You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The term "technology in dentistry" is often equated with the use of CAD/CAM. The phenomenon of CAD/CAM in dentistry has occupied the attention of much of the scientific dental literature as a result of its standing within the scope of dental practice.1 It is only a matter of time before digital technologies replace non-digital/analog technologies for creating prostheses and developing diagnostic scenarios toward the improvement of patient care.2
Pediatric dentistry is the only specialty discipline of dentistry that cares for a specific population of patients rather than a particular condition. Therefore, pediatric dentistry must provide continuous care to all its patients using all types of treatment, including modern technology. Technological development within other disciplines of dentistry will lead to pediatric dentistry deployment of many of the techniques and science created initially to care for adults. In addition, with the availability of literature towards demonstration of digital technologies in the public domain, patients themselves as well as parents (regarding their children) are asking for the latest technologies.3
This article will review the historical use of dental impressions and then explore the use of digital workflow, including CAD/CAM, and its potential to become the dominant means of care in pediatric dentistry.
Uses of Impressions in Pediatric Dentistry
There are many areas where impressions are used during patient care in pediatric dentistry. Most commonly, impressions are made for study models. Study models are used for diagnostic purposes, to analyze the state of occlusion, to evaluate space and/or space loss, to assist in the determination of the status of growth and development, and in general, to demonstrate to the patient's caregivers the need for specific types of care.4
Besides study models, impressions are used for a variety of additional purposes. Commonly, space maintainers are fabricated when a primary molar is lost prematurely due to infection or other reasons. Space maintainers are necessary to preserve the arch length or to avoid malocclusions that are preventable. Impressions are made for a single quadrant in the case of a band and loop appliance or for a full arch in the case of appliances that will span the entire arch, such as a lower lingual holding arch or a transpalatal arch. In addition, impressions are made for active appliances to treat malocclusions in the early stages of the primary dentition as well as in the permanent dentition.5
With the use of stock crowns made of zirconia and with the increasing use of esthetic materials in pediatric dentistry as well as for adults, it has become clear that the need for precision crowns fabricated in a low-cost fashion made specifically for individual patients will be desired. Just as such appliances are created for permanent teeth on a routine basis and are one of the major uses of CAD/CAM technology, these types of prostheses will become possible and likely even prevalent in the near future for pediatric dentistry also, because improvements in the technology lower pricing considerably.6 This author and colleagues work together with prosthodontists and other specialists to create transitional appliances using CAD/CAM technology for patients who have, for example, hypodontia, which may occur with ectodermal dysplasia. The uses of CAD/CAM technologies as typically deployed in prosthodontics and that may become incorporated into pediatric dental treatments may allow distinct advantages not available previously.
The creation of space-maintainer appliances or active appliances to correct malocclusions requires an accurate and stable impression to form a model that will represent the actual scenario in the patient's mouth.7 This is not always possible through traditional means for a variety of reasons, as described below.
Traditional Method/Workflow With Impressions
The traditional technique using impressions requires a very specific process that is sometimes challenging for young children. For all the above-mentioned appliances, including study models, alginate is the material most commonly used, because it is inexpensive and easy to mix and sets very quickly. These features, particularly the fast setting time, are important for children. In spite of this, many children, especially those under age 5, have difficulty tolerating impressions, even for the relatively short duration in the mouth.8 Because the alginate material flows extensively beyond the places where it is needed, it can cause gagging, excessive salivation, and in some children a perception of choking, which raises the anxiety level to exceptionally high. Alginate also can be messy and, because it gets to areas where it is not desired, create a challenging situation for cleanup afterwards.
