36%, n=85) were between the ages of 30-44 and one-third (33%, n=76) were aged 45-59. Nearly half of participants (48%, n=111) had a four-year degree, 39% (n=91) held a two-year degree, and 11% (n=26) held a master's degree. Geographically, almost half of participants (46%, n=106) were from the South and most participants were White (71%, n=166). Demographic characteristics are displayed in Table I.
Results revealed an overall average score of 54.04 on the CoBRAS questionnaire indicating overall moderate unawareness of racism among participants (Table II). When comparing overall CoBRAS means among the group demographics of geographic location and education, no statistically significant differences were found (p's>0.05). However, when comparing age groups, ANOVA revealed a statistically significant difference (F(3, 99.844)=4.076, p=.009).
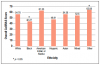
Games-Howell post hoc test revealed participants aged 18-29 had significantly lower overall CoBRAS scores when compared to participants aged 60 and over (x=49.41, x=59.17, respectively; p=.019). Additionally, ANOVA revealed a statistically significant finding related to ethnicity (F(6, 226)=2.561, p=.020). Tukey post hoc tests revealed participants of African American ethnicity had significantly lower overall CoBRAS scores compared to those who identified in the Other ethnicity category (x=42.27, x=62.08, respectively; p=.029) (Figure 1).
CoBRAS subscales were also compared among group demographics of age, ethnicity, level of education, and geographic location. Participant average score on the racial privilege subscale was 16.80, indicating low unawareness of White racial privilege. When comparing means among group demographics of age, level of education, and geographic location on the racial privilege subscale, no statistically significant differences were found (p's>0.05). When comparing ethnicity groups, ANOVA revealed a statistically significant difference between ethnicity groups (F(6, 226)=2.541, p=.021), however Tukey post hoc tests showed that there was no significant difference between any ethnicity groups (Table III).
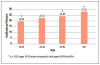
The overall average score on the institutional racism subscale was 23.56, indicating moderate unawareness of the implications of institutional types of racism (Table II). When comparing means among group demographics of level of education and geographic location, no statistically significant differences were found (p's>0.05). However, when comparing age groups, ANOVA revealed statistically significant differences (F(3,100.849)=7.443, p<.001). Games-Howell post hoc test revealed participants aged 18-29 had significantly lower scores on the institutional racism scale compared to participants aged 45-59 and 60 and older (x=19.29, x=24.87, x=27.03, respectively; p=.004 and <.001). Additionally, participants aged 30-44 had significantly lower institutional racism scores compared to those 60 and older (x=22.42, x=27.03, respectively; p=.019) (Figure 2). When comparing ethnicity groups, ANOVA revealed a statistically significant difference between ethnicity groups (F(6, 226)=2.239, p=.041), however, Tukey post hoc tests showed there was no significant difference between an individual group (Table III).
Finally, the overall average score on the blatant racial issues subscale was 13.87, indicating low unawareness of more overt, pervasive racism. When comparing group means among demographics of age, level of education, and geographic location, no statistically significant differences were found (p's>0.05). However, when comparing ethnicity groups on the blatant racial issues scales, ANOVA revealed a statistically significant difference (F(6, 226)=2.234, p=.041). Tukey post hoc test revealed participants of Hispanic ethnicity scored significantly lower on the blatant racial issues scale compared to those in the Other ethnicity category (x=11.00, x=17.17, respectively; p=0.048).
Discussion
Biases in health care providers may influence patient-provider relationships, hiring and promotion practices, decision making, treatment, and interpersonal communication thereby perpetuating health inequities.6-15,18,19 Striving to mitigate both explicit and implicit bias is important for all clinicians including oral health care providers and starts with awareness. Refusing to acknowledge differing values, traditions, and racial identities creates obstacles to acceptance and serves as a barrier when addressing the negative impact of racial discrimination and health care.32 This study investigated the prevalence of one form of implicit bias, color-blind racial attitudes in dental hygienists in the US. Overall participant CoBRAS questionnaire scores indicate moderate levels of denial/unawareness of racism. These findings were similar to previous studies among dental and dental hygiene students.28-30 Interestingly, average subscale scores of participants indicated moderate unawareness in only one subcategory, institutional racism.
