You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Dentures With Dignity: The Influence of Esthetics, Function, and Patient Psychology on Successful Treatment Outcomes
Cornelia Cone, MA; and Miles Cone, DMD, CDT, FACP
Successful outcomes of complete denture therapy are largely dependent on the mastery of numerous technical procedures, adequate consideration of dynamic functional and biological elements, and a seamless collaboration between the patient, dental practitioner, and dental laboratory to reach consensus regarding dental esthetic preferences. Another important component of treatment that greatly impacts the final outcome of complete denture therapy - yet is often ignored - is the recognition and strategic management of various patient psychological factors.1,2
Despite the relative lack of focus that clini-
cians place on the psychological factors of patients who receive dentures, there exists a well-established relationship between the psychology of the patient, the patient personality, and the dentist-patient interaction.1,3-8Pertinent psychosocial factors that warrant consideration when treating edentulous patients include depression, anxiety, fear, adaptability, social support network, perceived quality of life before treatment, and body image.9-11 However, the psychological components that need to be addressed when managing the oral health care needs of patients treated with dentures often remain obscure, owing to the inherent subjective nature of these psychological factors, and also because of the paucity of formal training that dentists receive on this subject in undergraduate and residency training programs.
An increased awareness of the correlation between demographic variables, medical conditions, and patient psychological factors will help enable clinicians to identify and control the attitudes, expectations, and concerns of individual patients while establishing trust as a standard part of any treatment protocol. The ability to build rapport with patients has been shown to result in higher levels of patient acceptance regarding the skills, knowledge, and professionalism of the dental practitioner, and may also have a powerful influence on overall patient satisfaction.12,13This article aims to present a pragmatic approach to considering both psychology and physiology when treating edentulous patients to increase the frequency and predictability of successful treatment outcomes.
Case Study 1 - Patient With Failing Natural Dentition Treated With Immediate Dentures Followed by a Maxillary Denture / Two-Implant Mandibular Overdenture
A 65-year-old woman presented for a clinical consultation regarding cosmetic and functional concerns with her natural teeth (Figure 1). The patient's medical history was unremarkable; however, her intraoral and radiographic examination revealed poor to fair oral hygiene, generalized periodontal disease (gingival inflammation, bleeding on probing, and horizontal/vertical bone loss), heavily restored dentition, bilateral occlusal plane discrepancies, wide-spread recurrent decay, numerous endodontically treated teeth, and several periapical radiolucencies. The patient further reported that she was suffering from various oral health-related quality of life issues such as missing work as a result of dental-related pain and discomfort, as well as severe anxiety and depression due to esthetic concerns that her smile made her unattractive in social settings.
Oral health status such as that exhibited by this patient is commonplace within the dental profession and poses particular challenges in terms of managing the psychological aspects of treatment. Being confronted with the potential loss of teeth, especially those that are highly visible structures of the oral cavity, often results in severe anxiety and depression,14 as was the experience of this patient.The management of patients requiring highly invasive and extensive prosthodontic care is most successful when it revolves around open lines of communication regarding the needs, values, and preferences of patients regarding treatment. It is critical for the clinician to take any fears and apprehensions into account and to demonstrate proper respect and empathy for the patient's feelings, allowing the patient sufficient time to feel comfortable proceeding with the planned restorations. The relationship that is borne from this interaction is known as a "therapeutic alliance"15,17 and is characterized by empathy, a collaborative approach to care, open communication, and mutual respect. When a "therapeutic alliance" forms the bedrock of clinical treatment, the clinician is able to focus on patient-centered care. In this particular case study, the clinician provided a relaxed initial consultation aimed at making the patient feel comfortable voicing concerns and reservations regarding treatment. This was followed by a secondary treatment plan discussion, and ample time was provided during each scheduled appointment to ensure that the patient felt heard, informed, understood, and comfortable with each procedure. This therapeutic alliance allowed for and encouraged the patient to actively share and engage in the clinical decision-making process regarding her definitive treatment plan. This mode of healthcare partnership in which the patient is given the tools to better understand treatment options and make an informed choice about his or her future care has been shown to be associated with improved physical and psychological outcomes.16,17
Studies indicate that the psychological response to tooth loss closely resembles the five stages of bereavement-ie, denial, anger, depression, bargaining, and acceptance.14Anecdotally, the authors have found that it may typically take approximately 18 to 24 months for patients to adequately accept the need for tooth extractions and restorations. The patient of this case study exhibited outward denial regarding the severity of her current oral status and ultimately delayed treatment for just over 1 year from the date of her initial examination. Upon her return to the dental clinic, the patient noted that she had tried to improve her oral health with more frequent brushing and flossing, had sought out second opinions from other providers, had fractured several more teeth, and had developed an additional abscess in one of her maxillary molars. In the patient's own words, she described her emotional status as "I am sick and tired of being sick and tired," and stated that she was finally ready to accept the recommended treatment plan. In the clinician's experience, successful treatment outcomes are more likely to be achieved when the patient does not feel coerced into treatment, but rather is resolved to proceed with the treatment of their own accord, as was the case with the patient in this case study.
