You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Biases, even those that are unintentional, inhibit impartial judgment. Further complicating the ability to make correct decisions is the way in which memories are stored and maintained. The human brain does not act like a computer, storing memories in digital binary code. Rather, memories are altered each time the brain accesses them. Take, for example, the last recall patient of the day, who had a failing root canal and a successful implant side-byside. That experience would alter the clinician's overall memory and personal bias regarding the predictability of success of implants versus endodontics. The tendency in mainstream dentistry to perform endodontics without the constant and consistent use of an operating microscope is also a significant problem. What cannot be seen cannot be critically analyzed, and the inside of a tooth cannot be seen without a microscope.
This article will provide a brief overview of the problem, highlight examples, offer take-home solutions and/or a game plan that can be implemented immediately to acquire the information, training, and instruments to create real change.
For this article's purposes, endodontic biases will be grouped into four types: anatomy, instruments, shaping, and outcomes/ predictability. The sequence of these biases is relevant. The anatomy is unyielding and all other endodontic components, ie instruments, shaping strategies, etc, must acquiesce to the individual anatomy of the tooth.
Anatomic Bias
All dental clinicians could benefit from regular continuing education that focuses on anatomy. Endodontic, occlusal, periodontal, and even esthetic problems often have anatomic considerations that go unnoticed and unsolved. Some stylized or oversimplified educational materials can actually exacerbate the problem with illustrations depicting unrealistic or downright flawed anatomy.
Anatomic Bias I
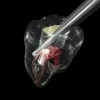
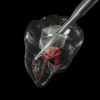
Figure 1 shows a radiograph of a typical maxillary first molar. Upon extraction, the apical anatomy was immediately studied and photographed under a global microscope ( Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6). That is a take-home lesson; the extracted teeth should be studied with loupes or microscopes. These photographs demonstrate an important lesson. The two-dimensional radiograph shows three roots. In reality, however, a significant percentage of maxillary first and third molars—80% in some studies—have four roots and four or more canals. 1,2 While the MB and MP (MB-2) roots are usually fused, their morphology is unique. For diagnostic, access, and shaping purposes, it is safer to think of them as separate roots. Wisdom teeth often exaggerate the anatomic features of first and second molars, and a significant percentage of maxillary third molars have four distinct roots. The author's personal bias is to consider most maxillary first the radiographic apex of the tooth. The use of the radiographic root apex for use as the reference point for measuring the apical extent of the root filling is the common standard, yet has been criticized because of the poor correlation between the location of this point and the actual canal foramen. 5 The illustrations used in advertising and manufacturer's "tip cards" only further the notion of simple foramen anatomy. While simple anatomy is often the case with incisor teeth, a quick perusal of the posterior teeth in Brown and Herbransen's Dental Anatomy & 3D Interactive Tooth Atlas demonstrates that a significant portion of the foramen exit short of the apex and have multiple foramina. 6 The same extracted tooth in Figure 2 demonstrates that the palatal foramen is more than a millimeter short of the radiographic apex. If this tooth were filled to the constriction, which for arguments sake is 0.75 mm from the foramen, a straight-on radiograph would depict the fill as being at least 2 mm "short."
Anatomic Bias III: Apical Constriction
The constriction can be found as far as 3 mm from the foramen, which would mean that the correct fill in this example would be 4 mm "short" of the radiographic apex. 7 Anatomic biases II and III can be confronted with the use of an apex-locating device. Several recently published studies discuss the accuracy of electronic apex locators. 8,9 Many of the current generation of electronics apex locators provide very accurate readings, and the manufacturers claim the device measures the constriction as opposed to the periodontal ligament. 10 The author has tested newer models that claim to measure to the constriction and found that they sometimes do indeed give slightly shorter readings than other apex locators, which would support the manufacturer's claims. For vital (nonlesion) cases in which consistent and repeated apex locator readings agree with other factors, the author is now filling shorter in some roots than in the past. Slight overfills of vital cases do not make sense from a histological standpoint. It is interesting to note that when the author lectures at and attends European endodontic meetings, the Europeans often ask why North American clinicians routinely overfill. The bias in North America seems to have shifted apically over the past 50 years.
Anatomic Bias IV: Radiographic Canal Obliteration
When a tooth appears completely calcified on the radiograph, it is often assumed there is no pulp tissue in that portion of the tooth. Evaluating the research reveals that this bias is unfounded. 11-13 Although radiographs may reveal what appears to be a total obliteration of the pulp canal, there generally remains clinical evidence of a pulp canal and pulpal tissue. 14-16 It is crucial to eliminate this bias, due to the errors and gouging that follow such a flawed mental model.
