You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Prolonged muscle strain and repetitive movements in the dental workforce may lead to work-related musculoskeletal disorders (WMSDs).1 The prevalence of WMSDs affects the majority of dental professionals. De Sio et al. reported that 54-93% of dental professionals suffer from work related pain2 whereas Hayes et al. found that approximately 68% of dental clinicians experienced pain in the neck, lower back, and shoulders.3 Over time, the gradual severity of WMSDs may lead to increased physical limitations and the eventual inability to work.
Dentists and dental hygienists often adopt asymmetric and compromised postures, such as having the head flexed forward or the shoulders slumped forward or elevated above line of the trunk.4 Over time, muscles and joints become strained - triggering symptoms such as backache, headache, neck and shoulder pain.5 By improving and maintaining neutral postures, dental hygienists can reduce the risks of developing WMSDs through ergonomics.6,7 Ergonomics is defined by the scientific discipline of modifying techniques, designing equipment, and transforming working spaces to maximize the clinician's safety and efficiency and minimize operator pain and fatigue. Possessing the theory of ergonomics, however, is insufficient to prevent WMSDs. Despite having knowledge of ergonomics concepts, Cervera-Espert et al. found that only 28.6% of dental clinicians demonstrated acceptable and uncompromised postures.8This disparity between the theory and the application of ergonomic concepts can be mitigated with postural modifications discovered through self-awareness and self-assessment.
Self-assessment is an accurate evaluation of oneself based on specific criteria.9-11 Bowers and Wilson stated that self-assessment had positive effects on dental hygiene education and clinical practice.12 Ergonomics training using self-assessment and photography has been shown to improve the postures and the accuracy of ergonomic self-assessments among dental hygiene students.5 However, it is not known whether this type of ergonomics training, involving self-assessments and photography, would be effective with practicing clinicians. The purpose of this study was to determine whether feedback involving photography and self-assessment would improve the postures and the accuracy of ergonomic self-assessments among practicing dentists and dental hygienists.
Methods
This study received approval from The Ohio State University Institutional Review Board (2018H0157). A randomized controlled design was used with two parallel groups. A convenience sample of dentists and dental hygienists, employed at The Ohio State University Dental Faculty Practice, was recruited by the principal investigator (PI) (n=50). The following inclusion criteria were used for the participants: an active Ohio dentist (DDS) or Registered Dental Hygienist (RDH) license; currently involved in at least 8 hours of clinical practice per week; available to commit to the time requirements of the study. Following the provision of the study details and a question-and-answer session, participants signed an informed consent document prior. As determined with G-power (Dusseldorf, Germany), a sample of 50 participants would yield a power of 0.80, which would determine whether the intervention had a true effect on the population. The PI used the randomization feature in SPSS Version 26 (IBM, Armonk, NY, USA) to generate a random list of random numbers to assign participants to the control and experimental (training) groups. The PI kept all research personnel blinded to the random assignment.
Instruments
The Modified-Dental Operator Posture Assessment Instru-ment (M-DOPAI) was used for the participants' ergonomic self-assessments and the raters' ergonomic evaluations.13,14 The M-DOPAI combined Branson et al. Posture Assessment Instrument, which was tested for validity and reliability for of ten of the twelve criteria,15 and Maillet et al.16 Posture Assessment Criteria.16 Each criterium had one of three categories: acceptable (one point), compromised (two points), or harmful (three points). The ergonomic scores ranged from a total of 12 points (most acceptable posture) to 32 points (most harmful postures).
Digital photographic images were captured using a 10.5-inch iPad Pro (Apple, Cupertino, CA, USA). The flash and sound options were disabled to minimize any disruptions to the participants. The size of the screen allowed the PI to readily review the photographs with the participants and/or patients. All images were stored in the secure Buckeye Box, which was only accessible to the PI and key personnel.
A survey instrument was used to evaluate for changes in attitudes about musculoskeletal disorders and ergonomics. The pre- and post-test surveys had two items, with 5-point Likert-scale attributes ranging from 1-strongly agree to 5-strongly disagree. The questions were modeled after existing attitudinal survey questions.13,14 The post-test survey included one open-ended question for general comments about the study. The survey was administered through Qualtrics (Provo, Utah, USA). Survey invitations were sent at week one and after the conclusion of the study at week four.
