You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The use of local anesthesia is essential to facilitate many procedures in the dental field. There are a variety of target sites and techniques used to achieve patient comfort. The posterior superior alveolar (PSA) block is used to achieve pulpal and soft tissue anesthesia to the maxillary third molars, second molars, as well as the first molars, with the exception of the mesiobuccal root in some cases.1-3 When the middle superior alveolar (MSA) nerve is not present, as is the case with approximately 72% of the general population, the PSA nerve innervates the mesiobuccal root of the maxillary first molar and a PSA block will provide complete pulpal and soft tissue anesthesia here as well.1-4 The PSA nerve is the target area for the PSA block injection, which requires access via the height of the mucobuccal fold just distal to the apex of the maxillary second molar. The current recommended technique for accessing the PSA nerve for an "average-sized" adult is a depth of 16mm.2,3 There is allowance for the modification for "most smaller-skulled" patients to a penetrating depth of 10-14 mm.2 Student dental professionals are taught and tested using this recommended practice in their professional programs and on national and clinical board licensing examinations.2,5 This injection technique often evokes anxiety in some clinicians as there is no osseous contact alerting the clinician that the proper depth has been reached, thus over insertion is a possibility.4 The pterygoid plexus of veins is located in this area and the inadvertent penetration of this plexus and/or nearby maxillary artery can result in unpleasant complications for the patient.
The PSA block has a 3.1% positive aspiration rate, the second highest in the oral cavity, second only to the inferior alveolar block.3 The risk of causing a large hematoma often deters clinicians from utilizing this nerve block, while instead choosing a less suitable supraperiosteal injection, requiring multiple needle penetrations to the patient. A variety of PSA techniques have been explored, including a study by Harn, SD et al. which reported seventeen variations to the PSA technique being utilized by practitioners.6 One conservative insertion technique has been suggested in the literature in an attempt to minimize these risks.2,7 Given the depth of the target area of the PSA nerve as it exits the posterior superior alveolar foramina within the infratemporal fossa, it has been theorized that a shorter needle depth is sufficient for adequate anesthetic delivery while being far enough away from the pterygoid plexus of veins and maxillary artery to avoid puncture and hematoma risk.2,4
Minimal literature exists however, to validate efficacy and hematoma risk reductions while delivering a PSA block with a reduced needle depth insertion technique. The purpose of this study was to determine if pulpal anesthesia of the maxillary second molar could be achieved using a PSA block with a reduced depth of penetration of 10 mm as compared to the standard suggested depth of 16 mm while minimizing complication risks.
Materials
This pilot study used a quasi-experimental design in which a single pre-test measurement (O1) was taken followed by an intervention (X) and finishing with a post-test measurement (O2).8 Investigators assessed whether a reduction in needle depth of the PSA block resulted in achieving pulpal anesthesia of the maxillary second molar. Since only approximately 28% of the population has an MSA nerve to innervate the mesiobuccal root of the maxillary first molar, the second molar was selected as the test tooth to be studied.1-4 Approval for this study was granted through the University of New Mexico's Institutional Review Board and the Human Research Protection Office (HRPO). Students enrolled in the undergraduate and graduate dental hygiene programs were recruited to participate. Informed consent was obtained from all participants and preliminary screening for eligibility was completed. The screening process included a review of health history, vital signs, and intraoral screening. Any participants indicating an allergy to lidocaine, blood clotting conditions, pregnant, or those taking anticoagulant medications or any type of analgesic within the last 12 hours were excluded from further participation in the study.
The intraoral screening was performed to evaluate teeth #2 and #15 to ensure they met the study criteria. Participants were immediately excluded from the study if they were missing both maxillary second molars. Each molar was assessed individually for any confounding features. Any maxillary second molar which had an amalgam, composite, crown or bridge, a root canal, an implant, frank decay or visible signs of active infection including an abscess or fistula in the maxillary molar area was not used in the study. Participants satisfying all criteria of the screening had a digital periapical radiograph of the qualified tooth taken as a final evaluation to confirm there were no radiolucent areas or visible abnormalities.