Patient hesitancy regarding dentition replacement may also be attributed to the "sunk-cost effect," wherein patients feel compelled to save their teeth to justify the massive time and financial investment that has already been made over several years.18 Patients commonly find themselves in this position as a result of dentists' inability to recognize the "tipping point" in the lifecycle of teeth that have endured a prolonged and poorly planned prosthetic treatment. In other cases, the dentist may have lacked the resolve to inform the patient of the poor prognosis of the remaining dentition.
Following a consultation and thorough examination together with the oral surgeon, the patient agreed to a treatment plan in which she would be placed under intravenous sedation to have her remaining dentition removed and two mandibular implants simultaneously placed to aid in the retention of a mandibular prosthesis, coupled with same-day delivery of an immediate maxillary and mandibular denture (Figure 2).
Although edentulism does not constitute optimum oral function, the upside is that it can be seen as offering a fresh start-which many patients welcome as an opportunity for a cosmetic overhaul allowing them to select a completely new set of teeth. It is known that the restorative dentist's perception of dental esthetics may differ significantly from that of the patient,19 and it is therefore critical to include the patient in the denture tooth selection aspect of the decision-making process. When given the opportunity, patients will tend to favor teeth that look more natural or possess exaggerated form and anatomy.20 The patient in this case study selected posterior denture teeth possessing a highly convoluted occlusal topo-graphy and anterior teeth with aggressive morphology and line angles (Figure 3). The patient felt confident with this choice, as it ensured a youthful appearance at the final delivery appointment (Figure 4). Patients who are provided with anatomically based posterior teeth and canine guidance in their complete dentures also exhibit higher levels of denture retention and self-perceived satisfaction.21,22A maxillary anterior wax try-in was the patient's first opportunity to review and approve the esthetics of the proposed restoration setup after consultation between the clinician and the laboratory technician (Figure 4). This intermediate step helps to establish psychological comfort, confidence, and trust in the clinical and laboratory team, as the patient is allowed to assess, critique, and make any necessary recommended changes to the final tooth shade and set-up.
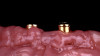
Studies have shown that prior to definitive prosthetic treatment, fully edentulous patients often suffer from compromised levels of various oral health-related quality-of-life factors. These factors, which include functional limitations and psychological discomfort, exhibit statistically significant improvements within a matter of 5 weeks after delivery of their complete dentures.23 To further augment a successful patient outcome, part of the treatment plan for the patient in this case study, following full-mouth extractions and bone grafting procedures, included the placement of Locator® (Zest Dental Solutions) abutments on each mandibular endosseous implant to be used to aid in the retention of the mandibular prosthesis (Figure 5). Consensus research has repeatedly demonstrated that improvements in quality-of-life factors such as denture stability, comfort, and masticatory efficiency are greatly improved with the use of two-implant overdentures compared with traditional dentures.24,25A self-curing resin, CHAIRSIDE® Attachment Processing Material (Zest Dental Solutions), was utilized in the clinic to pick up and incorporate each Locator housing into the final denture and was well tolerated by the patient.