Participants scored in the low unawareness range for the subscales unawareness of racial privilege and awareness of blatant racial issues, meaning they were aware of White racial privilege and aware of more explicit forms of racism. These subscale findings were slightly different from previous studies of dental and dental hygiene students where participants were moderately unaware of both institutional racism and White racial privilege, which are considered to be more implicit types of color-blind ideology.28-30 Previous research of color blind racial attitudes in students who scored moderate in the White racial privilege scale could be a result of White students experiencing less racial discrimination and less interracial tensions and recognition of racial conflict.33 Institutional racism exists in unfair policies and institutional culture resulting in differing access to goods and services, including health and dental care for minority groups.34,35 Institutional racism is difficult to detect and research suggests it is rarely visible by those privileged by it.1,35 Perhaps the practicing dental hygienists in this study, being older and having more life experience, have experienced or witnessed racial discrimination which resulted in their awareness of White racial privilege but unawareness of those negatively impacted by institutional racism, resulting in their moderate scores on this subscale.
The results also showed that older participants (60+) scored significantly higher on the overall CoBRAS questionnaire as well as the institutional discrimination subscale. Additionally, younger participants, aged 18-29, scored in the low unawareness range on the overall CoBRAS questionnaire, indicating they were more aware of the overall implications of racism. For the institutional discrimination subscale, older participants (45-49 and 60+) were significantly more unaware of institutional types of racism compared to those in the 18-29-year-old age group and the 30-44-year-old age group. These findings suggest older participants may be more unaware of the existence of racism as well as the racial inequalities that exist at a societal, political, and economic level.36,37 Perhaps these findings can be explained as a product of the culture in which these participants were raised. They could also be related to aging as research suggests the ability to suppress a thought or bias intentionally and unintentionally from consciousness, declines with age.38-40
There is also evidence suggesting that older adults show greater implicit prejudice than younger adults and the loss of inhibition that occurs with aging may play an important role in activation of those implicit prejudices.38-40 Additionally, the life experiences of younger individuals in this study along with recent media coverage of implicit and explicit bias may have increased their awareness of racial inequalities.41 Importantly, institutional forms of racism may affect oral health care delivery and some dental hygienists may need to practice effortful inhibitory processes, as well as stereotype suppression, to replace implicit thoughts on institutional racism with more egalitarian thoughts.42 These efforts may produce a positive impact in reducing some barriers to care for diverse population groups. A greater understanding of the unconscious dynamics operating within a color-blind ideology may lead to challenges in understanding how these biases affect the unbiased delivery of dental hygiene care.43
Participant's race played a significant role in overall CoBRAS scores as well as scores on the blatant racial issues subscale. African American participants scored significantly lower on overall CoBRAS scores compared to those in the Other ethnicity category. Moreover, African American participants' overall CoBRAS scores fell in the low unawareness range. Hispanic participants also scored significantly lower on the blatant racial issues subscale compared to participants in the Other ethnicity category. Hispanic participant average scores on this subscale also fell in the low unawareness range as compared to the moderate range for the Other ethnicity category. Race also played a significant role on the racial privilege subscale with American Indian or Alaska Native and Asian participants scoring the highest on this subscale, in the moderate unawareness range. Often, indigenous, Black, and other minority Americans have faced the most severe oppression and repression in everyday instances within these systems and in the past.44,45 Findings from this study were interesting because as minority ethnicities, American Indian and Alaska Native and Asian participants scored in the moderate range on the racial privilege subscale. Research suggests being able to ignore, dismiss, or truly believe privilege does not exist, stems from receipt of that privilege.1 It is possible this subset of participants have not experienced biases based on their ethnicity which led to their unawareness related to White racial privilege.
