You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
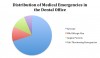
An understanding of which emergencies occur most commonly provides a foundation for comprehending the medications and equipment that are most likely to be needed. A study by Malamed, which included two surveys of more than 4,000 dentists, found that more than 30,000 incidents were reported to have occurred over a 10-year period.1 Among the 30,608 incidents analyzed, vasovagal syncope accounted for more than 15,000 events. Other surveys have reported even higher incidences, ranging from 57% to 67%.2-4 The next most common in Malamed’s analysis were mild allergic reactions (2,583), angina pectoris (2,552), and postural hypotension (2,445). Also occurring with some frequency were seizures (1,595), asthma attacks (1,392), hyperventilation (1,326), epinephrine reactions (913), and hypoglycemia (890).
Incidents and Emergencies
A breakdown of emergencies analyzed by Malamed (Figure 1) shows that more life-threatening events (including cardiac arrest, anaphylactic reaction, myocardial infarction, local anesthetic overdose, acute pulmonary edema, diabetic coma, cerebrovascular accident, adrenal insufficiency, and thyroid storm) were reported a total of 1,475 times, constituting 4.8% of the total incidents. Compared with the 2,583 mild allergic reactions, anaphylaxis occurred only 304 times. Compared with the 2,552 incidents of angina, only 289 reported myocardial infarctions and 331 cardiac arrests occurred. If a mild allergic reaction or an angina attack can be intercepted appropriately, it will hopefully not develop into a more severe and life-threatening event such as anaphylaxis, myocardial infarction, or cardiac arrest.
Depending on the malpractice liability insurance carrier and the specific state board governing any given practice, requirements for emergency kits may vary. Furthermore, a higher-risk patient base and unusual patient comorbidities may make it desirable to expand beyond a basic kit. However, in conjunction with an oxygen tank and an automated external defibrillator (AED), most commercially available emergency kits are generally adequate. These kits provide a systematic way to organize their contents, and some manufacturers have even devised systems for alerting the practice staff when medications contained in the kit have expired.
Any emergency situation can be stressful. To be best prepared, it is advisable to thoroughly understand the most important components of emergency readiness. These can be loosely divided into equipment and medications. Among the former are equipment used for airway-related emergencies, cardiovascular emergencies, and other miscellaneous situations. Medications may be broadly divided into injectable and non-injectable drugs. The remainder of this article will discuss emergency equipment and non-injectable medications. Part 2 will be devoted to injectable drugs.
Emergency Equipment
Airway Equipment
Figure 2 displays an E tank of oxygen with an attached regulator. The function of the regulator is to lower the pressure inside the tank (typically 2,000 pounds per square inch) to one that the patient can breathe without injuring the lungs. The black knob at the end of the regulator adjusts the flow rate. Next to the knob, the flow rate (in meters per minute) is displayed. Below that is an attachment for the nasal cannula or oxygen tubing that attaches to a bag valve mask; this may also be called the “nipple” or “Christmas tree.” On the right, the small knob is used to tighten the regulator onto the yoke of the tank. A wrench on the top is used to open and close the tank.5-7
All medical gas tanks are color-coded to prevent any confusion between oxygen and nitrous oxide sources. In the United States, oxygen tanks are always green, while nitrous oxide tanks are blue. However, the wrenches may be various colors including blue, black, gray, and silver. The pin index safety system helps to prevent any cross-assembly of oxygen and nitrous oxide tanks. Figure 3 displays the pin index safety system intended for supplying oxygen. As shown, the holes on the yoke assembly of the tank match the pins on the regulator that correspond to the tank. The pins and holes have a unique lock-and-key configuration for each gas. The locations of the pins on the yoke assembly of the oxygen tank are in a different position than those intended for nitrous oxide tanks. This is one safety mechanism to prevent the administration of incorrect gases.