Incorporating two endosseous implants to the alveolar ridge and converting the mandibular prosthesis to an overdenture offers patients an affordable pathway with increased predictability to long-term satisfaction with their dentures and their oral health. The radically improved function and esthetics (Figure 6) that are evident over a relatively short span of time may be quite impactful in solidifying a positive relationship with the clinician and, in the patient of this case study, reduced her anxiety and depression by restoring the functionality of her dentition and her ability to smile again with self-confidence.
Case Study 2 - Patient With Existing Conventional Maxillary / Mandibular Dentures Treated With Conventional Maxillary Denture / Two-Implant Mandibular Overdenture
A 62-year-old man presented with functional complaints about his existing dentures that included occlusal mismatch between the maxillary and mandibular teeth and lack of retention/stability. He expressed clear expectations related to augmenting the functionality of the prosthesis, since he could not adequately masticate food with his existing dentures and noted that he would frequently choose to not wear the prosthesis while eating. The patient had only one minor cosmetic desire, namely, a slightly brighter shade for his teeth, which he also noted was not a very important concern (Figure 7). The patient's prioritization to improve mastication compared to esthetic enhancement of his complete denture is consistent with the findings in the literature that men tend to object more than women to ill-functioning oral prosthetics.3
The patient was diagnosed with a brain tumor approximately 1 year before his initial consultation, and his remaining teeth had been extracted just before his oncologic surgery and radiation therapy. The patient was well-accustomed to the idea of tooth loss at the time of his initial visit and did not show any overt signs of depression or anxiety associated with his edentulism. In this particular case, it was vital to note that even though the patient did not fall into a geriatric demographic, his neurological medical history proved to constrain the channels of dentist-patient communication, similar to that which has been found to occur with patients of advanced age.26 Many of the patient's particular psychological challenges stemmed from a decline in sensory processes (ability to see, hear, touch, and taste). The clinician provided him with extended appointments to allow him more time to understand treatment options and information, and delivered oral healthcare guidelines and treatment information gently and at a pace that helped ensure understanding and trust. To help support the patient throughout treatment, the clinician requested that the patient's spouse attend each office visit, and provided detailed written instructions that outlined each step of each procedure; in addition, after-hours appointments were made available to the patient.
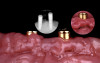
The treatment plan for the patient included a complete remake of his existing maxillary and mandibular dentures to include higher-value denture teeth and the addition of two implants to address the lack of retention caused by his resorbed alveolar bone in the mandible. During implant planning with a clear surgical guide, it was noted that the atrophied mandibular bone might necessitate a compromised implant position, requiring a facially oriented placement of the attachment housings within the mandibular denture (Figure 8, left panels). It has been shown that acrylic alone is often an unreliable material to mask the appearance of metal substructures27 and the use of metallic-colored housings in such positions may have a negative esthetic impact on the prosthesis. Research has shown that pink anodized titanium implant components offer an effective means to achieve excellent esthetics in situations where discoloration may occur28 (Figure 8, right panel). For this reason, the decision was made to utilize a Locator housing with a pink anodized finish to aid in the concealment of the incorporated attachment hardware (Figure 9). Each step of this process, including anatomical limitations, prosthetic treatment planning, and the denture fabrication techniques, were discussed in detail with the patient to facilitate a supportive dentist-patient relationship.
After a 3-month postimplant placement healing phase, final impressions for the maxillary and mandibular arch were performed using a simplified technique with Massad™ Edentulous Low Temp Impression Trays (Zest Dental Solutions) and irreversible hydrocolloid (Figure 10). Many of the historical guidelines and principles described in the construction of complete dentures, including the use of a face-bow transfer,29 occlusal schemes,10 and impression tray plus material,30 have been shown to lack efficiency and be less cost-effective, and are not well supported by the literature.31 Applying a simplified technique also helped to assuage the patient's stress and anxiety levels by reducing the chair time for this appointment from an average of 90 minutes to less than 30 minutes.