In contrast, the African American and Hispanic participants in this study may have been subject to biases based on their ethnicity which led to more awareness and low scores on both the overall CoBRAS and blatant racial issues subscale. These findings were significant as research has indicated racially concordant health care interactions are associated with more positive health care interactions related to communication as well as utilization of health care services.46-48 Dental hygienists will encounter increasing diversity in their patient pool as the US population diversifies across the country. Hence, contemporary oral health care professionals need to increase personal awareness of biases as an important step in providing impartial care to patients from all ethnicities.49 Unless dental hygienists address biases such as color-blindness, oral health disparities may continue. Moreover, as in dentistry, greater diversity in the dental hygiene workforce is needed and, at the same time, increased understanding of the implications of racism by current practitioners may increase and improve access to high-quality oral health care.
Health care providers, including dental hygienists, may harbor color-blind racial attitudes in an effort to promote objectivity in oral health care delivery; however, research indicates these attitudes perpetuate barriers and is negatively associated with multicultural knowledge and empathy.21,26,27 Research suggests the attitudes of health care providers and their effect on health disparities are relevant and require further examination.6 As a part of diversity training in the education experience, dental hygiene programs might consider adding curriculum content and training programs related to increasing awareness of biases and stereotyping as well as information on gaining an understanding of how personal attitudes affect patient care. Instilling a lifelong commitment to evaluating how personal biases and assumptions may affect the oral health care they deliver to individuals of varying ethnicities and backgrounds is important. Continuing education courses that help participants recognize and evaluate colorblind ideologies is also suggested as an important strategy for mitigating bias in the delivery of oral health care by current clinicians. Equity training may make counterproductive color-blind language and attitudes more transparent and foster more equitable and inclusive oral health care.50
Limitations
Several limitations could have influenced the results of this study. Upon viewing the survey invitation, dental hygienists familiar with color-blind ideologies may have been more likely to respond, which may have impacted the results. Other dental hygienists may have felt they did not understand the concept well enough or felt the topic was too controversial to respond. Future studies could include a brief synopsis of color-blind ideology in the invitation letter with a short explanation of the importance of participation. This could increase the response rate for future studies. Research focused on how dental hygienists' color-blind attitudes affect patient care is suggested as a starting point in addressing oral health inequities associated with bias. Future studies should also focus on education and intervention strategies specifically designed for oral health care professionals to assist with understanding and mitigating personal bias whether it is implicit or explicit.
Conclusion
Participants scores revealed moderate unawareness of the implications of a color-blind ideology on racism and older participants scored significantly higher on the institutional racism subscale compared to younger participants. African American and Hispanic participants were more aware of explicit forms of racism and American Indian or Native Alaskan and Asian participants were more unaware of White racial privilege. Findings underscore the need for more research to better understand how a color-blind ideology affects dental hygiene care. Awareness of color-blindness in oral health care professionals may be an important initial step in promoting more equitable delivery of care to increasingly diverse patient populations now and in the future.
Emily A. Ludwig, RDH, MS is an assistant professor; Susan L. Tolle, RDH, MS is a professor; Jessica R. Suedbeck, RDH, MS is an assistant professor; all at the Gene W. Hirschfeld School of Dental Hygiene, Old Dominion University, Norfolk, VA, USA.
References
1. Juric MK, Ghimire S, Ogonek J, et al. Milestones of hematopoietic stem cell transplantation - from first human studies to current developments. Front Immunol. 2016 Nov; 7:470.
2. Phelan R, Arora, M., Chen, M. Current use and outcome of hematopoietic stem cell transplantation: CIBMTR US summary slides. Center for International Blood & Bone Marrow Transplant Research, 2020.
3. D'Souza A, Lee S, Zhu X, Pasquini M. Current use and trends in hematopoietic cell transplantation in the United States. Biol Blood Marrow Transplant. 2017 Sep;23(9):1417-21.
4. Gooley TA, Chien JW, Pergam SA, et al. Reduced mortality after allogeneic hematopoietic-cell transplantation. N Engl J Med. 2010 Nov;363(22):2091-101.