Anatomic Bias Summary and Clinical Recommendations
The goal in vital (non-lesion) cases should be to fill to the anatomic constriction, not necessarily to the radiographic apex. Overfilling a vital (non-lesion) case is unacceptable. Taking a holistic, three-dimensional, anatomically enlightened approach using multiple measuring disciplines is recommended. For infected (lesion) cases, it may be safer to fill to the radiographic apex, understanding that using the arbitrary radiographic apex position assures that more of the root is cleaned and shaped, but will result in many actual anatomic overfills. Some will be fairly significant overfills. Anatomy in ovoid roots can be far more complex than the radiograph shows, and many teeth have more roots and more canal systems than is commonly assumed. Vertucci has classified eight separate canal patterns that can be found in an ovoid root with up to three separate canals and various anastomosing patterns. 14 Gulabivala added an additional five patterns to Vertucci's eight, including four separate canals in the one root. 15
Instrument and Shaping Bias
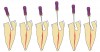
Round burs have long been the bur of choice when accessing beyond the initial cavosurface access of the tooth. Because of the rounded end, round burs seem safer than other burs. The round bur is also the most commonly used for accessing and subsequently exploring the calcified tooth in pursuit of a tiny wisp of pulp. Clinicians' bias toward this bur stems from a combination of factors, but is based mostly on habit. There is a universal misconception that round burs in a latch grip cut slowly and safely, but neither is the case. The radiograph in Figure 7 shows the dangerous gouging that is common with both a round bur and the parallel-sided tunnel that a round bur eventually creates. Rather, a conical shape is preferred. In the hands of a skilled clinician, the conical shape is possible to cut with a series of decreasing diameter round burs, but an uphill battle must be waged against the cutting action of round burs. With the advent of modern bur shapes, this exceedingly difficult and dangerous task is no longer necessary ( Figure 8 and Figure 9). Conical-shaped burs allow the clinician to work with the bur to create the ideal access shape. A secondary benefit is that one or two conical carbide burs can replace seven or more traditional burs, such as multiple round burs and Gates-Glidden burs, for instance.
Round burs have three inherent problems. Tip size is the first issue ( Figure 10). The tips are simply too big. The second problem is shape. The resultant irregular and parallel-sided cavity walls formed by a round bur work against the clinician when attempting to insert a hand file. When clinicians rummage around the calcified tooth with a round bur, it is common for the bur to become slightly misdirected. Then when inserting a file, it clunks into the bottom of the "well." The clinician has no choice but to continue to tunnel deeper and go back and forth, clunking hand files into the fruitless bottom and then burrowing deeper with round burs. In most cases, the wisp of pulp was higher up, like a trap door on the side wall ( Figure 11).
The third problem with round The third problem with round burs is their tendency to gouge during de-roofing. Khademi maintains that it is truly impossible to cut flat walls in three dimensions with a round (round bur) instrument. 16 What happens instead is that the chamber is not unroofed in some areas, which leaves pulpal and necrotic debris, with no specific subsequent step to address the debris. Yet the walls are overextended and gouged in other areas. Further, the internal radius of curvature at many of the pulp chamber line angles is simply too small for all but the smallest of round burs.
In the final analysis, round burs point cut in an endodontic access application, but planing is necessary. A new set of mental models based on vision is needed, along with a new set of instruments that are reflective of the task at hand and the desired shaping outcomes. The new vision-based mental model is "Look, Groom, Follow." The new burs are all rounded, ended tapers. Round burs tend to cut predictable shaping patterns that do not help the doctor or the tooth. 17
When a machined, smooth, and conical-shaped preparation is cut with conical carbide, the visual contrast between dentin and pulp tissue remnants (PTRs) is visually apparent and tactilely accessible ( Figure 12). Microsurgeon dentists operating at 8x to 24x magnification with an operating microscope can leverage the optimized dentinal maps for direct visual recognition of tiny PTR s, even when the smallest hand file does not bind. Endodontists and dentists who elect to perform endodontics without microscopes benefit from the tactile advantage of the conical shape. In either case, the patient can benefit, because minimized gouging allows peri-cervical dentin (PCD) to be maintained. PCD is defined as the crucial dentin in the "neck of the tooth," from 4 mm coronal to crestal bone to 4 mm apical to crestal bone.