Procedures
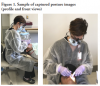
Data collection occurred through a four-week period. At week one, all participants were photographed twice (front and profile) and completed an ergonomic self-assessment (M-DOPAI) without viewing the photographs or receiving feedback (Figure 1). Prior to completing the self-assessment, the same general instructions were given to each participant. During weeks two and three, participants in the control group independently completed an ergonomic self-assessment
(M-DOPAI) without any additional photographs or feedback from the PI. Participants in the experimental training group had two additional photographs taken (front and profile) and completed an ergonomic self-assessment (M-DOPAI) with the PI. The PI had conducted multiple research studies involving the evaluation of postures, facilitating self-assessment of postures, and the calibration training of raters in the evaluation of postures. The PI facilitated the self-assessments by allowing each participant to self-assess their postures using each of the 12 criteria of the M-DOPAI. The PI would either agree or disagree with the participants' self-assessment and would discuss how to remedy any postural deficiencies. At week four, all participants were photographed twice (front and profile) and independently completed an ergonomic self-assessment (M-DOPAI) without viewing the photographs or receiving feedback.
After the four weeks of data collection, the photographs from week one and week four were evaluated for ergonomic scores. The raters consisted of two faculty members and two dental hygiene students enrolled in the The Ohio State University Dental Hygiene Program. All raters received a 30-minute calibration training from the PI, which consisted of a discussion of ergonomic principles, how to recognize harmful postures, and practicing ergonomic evaluations using sample photographs. Each rater evaluated the week one and week four photographs independently. The PI determined consensus with the scores. Interrater reliability was measured at a Cronbach's alpha level of 0.797 and intraclass correlation of 0.789, 95% CI [.697-.861].
Data analysis
The data were analyzed using SPSS version 26 (IBM, Armonk, NY, USA). A mixed-design ANOVA was used to evaluate improvements in ergonomic scores from week one to week four and a mixed-design ANOVA of Kappa values was used to evaluate improvements in the accuracy of ergonomic self-assessments. The accuracy of ergonomic self-assessments was calculated using Cohen's Kappa coefficient, which ranged from less than 0 (no agreement) to 1 (prefect agreement). Kappa values fell into the following ranges: 0.00 to 0.20 (slight), 0.21 to 0.40 (fair), 0.41 to 0.60 (moderate) and 0.61 to 0.80, and 0.81 to 1.0 (perfect).17 A, mixed-design ANOVA was used to evaluate differences in attitudes regarding ergonomics among the participants. The open-ended responses were categorized by the benefits and challenges of the intervention.
Results
Fifty-two licensed dentists and registered dental hygienists were recruited to participate in the study; two individuals were unable to participate. With this convenience sample (n=50), 25 participants were randomly assigned to either the control or to the experimental training group. Independent sample t-tests revealed no significant differences between the two groups based on gender, age in years (M=48.73, SD=13.82), hours in clinical practice (M=18.22, SD=13.85), and years in clinical practice (M=24.13, SD=14.94) (p>.05).
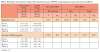
The first aim was to determine whether ergonomics training utilizing photography would improve ergonomic scores among practicing dentists and dental hygienists. A 2x2 mixed-design ANOVA was used to evaluate the effects of group (control and training group) and time (pre-test and post-test) on ergonomic scores. Significant interactions were found with time x group (F(1,3)=6.043, p=.015). Significant main effects were found with time (F(1,3)=18.209, p<.001) and group (F(1,3)= 4.356, p=.038. Post hoc one-way ANOVA revealed no significant differences in pre-test ergonomic scores of the training group (M=17.14, SD=3.270, 95% CI [16.21-18.07]) compared to the control group (M=16.98, SD=3.583, 95% CI [15.96-18.00], F(1,98)=.054, p>.05) but significant improvements in post-test ergonomic scores of the training group (M=14.24, SD=1.779, 95% CI [13.73-14.75]) compared to the control group (M=16.20, SD=3.239, 95% CI [15.28-17.12], F(1,98)=14.066, p<.001). The training intervention resulted in a significant improvement on ergonomic scores (Table I).
The second aim was to determine whether ergonomics training utilizing photography would improve ergonomic scores among practicing dentists and dental hygienists. A 2x2 mixed-design ANOVA was used to evaluate the effects of group (control and training group) and time (pre-test and post-test) on the accuracy of ergonomic self-assessments. A significant interaction was found with time x group (F(1,3)=2.769, p=.041) and a significant main effect was found with group (F(1,3)=6.583, p=.012). Post hoc one-way ANOVA revealed no significant differences in pre-test accuracy of ergonomic self-assessments of the training group (M=.127, SD=.193, 95% CI [.047-.207]) compared to the control group (M=.088, SD=.127, 95% CI [.036-.140], F(1,48)=.715, p>.05) but significant improvements in post-test accuracy of ergonomic self-assessments of the training group (M=.278, SD=.338, 05% CI [.139-.418]) compared to the control group (M=.095, SD=141, 95% CI [.037-.153], F(1,48)=6.251, p=.016). The training intervention resulted in a significant improvement on the accuracy of ergonomic self-assessments (Table I).