5. Wingard JR, Majhail NS, Brazauskas R, et al. Long-term survival and late deaths after allogeneic hematopoietic cell transplantation. J Clin Oncol. 2011 Jun;29(16):2230-9.
6. Martin PJ, Counts GW, Jr, Appelbaum FR, et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation. J Clin Oncol. 2010 Feb;28(6):1011-6.
7. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: the 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. 2015 Mar;21(3):389-401.
8. Georges GE, Bar M, Onstad L, et al. Survivorship after autologous hematopoietic cell transplantation for lymphoma and multiple myeloma: late effects and quality of life. Biol Blood Marrow Transplant. 2020 Feb(2):407-12.
9. Majhail NS, Rizzo JD, Lee SJ, et al. Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2012 Mar;18(3):348-71.
10. Léger CS, Nevill TJ. Hematopoietic stem cell trans-plantation: a primer for the primary care physician. CMAJ. 2004 May;170(10):1569-77.
11. Jenq RR, van den Brink MRM. Allogeneic haematopoietic stem cell transplantation: individualized stem cell and immune therapy of cancer. Nat Rev Cancer. 2010 Mar;(3):213-21.
12. Martinez-Cibrian N, Zeiser R, Perez-Simon JA. Graft-versus-host disease prophylaxis: pathophysiology-based review on current approaches and future directions. Blood Rev. 2021 Jul;48.
13. Elad S, Raber-Durlacher JE, Brennan MT, et al. Basic oral care for hematology-oncology patients and hematopoietic stem cell transplantation recipients: a position paper from the joint task force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) and the European Society for Blood and Marrow Transplantation (EBMT). Support Care Cancer. 2015 Jan;23(1):223-36.
14. Chaudhry HM, Bruce AJ, Wolf RC, et al. The incidence and severity of oral mucositis among allogeneic hematopoietic stem cell transplantation patients: a systematic review. Biol Blood Marrow Transplant. 2016 Apr;22(4):605-16.
15. Rankin KV, Epstein J, Huber MA, et al. Oral health in cancer therapy. Tex Dent J 2009 May;126(5):389-97, 406-19, 422-37.
16. Arora M, Klein JP, Weisdorf DJ, et al. Chronic GVHD risk score: a Center for International Blood and Marrow Transplant Research analysis. Blood. 2011 Jan;117(24):6714-20.
17. Meier JKH, Wolff D, Pavletic S, et al. Oral chronic graft-versus-host disease: report from the International Consensus Conference on clinical practice in cGVHD. Clin Oral Investig. 2011 Apr(2):127-39.
18. Lee SJ. Classification systems for chronic graft-versus-host disease. Blood. 2017 Jan;129(1):30-7.
19. Majhail NS, Tao L, Bredeson C, et al. Prevalence of hematopoietic cell transplant survivors in the United States. Biol Blood Marrow Transplant. 2013 Oct;19(10):1498-501.
20. Lee SJ, Wolff D, Kitko C, et al. Measuring therapeutic response in chronic graft-versus-host disease. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: IV. the 2014 response criteria working group report. Biol Blood Marrow Transplant. 2015 Jun;21(6):984-99.
21. Bar M, Sandmaier B, Inamoto Y, et al. Donor lymphocyte infusion for relapsed hematological malignancies after allogeneic hematopoietic cell transplantation: prognostic relevance of the initial CD3+ T cell dose. Biol Blood Marrow Transplant. 2013 Jun;19(6):949-57.
22. Zecca M, Prete A, Rondelli R, et al. Chronic graft-versus-host disease in children: incidence, risk factors, and impact on outcome. Blood. 2002 Aug 15;100(4):1192-200.
23. Vogelsang GB, Lee L, Bensen-Kennedy DM. Pathogenesis and treatment of graft-versus-host disease after bone marrow transplant. Annu Rev Med. 2003;54:29-52.