A baseline neural response was obtained using a thermal test by applying a large cotton pellet with a refrigerant, 1,1,1,2 Tetraflouroethane (Endo-ice®, Coltène/Whaledent Inc; Cuyahoga Falls, Ohio), to the middle third of the buccal surface of the tested tooth. Investigators noted either a positive or negative response to the test. After confirmation of positive response, a cotton tip applicator with 5% lidocaine topical anesthetic ointment was applied to the site of tissue penetration for 2 minutes. Participants were asked to close their mouth slightly, and shift their mandible towards the test side. They received the reduced depth PSA block using a 27-gauged, 20mm short needle, angled 45 degrees posteriorly, 45 degrees superiorly and 45 degrees medially to the point of insertion. The needle was inserted at the height of the mucobuccal fold slightly distal to the second maxillary molar and advanced to a depth of 10mm. All PSA blocks were completed either by the investigator or co-investigator. The left-handed investigator completed the PSA blocks used to test tooth #15, and was observed by the co-investigator. PSA blocks used to test tooth #2 were completed by the right-handed co-investigator and were observed by the left-handed investigator. Both investigators were present for each injection to ensure proper technique with the reduced needle depth for the PSA block was achieved.
Once it was agreed upon by the investigator/observer that the depth of 10mm had been reached at the proper angle, the investigator/operator aspirated in two planes and administered one full cartridge (~1.8 mL) of lidocaine 2% with 1:100,000 epinephrine. At 10 minutes, the thermal test was conducted again to assess the neural response of the test tooth. The same refrigerant and technique previously described was used. Investigators noted either a positive or negative response to the test for each subject with a negative response indicating pulpal anesthesia had been achieved.
Results
A total of 49 participants completed consent and enrolled in the pilot study however, after completing the screening process 6 participants were excluded as they either failed to satisfy minimum tooth requirements on tooth #2 or #15 or did not meet health history requirements. A total of 43 subjects, 39 females and 4 males, were eligible and participated in the study.
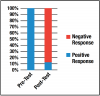
The pretest yielded a one hundred percent (n=43) "positive" baseline neural response when exposed to the refrigerant. Post-test results revealed an 88% (n=38) negative response, indicating no neural response was felt and pulpal anesthesia had been achieved on the majority of participants. This compared to 12% (n=5) of participants who still indicated a positive response on the post-test and did not achieve pulpal anesthesia. Figure 1 illustrates pre-test and post-test results of neural response of the tested teeth.
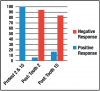
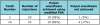
Investigators evaluated the injections administered to tooth #2 and tooth #15 individually. Twenty subjects received the modified PSA injection on tooth #2 and twenty-three subjects received it on tooth #15, resulting in a 95% and 83% negative neural response to the postthermal test, respectively. Table I and Figure 2 illustrate the results for teeth #2 and #15 individually.
A Fisher's Exact test was performed against the null hypothesis statement that there was no difference between the two groups. The test revealed (p=0.219 and α-value of 0.05) that the null hypothesis could not be rejected. A Chi-squared test was also performed and confirmed previous findings. No positive aspirations or hematoma were observed as a result of the procedure.
Discussion
Historically, it has been taught that in order to achieve profound anesthesia, the proper depth of penetration for the PSA block is 16mm.2,3 This depth of penetration is widely accepted among clinicians and educators, and is considered the measureable standard on local anesthesia clinical board examinations providing the rationale that a control was unnecessary for the purposes of this pilot study.
The traditional PSA block has a success rate of 95%.3 Complications of the PSA block are well documented in the literature and may range from local minor irritation at the injection site, trismus, or hematoma to more severe complications such as paresthesia and potential permanent eye complications.2,3,8-15 This pilot study yielded an overall success rate of 88% in achieving pulpal anesthesia on the second molar, using the reduced depth technique. Additional successes of the study included no positive aspirations and no hematomas. Results of this study indicate that more conservative injection techniques could be explored to decrease the complication risks. Perhaps clinicians would then be less fearful of causing unsightly hematomas and utilize this effective nerve block to achieve profound anesthesia.
As hypothesized, the majority of participants achieved full pulpal anesthesia with the modified technique, however lack of randomization and the convenience sample used limits the generalizability of these results to a larger population. It is also recognized that the majority of participants were women, and while still considered to have an "average" size skull, it is accepted that women generally have a smaller skull size.2-4 This could lead clinicians to think that the success rate of the reduced depth technique was influenced; however, investigators believe that results from this study provide support of the effectiveness of anesthesia through a PSA block at a reduced needle depth.
