You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The ADAA has an obligation to disseminate knowledge in the field of dentistry. Sponsorship of a continuing education program by the ADAA does not necessarily imply endorsement of a particular philosophy, product, or technique.
Xerostomia (dry mouth) is the subjective feeling of oral dryness. It is important to recognize that xerostomia is not a diagnosis, but a symptom with multiple possible causes. Although dry mouth is most frequently associated with altered salivary gland function, there are other etiologies for this oral issue. It is important to perform a complete evaluation of the patient with dry mouth, determining, if possible, the cause of the xerostomia so that appropriate management can be instituted in a timely manner. As the population continues to age with the aids of health advancements and medications, this issue will continue to be a problem in dentistry. The patient with xerostomia who has salivary gland hypofunction is at risk for many oral complications and it is critical to institute appropriate preventive measures. Xerostomia may also be a consequence of systemic disease, and early recognition may aid in treatment. This course will review methods of evaluation for xerostomia and practical measures for management of the patient with dry mouth.
Epidemiology and Etiology of Xerostomia
Xerostomia is a common oral concern for many patients. It is estimated that salivary gland hyposalivation, which causes xerostomia, affects between 1/5 to 1/3 of the adult population.39 Xerostomia is more frequent in the older population due to the synergistic effects of taking several medications.41 More women than men are affected by xerostomia.39 The percentage of occurrence increases in institutionalized elders. However, it should be recognized that xerostomia is not a result of aging per se and should not be dismissed as such. Hyposalivation also can also afflict children who are taking prescription medications for anxiety, depression, compulsive disorders, and attention deficit hyperactivity disorder (ADHD.)41 Salivary function in healthy, non-medicated elders does not vary significantly from younger individuals. It is believed that the increased frequency of dryness complaints with aging is a result of systemic disease and medication use, both more common in elders and both associated with xerostomia.4
As noted earlier, there are non-salivary gland related causes of xerostomia. These include conditions in which there are alterations of oral mucosal sensation or central cognitive changes, such as following a cerebral vascular accident (stroke). Other conditions of drug-induced non-neurally mediated conditions exist. Inhaled medications can cause the sensation of dryness without actually reducing salivary flow. Dryness has been associated with depression, even in the absence of recognizable changes in salivary function. The most common causes of xerostomia, however, are conditions or circumstances that result in alterations in salivary gland function, either quantitative or qualitative.1
Xerostomia is the most common oral side effect caused by medications. There are more than 400 pharmaceuticals that list xerostomia as a side effect (see Table 1 for common medicines).5,6,39,42 The salivary glands are stimulated strongly by cholinergic agents, drugs that stimulate nerve impulses. Therefore, anti-cholinergic medications, such as antihistamines and drugs that treat Parkinson's disease to reduce uncontrolled nerve stimulation are more likely to cause decreased salivary output and xerostomia.5,41 However, many other classes of medications, including sedatives, antipsychotics, antihypertensives, antidepressants, respiratory inhalers, and diuretics are associated with xerostomia.39 Interestingly, many herbal preparations may induce complaints of oral dryness, and patients should always be questioned about non-prescription drug use.7 Examples of commonly used preparations include members of the Labiatae family (specifically all the salvias), capsicum, garlic, Ginkgo biloba, and St. John's Wort (Hypercicum perforatum). Herbal preparations with strong diuretic properties, such as stinging nettle (Urtica dioica) and dandelion (Taraxacum officinale) also may lead to complaints of dry mouth. Caffeine is well recognized as a cause of xerostomia.8 As many as 25 million persons in the United States may experience xerostomia as a result of medication use.
There are also medical therapies that result in xerostomia. Radiotherapy to the head and neck region that includes the salivary glands in the treatment fields can lead to significant and persistent dry mouth. The degree of radiotherapy-induced xerostomia is dose dependent and is related to the amount of salivary gland tissue affected.41 This is an expected complication at exposure levels above 5200 cGy.9,10 Systemically administered radionuclides, such as 131 I for treatment of thyroid cancer, are a recognized cause of dry mouth, particularly when re-treatment is required.11 Bone marrow transplantation also may have xerostomia as a side effect, due to the salivary gland involvement in graft-versus-host disease.12
Another major cause of xerostomia is systemic disease. There are a large number of conditions that can affect salivary gland function and lead to complaints of dryness; including diabetes, thyroid disorders, cystic fibrosis and connective tissue diseases.13 The most prominent disease is Sjögren's syndrome, an autoimmune condition that may affect up to 2.5 million people in the United States, with more than 90% of them being women.43 In approximately 1⁄2 of the cases, Sjögren's syndrome occurs alone, with the other half occurring with another condition such as rheumatoid arthritis, lupus, and scleroderma.