24. Tiercy JM. HLA-C incompatibilities in allogeneic unrelated hematopoietic stem cell transplantation. Front Immunol. 2014 May;5:216.
25. Wolff D, Lawitschka A. Chronic graft-versus-host disease. In: Carreras E, Dufour C, Mohty M, Kröger N, editors. The EBMT handbook: hematopoietic stem cell transplantation and cellular therapies. 7th ed. Cham (CH): Springer; 2019. Chapter 44, Chronic Graft-Versus-Host Disease; p. 331-45.
26. Ferrara JL, Reddy P. Pathophysiology of graft-versus-host disease. Semin Hematol. 2006 Jan;43(1):3-10.
27. Cooke KR, Luznik L, Sarantopoulos S, et al. The biology of chronic graft-versus-host disease: a task force report from the National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2017Feb;23(2):211-34.
28. Arai S, Jagasia M, Storer B, et al. Global and organ-specific chronic graft-versus-host disease severity according to the 2005 NIH consensus criteria. Blood. 2011 Oct;118(15):4242-9.
29. Lee SJ, Flowers ME. Recognizing and managing chronic graft-versus-host disease. Hematology Am Soc Hematol Educ Program. 2008:134-41.
30. Mays JW, Fassil H, Edwards DA, et al. Oral chronic graft-versus-host disease: current pathogenesis, therapy, and research. Oral Dis. 2013 May;19(4):327-46.
31. Treister N, Duncan C, Cutler C, Lehmann L. How we treat oral chronic graft-versus-host disease. Blood. 2012 Oct;120(17):3407-18.
32. Treister N, Chai X, Kurland B, et al. Measurement of oral chronic GVHD: results from the chronic GVHD consortium. Bone Marrow Transplant. 2013 Aug;48(8):1123-8.
33. Fassil H, Bassim CW, Mays J, et al. Oral chronic graft-vs.-host disease characterization using the NIH scale. J Dent Res. 2012 Jul;91(7 Suppl):45s-51s.
34. Carpenter PA, Kitko CL, Elad S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: V. the 2014 ancillary therapy and supportive care working group report. Biol Blood Marrow Transplant. 2015 Jul;21(7):1167-87.
35. Hseih R, de Souza, MM, de Paula, F, et al. Oral chronic graft-versus-host disease: a short review. Trends transplant. 2016 Jan; 91(1):1-4.
36. Schubert MM, Correa ME. Oral graft-versus-host disease. Dent Clin North Am. 2008 Jan;52(1):79-109.
37. Curtis RE, Rowlings PA, Deeg HJ, et al. Solid cancers after bone marrow transplantation. N Engl J Med. 1997 Mar;336(13):897-904.
38. Rizzo JD, Curtis RE, Socié G, et al. Solid cancers after allogeneic hematopoietic cell transplantation. Blood. 2009 Jan 29;113(5):1175-83.
39. Haverman TM, Raber-Durlacher JE, Raghoebar, II, et al. Oral chronic graft-versus-host disease: what the general dental practitioner needs to know. J Am Dent Assoc. 2020 Nov;151(11):846-56.
40. Dowd FJ. Saliva and dental caries. Dent Clin North Am. 1999 Oct;43(4):579-97.
41. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007 Jan 6;369(9555):51-9.
42. Mawardi H, Hashmi SK, Elad S, et al. Chronic graft-versus-host disease: Current management paradigm and future perspectives. Oral Dis. 2019 May(4):931-48.
43. Mawardi H, Elad S, Correa ME, et al. Oral epithelial dysplasia and squamous cell carcinoma following allogeneic hematopoietic stem cell transplantation: clinical presentation and treatment outcomes. Bone Marrow Transplant. 2011 Jun;46(6):884-91.
44. Bassim CW, Fassil H, Mays JW, et al. Validation of the National Institutes of Health chronic GVHD oral mucosal score using component-specific measures. Bone Marrow Transplant. 2014 Jan(1):116-21.