Other airway equipment includes a nasal cannula, pocket mask, and bag valve mask (Figure 4). The nasal cannula is typically used to deliver supplemental oxygen to a patient who has been breathing on his or her own. A patient who is not breathing spontaneously will need assisted breaths delivered by the bag valve mask.5-7
Another piece of equipment that can be used as an adjunct for bag valve ventilation is the oropharyngeal airway. As shown in Figure 5, the red area is a bite block that rests between the incisors. The curved part goes behind the tongue, creating space behind the tongue and the pharynx to allow for gas exchange. Several bite block sizes are typically included in emergency kits. To determine the best fit for any patient, the bite block should be held next to the patient’s face, near the incisors. If the tip of the airway reaches the angle of the mandible, the airway is apt to fit well.5-7
A tongue blade can also be helpful for visualization of the oral cavity. If any debris such as a piece of gauze or crown is present, a Magill forceps can be used to retrieve it. This forceps is long and curved, and extends all the way to the back of the airway. The long, curved design of the Yankauer suction tip is better suited for extracting debris from the back of the airway than the regular dental suction or saliva ejector. A battery-powered backup suction device is a recommended piece of emergency equipment for two reasons. If electrical power in the office is lost in the middle of a procedure, battery-powered backup suction can enable the procedure to still be completed safely. Also, if an emergency develops outside the operatory such as in the waiting room, the backup suction can be carried to the patient.5-7
Cardiovascular Equipment
A stethoscope and sphygmomanometer are essential cardiovascular emergency equipment. Even if the practice is equipped with an automated blood pressure monitor, it is prudent to have a manual cuff in the event of monitor malfunctions. A stethoscope can be beneficial in several circumstances. It can be used to listen to the heart or lungs for sounds such as wheezing during an asthma attack. Routine monitoring of blood pressure and heart rate is recommended for any patient receiving dental treatment. In fact, the instructions for use on local anesthetic cartridges state that cardiovascular and respiratory vital signs and the patient’s state of consciousness should be monitored after each local anesthetic injection.5-7
Another essential piece of equipment is an automated external defibrillator (AED). It is incumbent upon all providers and staff to understand the use of and be familiar with the AED now that it is a required component of basic life-support cardiopulmonary resuscitation (BLS-CPR) certifications. When the AED is purchased, it is essential to ensure that it contains functional batteries. Different AED brands use different types of batteries which, in turn, can be charged in different ways. Healthcare professionals must also understand how to operate their particular AED model and ensure it is in proper working condition with the appropriate battery and pads to deliver shocks. The medical device sales representative should be consulted to verify that all components are included when purchasing an AED.5-7
Cardiopulmonary resuscitation (CPR) is effective if the person is laying on a flat surface. A CPR board permits a flat surface in the dental chair. If a patient requires CPR, it may not be possible to safely move him or her to the floor, depending on the person’s size and physical condition. If necessary, a CPR board placed under the patient’s back in the dental chair can provide the necessary flat surface.5-7
Miscellaneous Equipment
A glucometer should be available to check the patient’s blood sugar in cases of suspected hypoglycemia. Also, a backup-powered light source is recommended for use in case of a power outage or a medical emergency occurring outside the operatory. This might consist of a flashlight or even a loupe headlamp that incorporates a battery-powered light. Syringes, needles, wipes, and tape should also be included in the medical kit.5,7
Emergency Non-Injectable Medications
Several non-injectable medications should be available in response to various emergencies that may develop within the dental practice. Below are the recommended medications.