Alternative materials have been used as "alginate substitutes" or "alginate alternatives."9 These materials have some advantages yet also provide some distinct disadvantages compared with alginate. Such alternate materials are typically made of addition silicone and are therefore relatively expensive, certainly compared with alginate. However, they do provide a fast and easy way to gain impressions, particularly for space maintainers and other appliances, that will reproduce an impression and subsequent model that is precise, accurate, and not susceptible to the distortion that sometimes occurs with alginate.9
The workflow for either alginate or alginate alternatives is the same.9 The material of choice is used for the impression, and the impression is made. After it is verified that the impression is accurate (this is at the discretion of the dentist and his or her colleagues in the practice), the impression must be poured. In many cases, the impression is wrapped in wet towels and sent to the laboratory to be poured later. The phrase "run, don't walk" regarding alginate (in terms of the time desired to pour the model) is appropriate. The longer one waits, even with a wrapped impression, the more likely the impression will become distorted. This is a problem particularly when the alginate is being used for what will become a space maintainer: if the model is distorted, it will result in an appliance that will not fit. With these materials, having to wait for the model to be poured also is problematic, and the timeline is often weeks, not days, before the appliance can be received and placed into the child's mouth. Therefore, because of these various drawbacks to using alginate or alginate alternatives, the workflow can be challenging.
Digital Workflow Methodology for Pediatric Dentistry
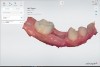
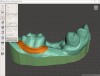
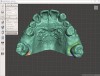
The digital workflow alternative provides many advantages over using impressions in pediatric dentistry.10 Whether for study models or appliances, the process is similar to the process for adults. The patient is situated in the chair and an explanation is given to the patient and caregivers; then the impression is made using a digital scanner (Figure 1). The scanner is then used to create a 3-dimensional (3D) color image of the case, including the surrounding soft tissues. A scanner allows the provider to "paint" the "impressed" image on the screen in the process of creating the impression. Examples of impressions for creating a space maintainer and a mouthguard are shown in Figure 2 through Figure 4.
Whereas scanning technology has improved dramatically over recent years and is likely to continue rapid improvement, it has reached the point where the speed of scanning is adequate for a young child, even perhaps one who may not tolerate a physical impression.6 In cases where the length of time to scan-although it will become shorter as technology improves-may be longer than desired, the problem can be mitigated because it is possible to scan part of the desired area and then go back and capture additional pieces of data to create the entire desired image. Even for an entire arch for study models, one does not have to perform the full scan at once without stopping. Therefore, even if it takes a little longer for a particular child than desired, scanning can be divided into separate pieces, unlike with traditional impressions. Allowing the process to be separated into different pieces is one of the most obvious advantages of digital scanning for space maintainers, study models, and other indicated uses in children.
The authors have found that digital scanning is exceptionally useful as an alternative because the time to scan is much less than the time required to perform all aspects of traditional impressions. In addition, the workflow is easier because the image can be sent to the laboratory in real time, and the appliance can be fabricated very quickly and returned to the dental office for placement in the patient's mouth much more expeditiously. This is not only desirable on the part of the patient and family, but also the provider and the dental laboratory that wants to provide the best service possible for the dental office and its patients. Dental laboratories are becoming more accustomed to digital workflow than to analog workflow.11
In addition, scanning technology, for children as well as adults, provides a more precise impression of the desired area than analog methods. There is no distortion of the image related to transport, which may happen with other impressions, and the images can be stored, transmitted, and additionally modified as desired later.12
For study models, the scanned images can be visualized in 3D form on the screen and discussed with the patient and caregivers immediately after the digital impressions are completed. The clinician does not need to wait for impressions to be poured; they can be examined immediately on the computer monitor. A conversation regarding diagnosis and treatment planning can ensue at the same visit if desired, which may not be possible when study models are needed for the conversation if they are made through physical means using analog impressions.
Finally, storage is much easier because a physical model does not need to be created and stored. If a physical model is desired later for any reason, it can be easily and quickly created using 3D printing.13 Because the information is stored digitally, all the patient information can be stored together in the health record along with any study-model digital impressions and any impressions for space maintainers and other appliances. In the event that a child were to lose or warp an appliance in the mouth, a new space maintainer or appliance could be made without the need for additional impressions in some instances.13
Figure 5 through Figure 7 show digital technology, historically used only for adults, now used in children for the fabrication of space maintainers and study models, with Figure 8 showing a completed transpalatal arch appliance. Figure 9 shows an example of a final space maintainer made via a digital workflow.