Dental practitioners routinely perform procedures such as periodontal probing, scaling and administering local anesthesia on both left and right sides of the mouth regardless of their dominant hand. In this pilot study, right- and left-handed investigators administered the PSA injection on their dominant side for purposes of providing the best viewing conditions of the needle position and depth. A study conducted by Khan et al. concluded that there was no difference in periodontal assessments based on the clinician's "handedness"16 and investigators believe the study results would have been replicated if only one investigator administered the injections on both sides of the mouth.
The limitations of a quasi-experimental pilot study are acknowledged. However, this quasi- experimental design was chosen intentionally for this pilot study to determine the logistical feasibility of conducting a larger randomized, blinded clinical study.
Conclusion
The reduced needle depth technique showed promise in achieving desired results of pulpal anesthesia coupled with decreasing risk and complications. Additional randomized, controlled, blinded clinical studies are recommended to achieve evidence-based support for the academic and dental communities to assess replacing the current recommended PSA block technique with the modified PSA block with a reduced needle depth.
Acknowledgements
Authors wish to thank Demetra Logothetis, RDH, MS and Margaret Fehrenbach, RDH, MS for providing the anatomical background and local anesthesia expertise, which lead to the investigation of this technique.
About the Authors
Diana B. Aboytes, RDH, MS is an assistant professor; Vicki G. Pizanis, RDH, MS, EdD is a member of the adjunct faculty; both in the Department of Dental Medicine at the University of New Mexico, Albuquerque, NM.
Corresponding author: Diana B. Aboytes, RDH, MS; DAboytes@salud.unm.edu
References
1. Loetscher CA, Melton DC, Walton RE. Injection regimen for anesthesia of the maxillary first molar. J Am Dent Assoc. 1988 Aug;117(2):337-40.
2. Logothetis D. Local anesthesia for the dental hygienist. 2nd ed. Missouri: Elsevier; c2017. 363 p.
3. Malamed SF. Handbook of Local Anesthesia. 6th ed. Missouri: Elsevier Mosby; c2013. 409 p.
4. Fehrenbach MJ, Herring SW. Illustrated Anatomy of the Head and Neck. 5th ed. Missouri: Elsevier Saunders; c2016. 331 p.
5. Darby M, Walsh M. Dental hygiene theory and practice. 3rd ed. Missouri: Elsevier Saunders; c2010. 1176 p.
6. Harn SD, Durham TM, Callahan BP, Kent DK. The triangle of safety: a modified posterior superior alveolar injection technique based on the anatomy of the PSA artery. Gen Dent. 2002 Nov-Dec;50(6):554-7.
7. Logothetis D, Fehrenbach MJ. Local anesthesia for the dental hygienist. 2nd ed. Missouri: Elsevier; c2017. Chapter 12, Maxillary anesthesia; p. 222.
8. Harris A, McGregor J, Perencevich E, Furuno J, et al. The use and interpretation of quasiexperimental studies in medical informatics. J Am Med Inform Assoc. 2006 Jan; 13(1):16-23.
9. Prakasm M, Managutti A, Dolas RS, Agrawal MG. Temporary pupillary dilatation and ptosis: complications of PSA nerve block: a case report and review of literature. J Maxillofac Oral Surg. 2009 Jun;8(2):181-3.
10. Goldberg AS. Transient diplopia as a result of block injections. Mandibular and posterior superior alveolar. N Y State Dent J. 1997 May;63(5):29-31.
11. Peñarrocha-Diago M, Sanchis-Bielsa JM. Ophthalmologic complications after intraoral local anesthesia with articaine. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000 Jul;90(1):21-4.
12. Shaner JW, Saini TS, Kimmes NS, Norton NS, et al. Transitory paresis of the lateral pterygoid muscle during a posterior superior alveolar nerve block-a case report. Gen Dent. 2007 Nov-Dec;55(6):532-6.
13. McNicholas S, Torabinejad M. Esotropia following posterior superior alveolar nerve block. J Calif Dent Assoc. 1992 Sep;20(9):33-4.
14. Kim WK. Diplopia and inferior rectus muscle palsy after posterior superior alveolar nerve block. J Korean Assoc Maxillofac Plast Reconstr Surg. 2001;23(5):461-70.
15. Marinho RO. Abducent nerve palsy following dental local analgesia. Br Dent J. 1995 Jul;179(2):69-70.
16. Khan SM, Blanchard SB, Dowsett SA, Eckert GJ, Kowolik, MJ. Periodontal assessment by right- and left-handed examiners: is there a difference? J Periodontol. 2006 Jul;77(7):1099-103.