Xerostomia is one of the hallmark symptoms in Sjögren's syndrome, experienced by over 95 percent of patients. The condition is known to progress slowly over time so that most diagnoses are recognized when a person is in their forties to fifties.43 Patients experience a number of dryness complaints in addition to xerostomia. These include eye, nose, throat, skin and vaginal dryness. Since complaints of oral dryness typically do not appear until salivary function has been reduced by approximately 50 percent, more than a single gland must be affected for xerostomia to manifest.15 This emphasizes that dryness resulting from salivary dysfunction is usually indicative of systemic involvement. Table 2 provides a fuller listing of systemic conditions with xerostomia as a possible symptom.
Biologic Process of Salivary Glands
Three major salivary glands are present in the human oral cavity: the parotid, the submandibular and sublingual glands. The parotid and submandibular glands secrete most of the saliva, while the sublingual glands and other minor salivary glands produce the remainder. The parotid gland is located in the cheek just below and in front of the ear. The saliva exits into the mouth through the Stenson's duct, located in the area of the maxillary first and second molars. The submandibular gland lies beneath the mandible in the submandibular fossa. This saliva enters the mouth through the Wharton's duct. The sublingual gland is located more anteriorly and under the floor of the mouth. This saliva enters the mouth under the anterior portions of the tongue through the Bartholin's duct.
Saliva is regulated by both parts of the autonomic nervous system: the sympathetic and parasympathetic systems. Hormones also play a part in this regulation.39 Secretions are often due to some kind of stimulation, such as chewing, speaking, gustatory actions, or taste.41
When at rest, the average adult will secrete about 2 cups of pH-neutral saliva in a 24-hour period, with most of that occurring during the hours they are awake. The waterier saliva, known as serous saliva, is secreted by the parotid gland and aids in digestion. The sympathetic nervous system stimulates the submandibular and sublingual to produce a thicker, more concentrated (mucinous) saliva during the "fight or flight" response and also causes vasoconstriction. This response makes the mouth feel sticky and dry during that anxious or frightening time.41
Minor salivary glands located throughout in the labial mucosa produce about 10% of the total amount of mucinous saliva. This saliva is rich in proteins and carbohydrates and production is essential for maintaining the oral tissue lubrication necessary during eating and talking. Mucinous saliva also prevents penetration of carcinogens, toxins, and oral irritants. Because saliva production is stimulated by the nervous system, any neural health complication can affect salivary production.39,41
Diagnosis of Xerostomia
It is critical that oral health care practitioners recognize xerostomia and salivary gland dysfunction in their patients, as saliva plays an essential role in protection of oral hard and soft tissues and support of oral functions.16 One should follow a systematic assessment approach to the patient with xerostomia: listen for and elicit symptomatic complaints, examine for oral signs of salivary gland dysfunction, and evaluate salivary gland function.
The most frequently voiced complaint is a feeling of dryness of all the oral mucosal surfaces, including the throat (Table 3). Additionally, patients may report difficulty in chewing, swallowing, or speaking. A need to drink fluids to help swallow while eating or an inability to swallow dry foods is also common. Many patients will carry fluids at all times for comfort and to aid in speaking and swallowing. Pain is often reported, and the oral mucosa may be sensitive to spicy or coarse foods, which may limit the patient's diet and enjoyment of meals. Patients may report that their lips and the oral mucosa stick to their teeth. The salivary glands may swell intermittently or chronically. Removable denture wearers commonly report problems with retention and mucosal damage due to lack of lubrication. When denture adhesives are used, they may not fully develop their adhesive and retentive properties through failure to hydrate adequately. Patients should also be questioned concerning dryness in other areas. Eye, throat, nasal, skin or vaginal dryness, in addition to xerostomia, may be indicative of a systemic condition, such as Sjögren's syndrome.