Case Report
The feature case of this article, highlighted in Figure 13 through Figure 24, demonstrates a comprehensive shift in many aspects of endodontic access. The calcified central incisor ( Figure 13) of a 42-year-old woman was treatment planned for elective endodontics to facilitate internal bleaching for esthetic reasons. The preoperative radiograph demonstrated almost complete obliteration of the pulp, except for a small pouch in the center of the root. Referring these challenging cases to a microscopeequipped endodontist should always be considered. However, many well-trained general dentists attempt these difficult cases, and most dentists routinely deal with partially calcified cases. Still, the concepts forwarded in this case can be employed as indicated in every endodontic access treatment.
Single-tooth isolation does not give the clinician a good 3-dimensional feel for root anatomy and angulation. The problem is further compounded when there is a full crown present and the original anatomic landmarks are gone. The clamp can also impede handpiece orientation, which further steers the clinician astray. Additionally, the clamp blocks x-ray passage if the clinician chooses to pause and take a radiograph for access location and direction verification. Endodontists often report that they remove the rubber dam entirely for difficult calcified cases. This enables the clinician to develop a better feel for the three-dimensional procedure of canal discovery, and then replace the dam once the canal systems are safely discovered. The author finds that the quadrant dam offers the best of both worlds ( Figure 14).
The first step in the access for the calcified tooth is the establishment of the palatal–incisal notch ( Figure 15 and Figure 16). Once the area where the original pulp chamber was located has been accessed, it is advisable to take an orientation verification radiograph or multiple angled radiographs ( Figure 17). The palatal–incisal notch works in concert with the narrow shaft of the bur to perform important tasks. Similar to a surgical stint for implant drilling, the notch first stabilizes and directs the head of the bur by cradling the shaft. Secondly, it allows a more appropriate angulation—toward the incisal—of the back of the bur. Anatomy lessons have taught clinicians that the root and the crown of incisors are not parallel.
The resultant cavosurface outline is quite long and fairly narrow for the calcified tooth, and creates better potential for accuracy ( Figure 18 and Figure 19). A final view of the access in Figure 20 shows the orientation of the palatal–incisal notch and the dentinal map, which is encountered as early as possible. The radiographic sequence ( Figure 21, Figure 22, Figure 23 and Figure 24) teaches a new concept in accessing calcified canals, that of radiographs taken using the pointing quality of a conical bur to assess direction and position of the access cavity. Corrective steps can then be taken to avoid gouging or perforation. In the past, only endodontic files have been used as metallic (radiopaque) radiographic markers. The snug fit of a conical bur as opposed to the loose fit of a round bur facilitates the use of the bur in taking "bur instrument films."
The old bias of horizontal primary access that intersects the dentinal map in the middle of the crown deprives the clinician of this incredibly useful and important landmark, that of the old pulp horn. Additionally, the old bias requires a 90° turn from horizontal to vertical, which invariably leads to facial gouging and other more subtle problems. Each step of the access should lay a foundation for success and prevention of gouging. There are five critical biases and the accompanying changed access principles demonstrated in the feature case, which are outlined in Table 1.
Bias Summary
In restorative dentistry, the fissurotomy bur, air abrasion, hard tissue lasers, and other modern cutting modalities allow occlusal defects and occlusal caries to be accessed with significantly less tooth removal than the old-fashioned but widely popular flat-ended fissure bur. Thankfully, a good percentage of restorative dentists and dental schools have embraced this move toward minimally invasive preparation design; a design that was once only possible or practical with new armamentarium and new filling materials. In contrast, endodontic access shapes have recently become more aggressive and potentially more iatrogenic, while restorative dentistry has trended toward the minimally invasive. For many endodontic camps, changing biases will happen slowly or not at all. Nevertheless, pressure from restorative dentists will eventually drive endodontic access and shaping toward conservatism, with the secondary benefit of expediency.
Outcomes/Predictability Bias
Endodontic success/failure rates and comparisons to implant success/failure rates is currently a hot topic. Endodontic outcome study results are so diverse that it is difficult to obtain a general sense of predictability. Is endodontics 95% successful, or only 75% successful? If it is only 75% successful, then the implantologists are right, and implants are certainly a better option. As the gatekeepers, restorative dentists are obligated to fully understand whether implants or endodontics are truly in the patient's best interest. Interpreting endodontic outcome studies is incredibly complicated. Variables include tooth type (singlerooted or multi-rooted), sample size, and case selection. Treatment options are variable, and providers, techniques, culturing, and the subsequent restoration are all factors with a strong influence. The methodology of the studies is critical, and these factors include the study design, recall rate, radiographic interpretation, follow-up period and, finally, analysis. Outcome studies used by the American Association of Endodontists and other endodontic advocates often differ from those of implantologists, as they engage in healthy skirmishes over dental turf.