45. Gomes AO, Torres SR, Maiolino A, et al. Early and late oral features of chronic graft-versus-host disease. Rev Bras Hematol Hemoter. 2014 Jan-Feb;36(1):43-9.
46. Bollero P, Passarelli PC, D'Addona A, et al. Oral management of adult patients undergoing hematopoietic stem cell transplantation. Eur Rev Med Pharmacol Sci. 2018 Feb;22(4):876-87.
47. Ashe TE, Elter JR, Southerland JH, et al. North Carolina dental hygienists' assessment of patients' tobacco and alcohol use. J Dent Hyg. 2005 Spring;79(2):9.
48. Kuten-Shorrer M, Woo SB, Treister NS. Oral graft-versus-host disease. Dent Clin North Am. 2014 Apr;58(2):351-68.
49. Lewis MAO, Williams DW. Diagnosis and management of oral candidosis. Br Dent J. 2017 Nov;223(9):675-81.
50. Quindós G, Gil-Alonso S, Marcos-Arias C, et al. Therapeutic tools for oral candidiasis: current and new antifungal drugs. Med Oral Patol Oral Cir Bucal. 2019 Mar;24(2):e172-80.
51. Singhal S, Powles R, Treleaven J, et al. Pilocarpine hydrochloride for symptomatic relief of xerostomia due to chronic graft-versus-host disease or total-body irradiation after bone-marrow transplantation for hematologic malignancies. Leuk Lymphoma. 1997 Feb;24(5-6):539-43.
52. Couriel D, Carpenter PA, Cutler C, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: V. the 2014 ancillary therapy and supportive care working group report. Biol Blood Marrow Transplant. 2006 Apr;12(4):375-96.
53. Carpenter PA, Schubert MM, Flowers ME. Cevimeline reduced mouth dryness and increased salivary flow in patients with xerostomia complicating chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2006 Jul;12(7):792-4.
54. Von der Fehr FR, Löe H, Theilade E. Experimental caries in man. Caries Res. 1970;4(2):131-48.
55. Moynihan P, Petersen PE. Diet, nutrition, and the prevention of dental diseases. Public Health Nutr. 2004 Feb;7(1a):201-26.
56. Castellarin P, Stevenson K, Biasotto M, et al. Extensive dental caries in patients with oral chronic graft-versus-host disease. Biol Blood Marrow Transplantation. 2012 Oct;18(10):1573-79.
57. Weyant RJ, Tracy SL, Anselmo TT, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91.
58. Featherstone JDB, Chaffee BW. The evidence for caries management by risk assessment (CAMBRA®). Adv Dent Res. 2018 Feb;29(1):9-14
59. Slayton RL, Urquhart O, Araujo MWB, et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: a report from the American Dental Association. J Am Dent Assoc. 2018 Oct;149(10):837-49.
60. Contreras V, Toro MJ, Elías-Boneta AR, Encarnación-Burgos A. Effectiveness of silver diamine fluoride in caries prevention and arrest: a systematic literature review. Gen Dent. 2017 May-Jun;65(3):22-9.
61. Bernabé E, Vehkalahti MM, Sheiham A, et al. Sugar-sweetened beverages and dental caries in adults: a 4-year prospective study. J Dent. 2014 Aug;42(8):952-8.
62. Young DA, Lyon L, Azevedo S. The role of dental hygiene in caries management: a new paradigm. J Dent Hyg. 2010 Summer;84(3):121-9.
63. Reed DN, Hall DL, Cottle JH, et al. Dental management of scleroderma patients using pentoxifylline plus vitamin E with and without TheraBite(®) to reduce trismus: two case reports and brief review of literature. Clin Case Rep. 2020 Jan 17;8(2):247-53.
64. Tolle SL. Scleroderma: considerations for dental hygienists. Int J Dent Hyg. 2008 May;6(2):77-83.
65. Poole J, Conte C, Brewer C, et al. Oral hygiene in sclero-derma: the effectiveness of a multi-disciplinary intervention program. Disabil Rehabil. 2010;32(5):379-84.