It is recognized that the severity of xerostomia is poorly correlated with salivary gland function. Some individuals tolerate marked (or almost complete) lack of salivation with few complaints, while for others modest decreases in salivary output may trigger severe complaints of dry mouth and oral discomfort. The reasons for this poor correlation are unclear and reflect a lack of knowledge about the elements necessary for oral comfort. Although subjective dryness does not correlate well with measurable salivary gland dysfunction, some symptoms have been found to have predictive value.17 When xerostomia is reported, patients should be questioned in greater detail about its nature, frequency and duration. A thorough evaluation of the patient's medical history must be completed. If questioning reveals difficulties with oral activities dependent on adequate salivation, such as chewing and swallowing, it is likely that salivary function is diminished.
Clinical Assessment of Xerostomia
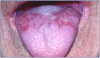
On examination, the patient with xerostomia due to reduced salivary gland function usually has obvious signs of mucosal dryness.1 The lips may be cracked, peeling and atrophic; the buccal mucosa pale and corrugated in appearance; and the tongue smooth and reddened with loss of papillation (Figure 1). The oral mucosa may appear reddened, thinner and more fragile. The patient may show signs of oral ulcerations, angular cheilitis, or complain of a burning sensation in their mouth and tongue known as stomatodyna.39 There is often a marked increase in erosion and dental caries, particularly at the gingival margin, and even cusp tip involvement. The decay may be rapid and progressive even in the presence of excellent oral hygiene (Figure 2). One should consider whether the caries' history and current condition are consistent with the patient's oral hygiene. Candidiasis, most frequently of the erythematous form, is frequent and may contribute to mucosal sensitivity (Figure 3). The salivary glands should be palpated for enlargement, changes in texture, sensation of pain, and also to determine if saliva can be expressed from the main excretory ducts. The saliva should be clear, watery and copious. A cloudy exudate may be a sign of bacterial infection, although some patients with very low salivary output will have opaque secretions that are sterile. After receiving radiation, saliva turns yellowish-brown in color, is thicker, and results in a more acidic pH.41
In addition to these physical effects on the oral cavity, a patient's quality of life is severely impacted.18,19 Since adequate salivary function is important to support alimentation and communication, salivary gland dysfunction and xerostomia may adversely affect some of our most critical activities of daily living. Salivary gland function should be assessed in the patient with xerostomia. This may be done easily in an office setting by determining the total unstimulated output of saliva, termed the whole saliva flow rate. Whole saliva is the mixed fluid contents of the mouth. Using the expectoration model, the patient allows saliva to accumulate in the mouth and then expectorates into a pre-weighed graduated cylinder every 60 seconds, for 5 to 15 minutes.20 To insure an unstimulated sample, patients should refrain from eating, drinking, oral hygiene or smoking for 90 minutes prior to the collection. While inter-individual variability makes it difficult to determine a "normal" value for salivary output, there is agreement on the minimal values necessary to consider salivary output normal. Unstimulated whole saliva flow rates of <0.1 mL/min are considered abnormally low and indicative of marked salivary hypofunction.21,45 A stimulated saliva test can be performed through mastication or by means of citric acid. Stimulated whole saliva flow rates of <0.7 mL/min are considered a low-range output and indicative of marked salivary hypofunction.45 It is important to recognize that output higher than that amount does not guarantee that function is normal. For some individuals, this may be a markedly reduced value. However, this value represents a generally accepted lower limit of normal and is a useful guide for the clinician. Using a well-defined, standardized, and clearly documented procedure for collection will allow meaningful comparisons to published material and with repeat measures in an individual over time.
The composition of the collected saliva may be analyzed (sialochemistry). Over 60 components have been identified in saliva.22 There is increasing interest in salivary diagnostics for systemic and oral diseases.23 Saliva is used currently for determining blood alcohol levels, smoking and drugs of abuse, as well as for HIV testing and detection of exposure to other microbes. Using newer genomic and proteomic techniques, researchers have begun to identify possible salivary biomarkers for a number of oral and systemic conditions. This is a rapidly expanding area of investigation.
Salivary function and gland integrity also can be examined with technetium (Tc) pertechnetate scintiscanning. Uptake of intravenously injected 99mTc tracer from the blood into the glands and subsequent secretion into the oral cavity can be monitored with a gamma camera. Salivary scintiscans correlate well with salivary function and can be used in clinical studies to monitor changes in function following interventions.24
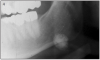
Tumors and structural alterations in the salivary glands can be visualized with sialography, ultrasonography, MRI or CT imaging.25 These techniques are useful to detect. Figure 4 shows a radiograph of a sialolith. These are not functional measures but are useful for diagnosis of salivary dysfunctions.