The master casts produced from the alginate impressions were utilized to fabricate record bases and wax rims for each arch. At the subsequent appointment, esthetic landmarks including facial/maxillary midline, maximum smile line, and approximate position of the canine teeth were recorded on the wax rims to serve as guidelines for the laboratory technician to set the anterior teeth (Figure 11). The wax rims further serve to aid the clinician in determining the occlusal vertical dimension, and as a means of capturing the centric jaw relation (CJR) record. Incorporating Locator housing attachments into the mandibular record base serves to make the CJR recording provide a more accurate reading; however, this is often not possible for the maxillary arch since implants are utilized less frequently and a removable prosthesis is more often retained with adhesion and atmospheric pressure.32 Using a few beads of dry mouth gel on the intaglio of the maxillary record base serves as an off-label denture adhesive and is an excellent alternative for the maxillary arch. During this phase of treatment, it is useful to view the wax rims within the oral cavity at rest and during speech. The author has found that asking the patient to discuss their family, pets, or favorite hobbies is not only a superb way to evaluate the dynamic lip position, maximum smile line, facial esthetics, and phonetics, but
also an excellent clinical approach to building positive rapport with the patient.
At the final delivery appointment, a vinyl polysiloxane (VPS) interocclusal bite registration jig was made to help in the intercuspation of the maxillary and mandibular teeth during the seating of the Locator housing attachments. Vent holes were placed through the lingual surface of each housing recess in the mandibular denture to ensure that hydraulic pressure from the CHAIRSIDE resin did not interfere with the seating and ultimate pick-up of each housing attachment (Figure 12).
The incidence in the number of edentulous patients worldwide is increasing, which is in large part due to an increase in the life-expectancy rates.33 Several studies have shown that between 20% and 30% of these edentulous patients experience difficulty adapting to their new dentures.34,35It is well-known that patients who receive more adequate dentist-patient communication and better-quality dentures will demonstrate higher levels of satisfaction.36 In addition to providing a well-designed prosthesis that possessed appropriate esthetic and phonetic attributes, the culmination of carefully executed treatment planning, collaboration with the dental laboratory, and communication with the patient of this case study were evident in the successful final outcome at the delivery appointment (Figure 13). The patient expressed deep appreciation and gratitude regarding the improvements in the function and esthetics of his denture. As a final gesture to improve post-treatment satisfaction and compliance, and to alleviate any potential apprehensions with his new prosthetics, verbal and printed instructions were provided that covered nutrition/diet, home-based hygiene/follow-up office visits, and tips and tricks to enhance and improve speech patterns.
Case Study 3 - Patient With Existing Conventional Maxillary Denture / Two-Implant Mandibular Overdenture Treated With Conventional Maxillary Denture / Two-Implant Mandibular Overdenture
A 40-year-old woman with an existing maxillary denture opposing a mandibular two-implant overdenture presented with cosmetic concerns regarding the "plastic" and homogenous look of her denture teeth, as well as a shift in the midline of the maxillary and mandibular dentures (Figure 14); she also experienced reduced ability to chew due to the poor alignment and occlusion of her prosthetics, which she noted was causing daily discomfort.
During the initial examination, the dentist-patient relationship was fueled through the use of open-ended questions, requesting that the patient describe her expectations for treatment, and discussing the patient's current situation using clear and concise language. When asked to detail her dental history, the patient noted that she had lost all of her teeth approximately 8 years ago, and stressed that to protect her career and because of her young age, she required discretion surrounding her treatment; she revealed that her close friends and immediate family were unaware that she was edentulous. The patient's expectations to have her oral health status remain a secret from her spouse was discussed at length. However, because the patient wanted a more natural esthetic, the clinician did explain to her that the same-day results of full-mouth transformation would likely be readily discernable to most individuals, particularly her husband. The patient indicated that she understood all the ramifications of replacing her existing prostheses and accepted the potential social consequences and attention that a new smile might attract.