Oxygen
Oxygen, which is responsible for all vital life functions and all aerobic metabolic processes, is indicated for treating virtually every medical emergency. Oxygen should be administered at the rate of 4 L/min to 6 L/min via nasal cannula to spontaneously breathing patients, and delivered to apneic patients via a bag valve mask at the rate of about 10 L/min to 15 L/min.6,8
The sole contraindication for oxygen is hyperventilation. However, serious conditions (eg, an asthma exacerbation or angina attack) can mimic hyperventilation. In these cases, the patient may be breathing rapidly and looking panicky; such patients should not be deprived of oxygen. If hyperventilation is suspected, the patient should be encouraged to take deep, slow breaths. The popular remedy of breathing in and out of a paper bag has been discredited because in situations where the patient needs oxygen, this can actually make him or her feel worse. Long, deep breaths will help with anxiety and hyperventilation but again, if angina or asthma is suspected, oxygen should be administered. Then, if the patient is clearly not benefiting or worsening, the nasal cannula can be removed and the patient can return to breathing air.7,9
Nitrous oxide
Nitrous oxide is another inhaled medication that can be useful, particularly if the practice staff is properly trained in its routine administration. It has several indications, but most relevant to the present discussion is the fact that nitrous oxide provides analgesia during an acute myocardial infarction. The mechanism of this action may involve noradrenergic pathways, the endogenous opioids, or the gamma-aminobutyric acid (GABA) receptors.6,7
Administration is via nasal hood. Starting with a mixture of 100% oxygen and 0% nitrous oxide, the nitrous-oxide component should be increased after a couple minutes to roughly 20%. The patient’s response should be monitored for a minute or so, and then the nitrous oxide should be increased by 10% increments over the next few minutes. Most patients will experience analgesia at levels of 35% to 50% nitrous oxide. It is worth noting that room air consists of only 21% oxygen. Therefore, a patient who is breathing a 50/50 mixture of nitrous oxide and oxygen is still receiving more oxygen than is present in room air. After any administration of nitrous oxide, the patient should be encouraged to breathe 100% oxygen for 3 to 5 minutes to prevent any diffusion hypoxia.6,7
Among the few contraindications to using nitrous oxide, one is pregnancy. Anecdotal evidence has linked nitrous-oxide exposure with miscarriages early in pregnancy. It must also be noted that nitrous oxide is 35 times more soluble than atmospheric nitrogen (N2). As a consequence, nitrous oxide can expand within closed body cavities and create pressure within them. It is thus contraindicated for patients who have obstructed bowels, blocked ear tubes, or acute sinus blockages. Some anatomic variations, such as a deviated septum, may also make nitrous-oxide administration difficult. Additionally, patients who have a methylenetetrahydrofolate reductase deficiency, which is an enzymatic problem, are not good candidates for receiving nitrous oxide either.6,7
If the provider is not proficient in establishing intravenous (IV) access, then attempting to start an IV during emergencies such as a myocardial infarction may be difficult, and continued attempts may increase pain and stress for the patient. If the patient cannot breathe through his or her nose, the patient can be instructed to hold the mask over his or her mouth instead. In the case of a myocardial infarction, this should be done after the administration of nitroglycerin and aspirin. Having the patient hold the mask over his or her own mouth may provoke less anxiety, as it gives the patient some degree of control over the mask position.7
Albuterol
Another important inhalational medication is albuterol. It works as a selective beta-2 agonist. The beta-2 activation mediates bronchodilators. Because albuterol has minimal beta-1 effects such as tachycardia, albuterol is a drug of choice for acute bronchospasms that may occur during asthma or allergic reactions. The contraindication for albuterol is if there is a hypersensitivity to the medication or any of its components.5,10,11