Biopsy of the salivary glands can be done as well. The most common procedure is biopsy of the minor salivary glands of the lower lip. Minor glands are abundant in this region and can be removed with minimal morbidity.26 Characteristic changes are seen in these glands with Sjögren's syndrome. The labial minor salivary gland biopsy is considered the best sole diagnostic criterion for the salivary component of Sjögren's syndrome.27
Laboratory studies may be helpful in the diagnosis of Sjögren's syndrome. Patients often have characteristic autoimmune alterations in the blood, including the presence of autoantibodies directed against SS-A (Ro) and SS-B (La), antinuclear antibodies and elevated immunoglobulins.
Using a systematic evaluation approach, the cause of dry mouth complaints can be identified in about 80 percent of patients. The remaining 20 percent of the patients are characterized as having idiopathic xerostomia, but still require palliative care for symptomatic relief.
Dental Team's Role and Management of Xerostomia
The dental team has an important role in recognition and management of the patient with xerostomia. With careful attention and regular management, most patients will achieve increased oral comfort and oral complications can be minimized.
Management may be viewed as a series of goals: to provide symptomatic relief of dryness complaints; to institute appropriate preventive measures; to treat any ongoing oral problems; if salivary function is decreased, to stimulate remaining function; and to address the underlying disease process. Management of xerostomia is a team process, involving the entire dental team and the patient's physicians. The medical history must include a complete list of medications so research can be conducted concerning those with a history of causing xerostomia. Effective communication is essential for optimal patient care.
Management starts with patient education and methods to relieve symptoms. These approaches are useful for any patient with dry mouth complaints, regardless of the cause. Recommending frequent sips of water will help to relieve dryness, ease swallowing, hydrate tissues and cleanse the mouth. As noted earlier, many patients with dry mouth carry water with them at all times, and this should be encouraged. Oral rinses and mouthwashes, gels, sprays and artificial salivas are frequently used and may reduce discomfort and improve function transiently. The dental professional should advise the patient to use oral care products that have been specifically formulated for a dry mouth; that is, without alcohol, using only mild detergents and flavorings, having a neutral or alkaline pH, containing no sugar and with added lubricants. The use of chewing gums, lozenges, candies or mints may provide symptomatic relief by stimulating salivation, but they must be sugar-free and non-acidic.
Polyols, such as xylitol or sorbitol, used as a sweetening agent in chewing gums, mouth rinses, and saliva substitutes should be encouraged. Polyols have been shown to inhibit S. mutans in the presence of oral sugars thus limiting bacterial growth and resulting in anti-caries properties.
For dry lips, a hydrating cream or ointment may help relieve symptoms. Use of products with aloe vera or vitamin E should be encouraged. Highly flavored toothpastes should be avoided because they may irritate the dry mucosa and cause pain or sensitivity. A diet that contains moisture-rich foods and not hot or spicy foods may be more comfortable for the patient. Alcohol and caffeine may produce further drying and should be avoided or used only in limited quantities. In addition to its other negative health consequences, smoking may be drying and irritating to the mucosa and should be avoided. An increase in environmental humidity is exceedingly important. Patients, especially in the wintertime, often experience a worsening of their symptoms. Use of room humidifiers, particularly at night, may improve discomfort markedly.
Preventive measures are necessary to minimize oral hard and soft-tissue damage. Patients should be seen on a frequent recare schedule of at least three to six months, until symptoms are minimized and dental caries are controlled.46 They must be instructed in and practice vigilant home oral hygiene. Patients should brush with fluoride toothpaste after each meal. Research has shown that sonic toothbrushing (Sonicare®, Philips Oral Healthcare) increased the salivary rate and significantly lowered the number of incipient lesions after brushing for 1 year over those xerostomia patients using a manual toothbrush.
At a minimum, rinsing the mouth immediately after eating to remove food debris is beneficial. Advice on diet is critical. The dental team must stress the importance of extremely low sugar intake, the use of sugar-free substitutes, and the avoidance of sticky, carbohydrate-rich foods to minimize the caries risk. Alcoholic beverages and mouth rinses containing alcohol are known to dry tissues and these should be avoided.44 Patients should also be aware of the increased risk of tooth wear. Patients must be careful not to consume acidic foods and beverages in excess (e.g. carbonated sodas) in an effort to relieve symptoms.