As a result of her insecurities about her edentulism, the patient reported that she routinely slept with her dentures on through the night. The constant contact of the alveolar mucosa with the intaglio surface of an ill-fitting mandibular prosthesis had resulted in inflamed, hyperplastic soft tissue and in a soft-tissue lesion around the left Locator abutment (Figure 15).
The treatment plan for this patient included a remake of the maxillary denture/mandibular two-implant overdenture, surgical removal of the excess hyperplastic tissue, repair of the soft-tissue defect, and replacement of the existing Locator with shorter abutments. The emergence angle of each mandibular implant as well as their height needed to be taken into consideration when designing the overdenture to help achieve a more uniform path of insertion and removal. The decision was made by the clinician and laboratory to capture the precise position and trajectory of each mandibular implant in the final impression. This was achieved with the use of Locator closed-tray impression copings (Figure 16), which were picked-up in the VPS final impressions (Figure 17). Silicone final impressions were also critical for this particular case, since the impressions would be mailed to the laboratory for pouring the master casts.
When considering dental esthetics with regard to gender and age, clinicians should note that younger women have been shown to exhibit more maxillary incisal display while smiling than all other demographic groups.37Further research on the smile dynamics of these patients has indicated two easily reproducible postures of the upper and lower lips that should be evaluated during prosthetic treatment: the position of the lips at rest (repose), and the position of the lips with a Duchenne smile (maximum smile).38
For this patient, during the try-in of the record bases and wax rims, it was critical to document the lips in repose and during the maximum smile to ensure the development of a tooth display most appropriate for a 40-year-old woman (Figure 18). The laboratory transferred this information to the wax trial denture (Figure 19) and used this phase of treatment to address the patient's chief complaint about the esthetics of her existing dentures - specifically, the monochromatic appearance of the teeth and gingiva, as well as a lack of texture and translucency in the teeth (Figure 20).
The necessary foundation to a natural-looking and attractive outward appearance of dentition is good oral health. Therefore, in this patient the final maxillary denture/mandibular two-implant overdenture was fabricated with properly extended borders, an intimately fitting intaglio surface, and a highly polished cameo surface to resist adhesion of bacteria and development of biofilm (Figure 21).
It is not uncommon for the experienced denture wearer, such as this patient, to require approximately 2 to 4 weeks of continual use of their new prosthetics to re-establish oral muscular coordination and speech competence.39 Similar to previous cases, the authors provided a list of suggested activities for the patient to help hasten the accommodation process and reduce concerns that others would notice the new dentures. This list includes reading or singing out loud, actively socializing, engaging in progressive eating patterns (soft diet followed by firmer/chewier foods over time), discouraging the use of pre-existing dentures, and providing improved oral hygiene habits/home-
care guidelines for patients.
The aggregate efforts of the clinician's technical skill, collaborative communication with the patient, and prosthesis fabrication by the dental laboratory produced predictable and exceptional results for this patient. Taking into consideration the patient's refusal to remove her dentures before going to sleep at night, the establishment of an appropriate occlusal scheme allowed the patient to function efficiently, without discomfort, and will certainly have a positive impact on the health of the underlying oral structures. The patient noted that even though she does not intend to reveal her oral health situation to family or friends, she nevertheless felt an immediate enrichment in overall self-
esteem. The patient related her newly established confidence to the improvements in dentition functionality and the enhanced denture esthetic, indicating that her new teeth possessed a more youthful and authentic appearance. She also reported that she greatly appreciated the correction of the maxillary and mandibular midline, which were now coincident (Figure 22).