Proper administration of albuterol is important. Any inhaler that is new or has not been used in 2 or more weeks must be shaken thoroughly and primed before use. Priming is accomplished by releasing about four pumps of the inhaler into the air. While most asthmatic patients have experience using inhalers, some may not. They may be having a bronchospasm for the first time or having one as a result of an allergic reaction. Any such patient should be instructed to exhale and then bring the inhaler to his or her mouth. As he or she slowly inhales, the patient should pump the inhaler, continuing to breathe in as slowly and deeply as possible. The patient should then hold their breath for about 10 seconds, remove the inhaler, and exhale. This will help transmit the medication down into the tracheobronchial tree. About two to three puffs can be administered every 1 to 2 minutes. This can be repeated as needed, up to three times.5,10,11
Some asthmatic patients use an inhaled corticosteroid medication daily as a baseline anti-asthma agent to reduce airway inflammation reactivity. The albuterol inhaler, on the other hand, is known as a “rescue inhaler” because it is taken in response to an acute asthma attack. It may be prudent to instruct patients to bring their own albuterol inhaler with them when they are scheduled to receive dental treatment, as stress associated with such treatment may exacerbate their asthma. Certainly, it is important to assess the success of any asthmatic patient’s control over their condition when taking a medical history. Albuterol, also on rare occasion, may cause a life-threatening paradoxical bronchospasm. In such an event, use of the rescue inhaler should be discontinued, and the patient should be transferred to an emergency room. Paradoxical bronchospasm often occurs with the initial use of a new inhaler; that is why it is essential to shake the inhaler well and pump it before administrating it to any patient.5,10,11
Smelling Salts
Syncope is one of the most common medical emergencies in the dental office. Smelling salts, also known as pneumonia inhalants or aromatic spirits of pneumonia, provide a quick and noninvasive way to rouse a semiconscious or unconscious patient. The ammonia inhaler is activated by pinching it between the fingers (Figure 6). With an odor reminiscent of hair dye, the inhalants are a very strong irritant. Deep or prolonged inhalation should be avoided, as it may result in headaches, dizziness, difficulty breathing, lung inflammation, and even pulmonary edema. Any contact with the eyes or skin also must be avoided, as it can burn or injure the tissue. Ingestion of ammonia inhalants may cause nausea, vomiting, diarrhea, and even death.5,12
Aspirin
Though used for pain relief since antiquity, aspirin recently has become recognized as a lifesaving drug. It has been shown to reduce the overall mortality from acute myocardial infarction, and it prevents cardiac ischemia from progressing to acute myocardial infarction. It works via the irreversible acetylation of the platelet’s cyclooxygenase (COX) enzyme. This prevents clot formation. Within the context of medical emergencies in the dental office, the principal indication is suspected acute myocardial infarction.5,13-15
Contraindications include having a known allergy to aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) or having asthma that is sensitive to aspirin or NSAIDs. Significant gastrointestinal bleeding is also a relative contraindication. The most effective dose is not known with certainty, but a minimum of 162 mg (eg, two “baby aspirin”) should be given immediately to anyone with pain suggestive of an acute myocardial infarction.
Nitroglycerin
Nitroglycerin, delivered sublingually, dilates the blood vessels. By reducing bloodflow to the coronary arteries and the oxygen requirements for the heart, nitroglycerin relieves coronary artery spasms. The indication for it is angina pectoris. Contraindications include hypersensitivity to nitroglycerin, nitrates, nitrites, or other components of the drug. Another notable contraindication is hypotension. The patient’s blood pressure should be checked, and if the systolic pressure is below 90, nitroglycerin should not be administered.5,16
Each tablet or spray contains 0.4 mg of nitroglycerin. A dose consists of either one spray or one tablet, but not both. After a dose has been delivered under the patient’s tongue, the patient should be closely monitored for 5 minutes. If no improvement occurs, another dose can be administered. After 5 more minutes, if no improvement is evident, one more dose may be given (a total of three). After that, if no improvement occurs, it should be assumed that the patient is suffering from an acute myocardial infarction.5,16