Patients with dry mouth have an increased risk of fungal infections. Consumption of sugar-free yogurt containing active yeast cultures may help to control oral fungal populations. If a fungal infection is present, appropriate antifungal treatments should be started. Due to the salivary dysfunction, treatment may be prolonged and re-treatment is frequently required. A therapeutic agent should be selected that does not contain sugar as a flavoring agent, as is common in many antifungal lozenges. Nystatin rinses may be prepared by a pharmacist from powder without the added flavoring ingredient(s).
Dental caries management is based on the severity of salivary dysfunction and the observed caries rate. All patients with xerostomia should use some supplemental fluoride, in addition to a toothpaste and oral rinse containing fluoride.44 Selection of the type, dose and frequency of application should be made in consultation between the dental team and the patient. Often a combination of office-applied and home-based fluoride treatments is optimal. Several over-the-counter, sodium fluoride mouth rinses are available for xerostomia patients, including ACT® Total Care Dry Mouth Rinse (Chatten Inc.), Biotene® (GlaxoSmithKline), and Colgate® Dry Mouth Relief (Colgate Oral Pharmaceuticals).41
Stimulating salivary gland flow is effective for relief of dryness symptoms and provides the myriad benefits of natural saliva. Chewing will stimulate salivary flow effectively, as will sour tastes. The combination of chewing and taste, as provided by gums or mints, can be very effective in relieving symptoms for patients who have remaining salivary function. As noted, however, patients must be told not to use products containing sugar as a sweetener. Electrical stimulation of the salivary glands has been attempted, but application is a challenge and the results have been modest at best. Presently, newer devices are being investigated and show promise for the future.28
Systemic drugs, termed a sialogogue, may be prescribed. The Food and Drug Administration (FDA) has approved two medications for the relief of dry mouth symptoms in Sjögren's syndrome: pilocarpine (Salagen®, Eisai, and generics) and cevimeline (Evoxac® capsules, Daiichi-Sankyo, and generics).29-31,42,44 These medications are parasympathomimetic, muscarinic agonists, which induce a transient increase in salivary output and statistically significant improvement in complaints of oral dryness. Common side effects of both medications include sweating, flushing, urinary incontinence and gastrointestinal discomfort. While rarely severe or serious, side effects are frequent and may limit the usefulness of these agents in some individuals. Parasympathomimetics are contraindicated in patients with uncontrolled asthma, narrow-angle glaucoma, and acute iritis and should be used with caution in patients with significant cardiovascular disease, Parkinson disease, asthma and chronic obstructive pulmonary disease. Pilocarpine is recommended at a dosage of 5 mg up to four times daily, while cevimeline is prescribed at 30 mg three times daily. These medications are widely used and provide significant relief of dryness complaints in many patients. Pilocarpine has also been approved for treatment of xerostomia related to head and neck radiotherapy (Figure 5).
A number of different approaches have been attempted to address the underlying disease process and therefore improve salivary gland dysfunction, particularly in Sjögren's syndrome. Current studies are targeting specific biologic pathways to modify the underlying autoimmunity.
Very low dose interferon-alpha, 150 or 450 IU once or three times a day orally, has been studied in primary Sjögren's syndrome. Use of 150 IU interferon-alpha three times daily resulted in increased stimulated whole salivary flow rates at 12 weeks compared to placebo.32 A subsequent phase 3 trial at this dose found increased unstimulated salivary function compared to placebo at 24 weeks. However, the co-primary endpoints of stimulated whole saliva flow and oral dryness were not significantly improved relative to placebo,33 and further clinical studies will be necessary.
Another approach has been to modify the inflammatory cytokine pathway, specifically targeting tumor necrosis factor alpha (TNFa). Anti-TNFa agents, including infliximab, etanercept and thalidomide, which have shown benefit in rheumatoid arthritis and lupus erythematosus, have shown no significant efficacy in randomized controlled trials in Sjögren's syndrome.34-36
At present, there is interest in modulation of B-cell activation. As there is well-documented B-cell hyperreactivity in Sjögren's syndrome, this approach may have an impact on the underlying disease. Rituximab is a humanized monoclonal antibody that binds specifically to the CD20 antigen, which is present on B lymphocytes and is involved in cell activation. In an open-label study, improvements in symptoms of dry mouth and salivary gland function were demonstrated.37 Although these results are promising, a randomized controlled trial is necessary before recommendation of this treatment option for Sjögren's syndrome. A recent open-label trial looked at an anti-CD22 monoclonal antibody and reported very promising results in Sjögren's syndrome.38 Further studies are anticipated.