Conclusion
Knowledge of the patient psychological factors that are involved in complete denture therapy is critical to successful treatment outcomes. In particular, clinicians need to have an understanding of the psychological and emotional status of the patient who has experienced complete tooth loss and now requires a full-mouth rehabilitation. Considering that denture therapy often requires protracted treatment timelines, it is not uncommon for this extended care to lead to frustration, erode clinical profit margins, and damage the dentist's confidence and reputation. The need to avoid these pitfalls of treatment elevates the importance of managing both the psychological and physiologic aspects of complete denture treatment when planning denture fabrication. Numerous studies have shown that patient satisfaction with their dentures is heavily influenced by both the patient's experience and psychological state, and satisfaction levels are frequently unrelated to the technical skill of the clinician or the quality of the prosthesis.40,41 Having a sound understanding of patients' physical, psychological, and emotional responses to complete denture therapy enables the clinician to efficiently formulate treatment planning and manage patient expectations in advance-giving the dental practitioner a distinct advantage in achieving treatment success.
References
1. John MT, Micheelis W, Steele JG. Depression as a risk factor for denture dissatisfaction. J Dent Res. 2007;86(9):852-856.
2. Bandodkar KA, Aras M. Psychological considerations for complete denture patients. J Indian Prosthodont Soc. 2007;7(2):71-76.
3. Langer A, Michman J, Seifert I. Factors influencing satisfaction with complete dentures in geriatric patients. J Prosthet Dent. 1961;11(6):1019-1031.
4. Lefer L, Pleasure MA, Rosenthal L. A psychiatric approach to the denture patient. J Psychosom Res. 1962;6(3):199-207.
5. al Quran F, Clifford T, Cooper C, Lamey PJ. Influence of psychological factors on the acceptance of complete dentures. Gerodontology. 2001;18(1):35-40.
6. Patil MS, Patil SB. Geriatric patient-psychological and emotional considerations during dental treatment. Gerodontology. 2009;26(1):72-77.
7. Ozdemir AK, Ozdemir HD, Polat NT, Turgut M, Sezer H. The effect of personality type on denture satisfaction. Int J Prosthodont.2006;19(4):364-370.
8. Sheiham A, Steele JG, Marcenes W, Finch S, Walls AW. The impact of oral health on stated ability to eat certain foods; findings from the national diet and nutrition survey of older people in Great Britain. Gerodontology. 1999;16(1):11-20.
9. Chamberlain BB, Chamberlain KR. Depression: a psychologic consideration in complete denture prosthodontics. J Prosthet Dent. 1985;53(5):673-675.
10. Klineberg I, Kingston D, Murray G. The bases for using a particular occlusal design in tooth and implant-borne reconstructions and complete dentures. Clin Oral Implants Res. 2007;18(Suppl 3):151-167.
11. Friedman N, Landesman HM, Wexler M. The influences of fear, anxiety, and depression on the patient's adaptive responses to complete dentures. Part II. J Prosthet Dent. 1988;59(1):45-48.
12. Hirsch B, Levin B, Tiber N. Effects of dentist authoritarianism on patient evaluation of dentures. J Prosthet Dent. 1973;30(5):745-748.
13. Evans DL, Charney DS. Mood disorders and medical illness: a major public health problem. Biol Psychiatry. 2003;54(3):177-180.
14. Fiske J, Davis DM, Frances C, Gelbier S. The emotional effects of tooth loss in edentulous people. Br Dent J. 1998;184(2):90-93.
15. Goldstein GR. Do we need House in the house? Int J Prosth. 2013;26(2):104-105.
16. Scrambler S, Delgado M, Asimakopoulou K. Defining patient-centered care in dentistry? A systematic review of the dental literature. Br Dent J. 2016;221(8):477-484.
17. Babatunde F, MacDermid J, MacIntyre N. Characteristics of therapeutic alliance in musculoskeletal physiotherapy and occupational therapy practice: a scoping review of the literature. BMC Health Serv Res. 2017;17(1):375.
18. Arkes HR, Blumer C. The psychology of sunk cost. Organ Behav Hum Decis Process. 1985;35(1):124-140.
19. Kokich VO Jr, Kiyak HA, Shapiro PA. Comparing the perception of dentists and lay people to altered dental esthetics. J Esthet Dent. 1999;11(6):311-324.
20. Waliszewski M, Shor A, Brudvik J, Raigrodski AJ. A survey of edentulous patient preferences among different denture esthetic concepts. J Esthet Restor Dent. 2006;18(6):352-369.