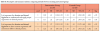
The third aim was to evaluate for changes in attitudes about musculoskeletal disorders and ergonomics among practicing dentists and dental hygienists. A 2x2 mixed-design ANOVA was conducted to determine any differences in attitudes from week one to week four. No significant differences were found in attitudes between the control and training groups (p>.05) (Table II). All participants either agreed or strongly agreed that it was important for both dentists and dental hygienist to understand proper ergonomics, apply proper ergonomics, and have accurate ergonomic self-assessment skills while in clinical practice. From the open-ended questions in the post-study survey, the respondents reported benefits from the "increased awareness of their postures" from their participation in the study and the challenges of "self-assessing without a mirror" and not achieving "ideal postures depending on the patient."
Discussion
The purpose of this study was to determine whether feedback involving photography and self-assessment would improve the postures of practicing dentists and dental hygienists. The ergonomics training utilizing photography resulted in improvements in ergonomic scores and the accuracy of ergonomic self-assessments among the dentists and dental hygienists. Although the participants understood the importance of proper ergonomics, much potential remains for improvements in the postures of dentists and dental hygienists engaged in clinical practice.
Dentistry is a physically demanding occupation in which the failure to maintain balanced and neutral postures may result in the development of work-related musculoskeletal disorders (WMSDs).1,7Anecdotally, based on the rater evaluations, the most recurring compromised area of the body during the evaluations was the forward flexion of the head. Pain associated with the neck area has been identified as one of the most common sources of pain for dental hygienists.1-4 Many times, dental clinicians fail to recognize the importance of ergonomic postures until after the initiation of pain.18 This finding emphasizes the importance of maintaining neutral, balanced postures while practicing dentistry and dental hygiene.
Although magnification loupes are perceived as preventative measures, they may also be the source of musculoskeletal problems with compromised or harmful positions of the head, such as the observed forward flexion of the head identified in this study. In theory, either through-the-lens (TTL) or flip-up magnification loupes, when properly selected and adjusted, can support balanced musculoskeletal ergonomic and provide working distances to keep the body upright and enhance clinical performance.9,10 However, 82% of surveyed dental professionals were found to have been practicing with coaxial misalignment of their magnification loupes, which do not support the optimal visual acuity or neutral postures.19 In addition, if the angle of declination of through-the-lens (TTL) magnification loupes is limited to 30 degrees, the natural tendency of the clinician is the forward flexion of the head. The neck, shoulders, and upper back have been reported as the most common sources of pain for dental hygienists.20Future research is needed to determine whether the angle of declination of TTL magnification loupes can be increased to angles greater than 30 degrees or whether flip-up magnification loupes may provide increased angles of declination to prevent the forward flexion of the head.
In this study, the accuracy of ergonomic self-assessments of the practicing dentists and dental hygienists was initially in the slight agreement range for all participants and increased to the moderate agreement range for the training group. In a previous study of dental and dental hygiene students undergoing a similar intervention, the accuracy of ergonomic self-assessments increased from slight to fair agreement.13,14 The main difference was that the dental and dental hygiene students overestimated the correctness of their postures whereas the practicing dentists and dental hygienists underestimated the correctness of their postures. Since dental and dental hygiene students are still learning the technical aspects of the dental hygiene profession, less attention may be placed on maintaining neutral postures. For experienced dental clinicians, more attention can be devoted to making postural improvements since less focus is devoted to learning the basic clinical aspects of the profession.
Although ergonomic interventions may consist of cognitive, physical, and organizational interventions, most studies, including the present study, have only tested the effects of physical interventions.21 The main limitation of cognitive and organizational interventions is the lack of translation into postural changes with the individual clinician.22 Dental students failed to demonstrate neutral working postures after receiving cognitive instruction on ergonomics.23However, no ergonomic intervention has been shown to overcome a clinical environment that inhibits neutral and ergonomic postures.5 Compromised postures arising from challenging work environments, may start to become habitual and difficult to modify over time.8
Limitations were identified in this study. The small sample size and the use of single research site limits the generalizability of the results. Future studies should be completed using larger sample sizes and dentists and dental hygienists practicing at different institutions and settings. The use of still-imaged versus video-imaged postures may have introduced bias when the postures were captured. Although the Hawthorne effect may have contributed to the overall improvements in postures, the training intervention led to greater improvements in postures with dentists and dental hygienists as compared to the control group. Future studies should explore longer-term effects of ergonomics training utilizing self-assessment, photography and feedback. Clinicians' confidence in performing ergonomic self-assessments and the benefits of booster ergonomics training sessions should also be explored.
Conclusion
Ergonomics training utilizing photography and feedback resulted in improvements in both ergonomic scores and the accuracy of ergonomic self-assessments among practicing dentists and dental hygienists. All participants strongly agreed that it was important for practicing clinicians to understand and apply proper ergonomics in addition to accurate ergonomic self-assessment skills. Improving ergonomic self-awareness through self-assessment, can help decrease the risks of developing WMSDs among practicing dentists and dental hygienists.