The February 2012 edition of JADA news reported a study using acupuncture to reduce xerostomia in patients receiving radiation therapy for head and neck cancer. The researchers of the study measured the patient's salivary flow in stimulated and unstimulated situations using standardized sialometry collection techniques. After one month and six months of receiving radiotherapy, salivary rates were greater in those patients receiving acupuncture.40
Management of xerostomia requires a team approach. The dental team should work together closely to minimize the patient's dryness complaints and to preserve and protect the oral tissues. Patient education is key. The dental team needs to explain the oral sequelae of dry mouth and the problems and issues patients may encounter in their daily lives. The oral condition needs to be assessed and monitored closely, and issues such as oral hygiene care and diet should be emphasized. Consultation with the patient's physician is indicated if, for example, the xerostomia appears to be related to medication use. In this case, discussion of alternative medications or dosing regimens to minimize xerostomia is indicated. If systemic disease is suspected as the underlying cause of salivary dysfunction, patients should be referred to their physician or an appropriate specialist without delay. Ongoing review and monitoring of the patient's oral and general health are important for optimal management.
Summary
Awareness and recognition of xerostomia are essential in order to help patients minimize dryness symptoms, to institute preventive measures and to limit oral complications. The dental professional has the opportunity to ask every patient if they are experiencing dry mouth. In particular, complaints of dryness while eating, or difficulty swallowing dry foods, or the necessity of using liquids to ease swallowing are important clues that salivary function may be impaired. As part of a routine oral examination, one should examine the oral cavity carefully for signs of salivary gland dysfunction. Findings such as an increase in caries activity, mucosal alterations, infection or salivary gland enlargement may indicate salivary dysfunction. Evaluation should be conducted proactively at each patient visit. Early recognition will minimize damage and dysfunction and allow appropriate management to begin. Although the salivary dysfunction may be irreversible, preventive measures and conservative treatments can avoid or limit mucosal breakdown, infections and permanent damage to teeth. Adequate symptomatic relief is possible with local palliative and systemic measures in many patients. Appropriate management of symptoms and increasing saliva output may help patients feel more comfortable and improve their quality of life.
Glossary
Alimentation - giving or receiving nourishment.
Angular cheilitis - an inflammatory lesion in the corners of the mouth (commissure).
Anticholinergic - an agent that blocks parasympathetic nerve impulses.
Autoantibody - acting against antigenic tissue products of the same organism in which it is formed.
Autoimmunity - the condition in which antibodies are produced against the body's own tissues.
Chronic - of long duration.
Cognitive - mental process such as problem solving, memory and language.
Dysgeusia - altered sense of taste.
Erythematous - redness of the skin.
Halitosis - bad breath.
Hypo - low.
Idiopathic - condition without clear pathogenesis or disease without recognizable cause.
Immunoglobulin - one of a family of closely related though not identical proteins capable of acting as antibodies.
Labiatae family - a large family of aromatic herbs and shrubs having flowers.
Parasympathomimetic - producing effects similar to those resulting from stimulation of parasympathetic nervous system.
Radionuclide - atom that disintegrates by emission of electromagnetic radiation.
Sialogogue - a drug or other agent that increases the flow of saliva.
Sialotic - concerning the flow of saliva.
Sjogren's syndrome - an autoimmune disease, causing decreases in saliva and tear production.
Stomatodyna - burning mouth and tongue sensation.
Systemic - pertaining to a whole body rather than to one of its parts.
Ultrasonography - use of ultrasound to produce an image or photograph of an organ or tissue.
References
1. Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc 2003; 134(1): 61-9.
2. Atkinson JC, Grisius M, Massey W. Salivary hypofunction and xerostomia: diagnosis and treatment. Dent Clin North Am. 2005; 49(2): 309-26.
3. Orellana MF, Lagravère MO, Boychuk DG, et al. Prevalence of xerostomia in population-based samples: a systematic review. J Public Health Dent 2006; 66(2): 152-8.