21. Sutton AF, Worthington HV, McCord JF. RCT comparing posterior occlusal forms for complete dentures. J Dent Res. 2007;86(7):651-655.
22. Peroz I, Leuenberg A, Haustein I, Lange, K-P. Comparison between balanced occlusion and canine guidance in complete denture wearers--a clinical, randomized trial. Quintessence Int. 2003;34(8):607-612.
23. Shrestha B, Basnet BB, Adhikari G. A questionnaire study on the impact on the oral-health related quality of life by conventional rehabilitation of edentulous patient. Br Dent J Open. 2020;6(3):1-5.
24. Feine JS, Carlsson GE, Awad MA, et al. The McGill Consensus Statement on Overdentures. Montreal, Quebec, Canada. May 24-25, 2002. Int J Prosthodont. 2002;15(4):413-414.
25. Thomason JM, Feine J, Exley C, et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients. The York Consensus Statement. Br Dent J.2009;207(4):185-186.
26. Mysore, AR, Aras MA. Understanding the psychology of geriatric edentulous patients. Gerodontology. 2012;29(2):e23-27.
27. White KC, Moore DJ. A method for simulating gingival color on aluminum alloy denture base. J Prosth Dent. 1986;55(5):650-652.
28. Wang T, Wang L, Lu Q, Fan Z. Changes in the esthetic, physical, and biological properties of a titanium alloy abutment treated by anodic oxidation. J Prosth Dent. 2019;121(1):156-165.
29. Walker F, Ayoub AF, Moos KF, Barbenel J. Face bow and articulator for planning orthognathic surgery: 1 face bow. Br J Oral Maxillofac Surg. 2008;46(7):567-572.
30. Kawai Y, Murakami H, Shariati B, et al. Do traditional techniques produce better conventional complete dentures than simplified techniques? J Dent. 2005;33(8):659-668.
31. Carlsson GE. Some dogmas related to prosthodontics, temporomandibular disorders and occlusion. Acta Odontol Scand. 2010;68(6):313-322.
32. Guédat C, Nagy U, Schimmel M, Müller F, Srinivasan M. Clinical performance of LOCATOR® attachments: A retrospective study with 1-8 years of follow-up. Clin Exp Dent Res. 2018;4(4):132-145.
33. Thomason JM, Lund JP, Chehade A, Feine JS. Patient satisfaction with mandibular implant overdentures and conventional dentures 6 months after delivery. J Prosthodont. 2003;16(5):467-473.
34. Wong MC, McMillan AS. Tooth loss, denture wearing and oral health-related quality of life in elderly Chinese people. Community Dent Health. 2005;22(3):156-161.
35. Divaris K, Ntounis A, Marinis, A, Polyzois G, Polychronopoulou A. Patients' profiles and perceptions of complete dentures in a university dental clinic. Int J Prosthodont. 2012;25(2):145-147.
36. Chen JH, Huang HL, Lin YC, Chou T-M, Ebinger J, Lee HE. Dentist-patient communication and denture quality associated with complete denture satisfaction among Taiwanese elderly wearers. Int J Prosthodont. 2015;28(5):531-537.
37. Ahmad, I. Anterior dental aesthetics: dentofacial perspective. Br Dent J. 2005;199(2):81-88.
38. Peck S, Peck L, Kataja M. Some vertical lineaments
of lip position. Am J Orthod Dentofacial Orthop.1992; 101(6):519-524.
39. Klineberg I, Murray G. Osseoperception: sensory function and proprioception. Adv Dent Res. 1999;13(1):120-129.
40. Heydecke G, Klemetti E, Awad MA, Lund JP, Feine JS. Relationship between prosthodontic evaluation and patient ratings of mandibular conventional and implant prostheses. Int J Prosthodont. 2003;16(3):307-312.
41. Mersel A, Peretz B. A behavioural approach in the treatment of elderly patients: a new philosophy. Int Dent J. 2003;53(1):51-56.