Discussion and Conclusions
One can easily see the advantages of using digital technology over standard analog impressions in pediatric dentistry, just as digital technology has advantages for adults. As the cost of scanners comes down as anticipated over the next several years, as the speed of scanning increases, and as the use of various software regimens for appliances, study models, and other needs becomes easier, the use of scanning is likely to increase in pediatric dental practices. In addition, because most dentistry for children is performed by general dentists, who refer only specialized care to the pediatric dentist, many general dentists have scanners in their office that they perhaps have not considered using for young children.14
There are some potential disadvantages as well. The cost of scanners is still relatively high, and if one does not perform many procedures using impressions, there may be no justification to purchase a scanner. However, most pediatric dental practices perform many study-model impressions and make space maintainers. It may also be argued that space maintainers might not be used as often as they should be because of the challenges of getting impressions and expeditiously placing the space maintainer. Figure 7 shows a case where a tooth was to be extracted; prior to a space maintainer being put in place, the tooth could be "extracted" on the digital model, and then a subsequent model without the tooth in place can be fabricated physically. The technician can then make a space maintainer that will adapt to the tissues when the tooth is extracted. Of course, this can be done with physical impressions as well, but the process is much faster and facilitated using digital impressions.
About the Authors
(Simon) Jen-Yih Lin, DDS, MS
Clinical Associate Professor, Department of Pediatric Dentistry, The University of Washington School of Dentistry, Seattle, Washington
Joel H. Berg, DDS, MS
Professor, Department of Pediatric Dentistry, The University of Washington School of Dentistry, Seattle, Washington
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
References
1. Goracci C, Franchi L, Vichi A, Ferrari M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: a systematic review of the clinical evidence. Eur J Orthod. 2016;38(4):422-428.
2. Aragón ML, Pontes LF, Bichara LM, et al. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: a systematic review. Eur J Orthod. 2016;38(4):429-434.
3. Grünheid T, McCarthy SD, Larson BE. Clinical use of a direct chairside oral scanner: an assessment of accuracy, time, and patient acceptance. Am J Orthod Dentofacial Orthop. 2014;146(5):673-682.
4. Kuhr F, Schmidt A, Rehmann P, Wöstmann B. A new method for assessing the accuracy of full arch impressions in patients. J Dent. 2016;55:68-74.
5. Zimmermann M, Koller C, Rumetsch M, et al. Precision of guided scanning procedures for full-arch digital impressions in vivo. J Orofac Orthop. 2017;78(6):466-471.
6. Burhardt L, Livas C, Kerdijk W, et al. Treatment comfort, time perception, and preference for conventional and digital impression techniques: a comparative study in young patients. Am J Orthod Dentofacial Orthop. 2016;150(2):261-267.
7. Sfondrini MF, Gandini P, Malfatto M, et al. Computerized casts for orthodontic purpose using powder-free intraoral scanners: accuracy, execution time, and patient feedback. Biomed Res Int. 2018; 2018:4103232.
8. Mangano A, Beretta M, Luongo G, et al. Conventional vs digital impressions: acceptability, treatment comfort and stress among young orthodontic patients. Open Dent J. 2018;12:118-124.
9. Camardella LT, Alencar DS, Breuning H, de Vasconcellos Vilella O. Effect of polyvinylsiloxane material and impression handling on the accuracy of digital models. Am J Orthod Dentofacial Orthop. 2016;149(5):
634-644.
10. Jung YR, Park JM, Chun YS, et al. Accuracy of four different digital intraoral scanners: effects of the presence of orthodontic brackets and wire. Int J Comput Dent. 2016;19(3):203-215.
11. Ender A, Zimmermann M, Attin T, Mehl A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin Oral Investig.2016;20(7):1495-1504.
12. Burzynski JA, Firestone AR, Beck FM, et al. Comparison of digital intraoral scanners and alginate impressions: time and patient satisfaction. Am J Orthod Dentofacial Orthop. 2018;153(4):534-541.
13. Wesemann C, Muallah J, Mah J, Bumann A. Accuracy and efficiency of full-arch digitalization and 3D printing: a comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017;48(1):41-50.
14. Güth JF, Runkel C, Beuer F, et al. Accuracy of five intraoral scanners compared to indirect digitalization. Clin Oral Investig. 2017;21(5):1445-1455.