Brian B. Partido, RDH, MSDH is the Executive Director, Dental Programs, Seattle Central College, Seattle, WA, USA, and former faculty member at The Ohio State University; Rebecca Henderson, RDH, MS is an assistant professor, Division of Dental Hygiene, College of Dentistry, The Ohio State University, Columbus, OH, USA.
Corresponding author: Brian B. Partido, RDH, MSDH; brian.partido@seattlecolleges.edu
References
1. Anghel M, Argesanu V, Talpos-Niculescu C, et al. Musculoskeletal disorders (MSDs) consequence of pro-longed static posture. J Exp Med Surg Res. 2007;4:167-72.
2. De Sio S, Traversini V, Rinaldo F, et al. Ergonomic risk and preventive measures of musculoskeletal disorders in the dentistry environment: an umbrella review. PeerJ. 2018;6:e4154.
3. Hayes M, Taylor J, Smith D. Introducing loupes to clinical practice: dental hygienists experiences and opinions. Int J Dent Hyg. 2015 Feb:1-5.
4. Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009 Aug;7(3):159-65.
5. Alyahya F, Algarzaie K, Alsubeh Y, et al. Awareness of ergonomics and work-related musculoskeletal disorders among dental professionals and students in Riyadh, Saudi Arabia. J Phys Ther Sci. 2018 Jun;30(6):770-6.
6. Kagan J. Chap 24 Ergonomics. In: Henry RK, Goldie MP, editors. Dental hygiene application to clinical practice. Philadelphia, PA: F. A. Davis Company; 2016. p. 394-407.
7. Nield-Gehrig J. Chap 1 Principles of positioning. In: Nield-Gehrig J, editor. Fundamentals of periodontal instrumentation and advanced root instrumentation. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2017. p. 9-48.
8. Cervera-Espert J, Pascual-Moscardo A, Camps-Alemany I. Wrong postural hygiene and ergonomics in dental students of the University of Valencia (Spain) (part I). Eur J Dent Educ. 2018 Feb;22(1):e48-e56.
9. Gordon MJ. Self-assessment programs and their implications for health professions training. Acad Med. 1992 Oct;67(10):672-9.
10. Mays KA, Branch-Mays GL. A systematic review of the use of self-assessment in preclinical and clinical dental education. J Dent Educ. 2016 Aug;80(8):902-13.
11. Mould MR, Bray KK, Gadbury-Amyot CC. Student self-assessment in dental hygiene education: a cornerstone of critical thinking and problem-solving. J Dent Educ. 2011 Aug;75(8):1061-72.
12. Bowers JA, Wilson JE. Graduates' perceptions of self-assessment training in clinical dental hygiene education. J Dent Educ. 2002 Oct;66(10):1146-53.
13. Partido BB. Dental hygiene students' self-assessment of ergonomics utilizing photography. J Dent Educ. 2017 Oct;81(10):1194-202.
14. Partido BB, Wright BM. Self-assessment of ergonomics amongst dental students utilising photography: RCT. Eur J Dent Educ. 2018 Nov;22(4):223-33.
15. Branson BG, Williams KB, Bray KK, et al. Validity and reliability of a dental operator posture assessment instrument (PAI). J Dent Hyg. 2002 Fall;76(4):255-61.
16. Maillet JP, Millar AM, Burke JM, et al. Effect of magnification loupes on dental hygiene student posture. J Dent Educ. 2008 Jan;72(1):33-44.
17. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012 Oct;22(3):276-82.
18. Garcia PP, Presoto CD, Campos JA. Perception of risk of musculoskeletal disorders among Brazilian dental students. J Dent Educ. 2013 Nov;77(11):1543-8.
19. Wen WM, Kanji Z, Laronde D, et al. Out of the loupe: the prevalence of coaxial misalignment of surgical loupes among dental professionals. J Am Dent Assoc. 2019 Jan;150(1):49-57.
20. Humann P, Rowe DJ. Relationship of musculoskeletal disorder pain to patterns of clinical care in California dental hygienists. J Dent Hyg. 2015 Oct;89(5):305-12.
21. Mulimani P, Hoe VC, Hayes MJ, et al. Ergonomic interventions for preventing musculoskeletal disorders in dental care practitioners. Cochrane Database Syst Rev. 2018 Oct;10:CD011261.
22. Droeze EH, Jonsson H. Evaluation of ergonomic interventions to reduce musculoskeletal disorders of dentists in the Netherlands. Work. 2005 Sep;25(3):211-20.
23. Garbin AJ, Garbin CA, Diniz DG, et al. Dental students' knowledge of ergonomic postural requirements and their application during clinical care. Eur J Dent Educ. 2011 Feb;15(1):31-5.