4. Ship JA, Pillemer SR, Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc 2002; 50(3): 535-43.
5. Ciancio SG. Medications' impact on oral health. J Am Dent Assoc 2004; 135(10): 1440-8.
6. Sreebny LM. Saliva in health and disease: an appraisal and update. Int Dent J 2000; 50(3): 140-61.
7. Abebe W. An overview of herbal supplement utilization with particular emphasis on possible interactions with dental drugs and oral manifestations. J Dent Hyg 2003; 77(1): 37-46.
8. Sreebny LM, Schwartz SS. A reference guide to drugs and dry mouth-2nd edition. Gerodontology. 1997; 14(1): 33-47.
9. Sciubba JJ, Goldenberg D. Oral complications of radiotherapy. Lancet Oncol 2006; 7(2): 175-83.
10. Dirix P, Nuyts S, Van den Bogaert W. Radiation-induced xerostomia in patients with head and neck cancer: a literature review. Cancer. 2006; 107(11): 2525-34.
11. Mandel SJ, Mandel L. Radioactive iodine and the salivary glands. Thyroid 2003; 13(3): 265-71.
12. Woo SB, Lee SJ, Schubert MM. Graft-vs.-host disease. Crit Rev Oral Biol Med 1997; 8(2): 201-16.
13. von Bültzingslöwen I, Sollecito TP, Fox PC, et al. Salivary dysfunction associated with systemic diseases: systematic review and clinical management recommendations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103 Suppl: S57.e1-15.
14. Kassan SS, Moutsopoulos HM. Clinical manifestations and early diagnosis of Sjögren syndrome. Arch Intern Med 2004; 164(12): 1275-84.
15. Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res 1987; 66 Spec No: 648-53.
16. Dodds MW, Johnson DA, Yeh CK. Health benefits of saliva: a review. J Dent 2005; 33(3): 223-33.
17. Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc 1987; 115(4): 581-4.
18. Ikebe K, Matsuda K, Morii K, et al. Impact of dry mouth and hyposalivation on oral health-related quality of life of elderly Japanese. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 103(2): 216-22.
19. Perno Goldie M. Xerostomia and quality of life. Int J Dent Hyg 2007; 5(1): 60-1.
20. Navazesh M. Methods for collecting saliva. Ann NY Acad Sci 1993; 694: 72-7.
21. Sreebny L. Saliva-salivary gland hypofunction (SGH). FDI Working Group 10. J Dent Assoc S Afr 1992; 47(11): 498-501.
22. Pesce MA, Spitalnik SL. Saliva and the clinical pathology laboratory. Ann NY Acad Sci 2007; 1098: 192-9.
23. Chiappin S, Antonelli G, Gatti R, De Palo EF. Saliva specimen: a new laboratory tool for diagnostic and basic investigation. Clin Chim Acta 2007; 383(1-2): 30-40.
24. Baur DA, Heston TF, Helman JI. Nuclear medicine in oral and maxillofacial diagnosis: a review for the practicing dental professional. J Contemp Dent Pract 2004; 5(1): 94-104.
25. Thoeny HC. Imaging of salivary gland tumours. Cancer Imaging 2007; 7: 52-62.
26. Fox PC. Simplified biopsy technique for labial minor salivary glands. Plast Reconstr Surg 1985; 75(4): 592-3.
27. Daniels TE. Labial salivary gland biopsy in Sjögren's syndrome. Assessment as a diagnostic criterion in 362 suspected cases. Arthritis Rheum 1984; 27(2): 147-56.
28. Strietzel FP, Martín-Granizo R, Fedele S, et al. Electrostimulating device in the management of xerostomia. Oral Dis 2007; 13(2): 206-13.
29. Vivino FB, Al-Hashimi I, Khan Z, et al. Pilocarpine tablets for the treatment of dry mouth and dry eye symptoms in patients with Sjögren syndrome: A randomized placebo- controlled fixed-dose multicenter trial. Arch Intern Med 1999; 159: 174-181.
30. Fife RS, Chase WF, Dore RK, et al. Cevimeline for the treatment of xerostomia in patients with Sjogren syndrome: a randomized trial. Arch Intern Med 2002; 162(11): 1293- 1300.
31. Petrone D, Condemi JJ, Fife R, et al. A double-blind, randomized, placebo-controlled study of cevimeline in Sjogren's syndrome patients with xerostomia and keratoconjunctivitis sicca. Arthritis Rheum 2002; 46(3): 748-54.