Once nitroglycerin tablets have been opened and exposed to light, their shelf life is 3 months. The shelf life for the spray is marked on the tube.5,16
Oral Carbohydrates
Oral carbohydrates serve as a source of glucose (the fuel needed for all metabolic processes). They are indicated for conscious patients who have acute hypoglycemia. There are no contraindications, as the dangers of acute hypoglycemia outweigh the dangers of acute hyperglycemia, even in diabetic patients. Hypoglycemic patients typically appear shaky, dizzy, sweaty, hungry, irritable, anxious, or nervous. A headache may be present as well. More severe symptoms are immediate and life-threatening; they include muscle weakness, jerky movements, slurred speech, visual disturbances, drowsiness, seizures, and unconsciousness. Shock and even death may result.5
The definitive treatment for hypoglycemic shock is 50% dextrose in water administered through an IV. However, since IV access is not routinely achieved in the dental office for most dental procedures, the carbohydrate can also be administered orally to any patient who is showing signs of hypoglycemia. Conscious patients should be instructed to eat or sip from a carbohydrate source. That could be juice, soda (as long as it is not a diet soda), Insta Glucose, or frosting. Oral carbohydrates should never be administered to an unconscious patient because of the risk for aspiration into the lungs.5
Conclusion
All dental practices should be prepared for the rare instance in which it faces a medical emergency, whether it is for a patient or a fellow staff member or other visitor to the practice. There are certain equipment and medications that should be contained in any standard dental practice emergency kit, and everyone in the practice should know where the kit is located, as well as how to use the equipment and administer the medications it contains. In the second part of this two-part series, injectable medications that can be used in the course of a medical emergency in the dental practice will be thoroughly reviewed.
ABOUT THE AUTHOR
Dr. Saraghi is an attending anesthesiologist at St. Barnabas Hospital, Bronx, NY. She is a member of the American Society of Dental Anesthesiologists and the American Dental Society of Anesthesiology. She maintains a private practice in New York City.
Disclosure
Dr. Saraghi has received an honorarium for writing this article.
References
1. Malamed SF. Medical Emergencies in the Dental Office. 6th ed. St Louis, MO: Mosby Elsevier, 2007.
2. Fast TB, Martin MD, Ellis TM. Emergency preparedness: a survey of dental practitioners. J Am Dent Assoc. 1986;112(4):499-501.
3. Müller M, Hänsel M, Stehr S, et al. A state-wide survey of medical emergency management in dental practices: incidence of emergencies and training experience. Emerg Med J. 2008;25(5):296-300.
4. Girdler N, Smith D. Prevalence of emergency events in British dental practice and emergency management skills of British dentists. Resuscitation. 1999;41(2):159-167.
5. Rosenberg M. Preparing for medical emergencies: the essential drugs and equipment for the dental office. J Am Dent Assoc. 2010;141(Suppl 1):14S-19S.
6. Morgan GE, Mikhail MS, Murray MJ. Clinical Anesthesiology. 4th ed. New York, NY: The McGraw-Hill Companies, 2005.
7. Malamed SF. Sedation: A Guide to Patient Management. 5th ed. St Louis, MO: Mosby Elsevier, 2010.
8. Hall JE. Guyton and Hall Textbook of Medical Physiology. 12th ed. Philadelphia, PA: Saunders Elsevier, 2011.
9. Cornet AD, Kooter AJ, Peters MJL, Smulders YM. Supplemental oxygen therapy in medical emergencies: More harm than benefit? Arch Intern Med. 2012;172(3):289-290.
10. Proventil HFA (albuterol sulfate) [package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 2012.
11. National Heart, Lung, and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. 2007. http://www.nhlbi.nih.gov/files/docs/guidelines/asthgdln.pdf
12. Ammonia Inhalant Solution [package insert]. Big Flats, NY: X-GEN Pharmaceuticals, Inc.; 2015.
13. Aspirin [package insert]. Morristown, NJ: Bayer Corporation; 2011.
14. Patrono C. Aspirin as an antiplatelet drug. N Engl J Med. 1994;330(18):1287-1294.
15. Schror K. Antiplatelet drugs: a comparative review. Drugs. 1995;50(1):7-28.
16. Nitrostat® nitroglycerin tablet [package insert]. New York, NY: Parke-Davis Division of Pfizer Inc.; 2014.