32. Ship JA, Fox PC, Michalek JE, et al. Treatment of primary Sjögren's syndrome with lowdose natural human interferon- alpha administered by the oral mucosal route: a phase II clinical trial. IFN protocol study group. J Interferon Cytokine Res 1999; 19: 943-51.
33. Cummins MJ, Papas A, Kammer GM, Fox PC. Treatment of primary Sjogren's syndrome with low-dose human interferon alfa administered by the oromucosal route: combined phase III results. Arthritis Rheum 2003; 49: 585-93.
34. Mariette X, Ravaud P, Steinfeld S, et al. Inefficacy of infliximab in primary Sjogren's syndrome: results of the randomized, controlled trial of Remicade in Primary Sjogren's Syndrome (TRIPSS). Arthritis Rheum 2004; 50(4): 1270-6.
34. Sankar V, Brennan MT, Kok MR, et al. Etanercept in Sjogren's syndrome: a twelve-week randomized, double-blind, placebo-controlled pilot clinical trial. Arthritis Rheum 2004; 50(7): 2240-5.
36. Pillemer SR, Leakan RA, Sankar V, et al. Prominent adverse effects of thalidomide in primary Sjogren's syndrome. Arthritis Rheum 2004; 51(3): 505-6.
37. Pijpe J, van Imhoff GW, Spijkervet FK, et al. Rituximab treatment in patients with primary Sjogren's syndrome: an open-label phase II study. Arthritis Rheum 2005; 52(9): 2740-50.
38. Steinfeld SD, Tant L, Burmester GR, et al. Epratuzumab (humanized anti-CD22 antibody) in primary Sjögren's syndrome: an open-label phase I/II study. Arthritis Res Ther 2006; 8(4): R129.
39. Noble WH, Aziz A, Edwards K, Salmon E. Xerostomia from A to Z. Dimensions of Dental Hygiene. January 2012; 22-28.
40. JADA News. February 2012. Acupuncture may reduce xerostomia in patients with head, neck cancer, study finds. 143(2) pg.111.
41. Spolarich A. Xerostomia and oral disease. Dimensions of Dental Hygiene - Special Continuing Education Supplement. November 2011.
42. Claiborne, DM. Medication use and Xerostomia. Dimensions of Dental Hygiene. November 2012; 34-38.
43. Little, J.W., Miller, C.S., Rhodus, N.L. (2018.) Dental Management of the Medically Compromised Patient. 9th ed., St. Louis: Elsevier
44. ADA Oral Health Topics: Xerostomia. Ada.org. Accessed 10.12.2017
45. Tanasiewicz, M, Hildebrandt, T, and Obersztyn I. Xerostomia of Various Etiologies: A Review of Literature. Adv Clin Exp Med 2016, 25, 1, 199-206.
46. Plemmons, JM. Et al. Managing xerostomia and salivary gland hypofunction. J Am Dent Assoc 2014; 145(8): 867-73.
About the Author
Philip C. Fox, DDS, FDS, RCSEd
Philip C. Fox received his BA and DDS degrees from Columbia University and completed training in oral and maxillofacial surgery at Harlem Hospital Center, New York, N.Y. and a fellowship in oral medicine at the National Institutes of Health in Bethesda, Md. He was a member of the National Institute of Dental and Craniofacial Research, National Institutes of Health, for 22 years, serving as chief of the Clinical Investigations Section, Gene Therapy and Therapeutics Branch, and as clinical director of the Intramural Research Program.
At present, he is a visiting scientist at the Department of Oral Medicine, Carolinas Medical Center, in Charlotte, N.C., and an independent biomedical consultant focusing primarily in the area of clinical trial design and analysis. He is a diplomate of the American Board of Oral Medicine.
About the Contributing Author
Wilhemina R. Leeuw, MS, CDA
Wilhemina R. Leeuw is a Clinical Assistant Professor in the Department of Dental Education at Indiana University - Purdue University Fort Wayne, located in Fort Wayne, Indiana. A DANB Certified Dental Assistant since 1985. She worked in private practice over twelve years before beginning her teaching career. She received her Baccalaureate and Master's degrees in Organizational Leadership and Supervision from IPFW. She has authored for the American Dental Assistant's Association and is currently serving as a CODA Accreditation site visitor. She is very active in her local and Indiana state dental assisting organizations. Her educational background includes dental assisting - both clinical and office management.