In the final analysis, comparing outcome studies is almost pointless. Putting a blanket success or failure number on all different types of endodontic cases just perpetuates unfounded biases. Gaining an understanding of the differences between variables within the major studies can be more insightful ( Table 2). 18-20
In reality, there are two types of endodontics: those with biofilm and without biofilm. The failure rate of infected (lesion) cases is at least three times higher than non-infected (non-lesion) cases. Non-biofilm cases are more like a deep pulp cap. Biofilm cases, on the other hand, are fraught with peril. Therefore, good endodontics performed on pulpitic (non-lesion, non-infected) cases with good restorative work should be 98% successful. Contrast that with the outcomes of poor endodontics combined with poor restorative work on a mix of lesion and non-lesion cases, where the failure rate is nearly 50% ( Table 2).
Take-Home Outcome Tips
Patients should be interviewed at each recall, and asked if they have any sensitive teeth. Teeth with crowns, a history of trauma, or deep fillings should be considered extremely high-risk if the patient has recently experienced sensitivity after a symptom-free period. After ruling out other causative problems such as cervical abrasions, sinusitis, stress, and bruxism, endodontics should be done before the tooth becomes necrotic.
Necrotic cases should be referred to an endodontist if the general dentist does not have the stomach for failures. The author now discusses implants when treatment planning endodontics for necrotic cases. Patients need to understand their odds and their option, although the author encourages his patients to choose endodontics over implants in higher-risk lesion cases once they understand the odds. Regardless, an extraction should instead be performed if the patient cannot afford endodontics and a good build-up and composite onlay (in the case where a crown will need to be delayed for posterior teeth). A "cotton and Cavit" temporary restoration that leads to failure and extraction blackens the eye of endodontics.
References
1. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod. 1999;25(6):446-450.
2. Somma F, Leoni D, Plotino G, et al. Root canal morphology of the mesiobuccal root of maxillary first molars: a micro-computed tomographic analysis. Int Endod J. 2009;42(2):165-174.
3. Al-N azhan S. Incidence of four canals in root-canal-treated mandibular first molars in a Saudi Arabian sub-population. Int Endod J. 1999;32(1):49-52.
4. Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population—a clinical study. Int Endod J. 2008;41(9):755-762.
5. Mizutani T. Ohno N, Nakamura H. Anatomical study of the root apex in the maxillary anterior teeth. J Endod. 1992:18;344-347.
6. Brown P, Herbranson E, eds. Dental Anatomy & 3D Interactive Tooth Atlas. Quintessence Pub Co; 2007.
7. Hassanin EE , Hashem A, Chalfin H. Histomorphometric study of the root apex of mandibular premolar teeth: an attempt to correlate working length measured with electronic and radiograph methods to various anatomic positions in the apical portion of the canal. J Endod. 2008;34(4):408-412.
8. Cianconi L, Angotti V, Felici R, et al. Accuracy of three electronic apex locators compared with digital radiography: an ex vivo study. J Endod. 2010;36(12):2003-2007.
9. Ravanshad S, Adl A, Anvar J. Effect of working length measurement by electronic apex locator or radiography on the adequacy of final working length: a randomized clinical trial. J Endod. 2010;36(11):1753-1756.
10. Nguyen HQ, Kaufman AY, Komorowski RC, Friedman S. Electronic length measurement using small and large files in enlarged canals. Int Endod J. 1996;29(6):359-364.
11. Haywood VB, DiAngelis AJ. Bleaching the single dark tooth. Inside Dentistry. 2010;6(8):42-52.
12. Piatelli A. Generalized "complete" calcific degeneration or pulp obliteration. Endod Dent Traumatol. 1992;8:259-263.
13. Kuyk JK, Walton RE . Comparison of the radiographic appearance of root canal size to its actual diameter. J Endod. 1990;16(11):528-533.
14. Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc. 1978;97(1):47-50.
15. Alavi AM, Opasanon A, Ng YL, Gulabivala K. Root and canal morphology of Thai maxillary molars. Int Endod J. 2002;35(5):478-485.
16. Clark D, Khademi JA. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010;54(2):249-273
.17. Clark D, Khademi JA. Case studies in modern molar access and directed dentin conservation. Dent Clin North Am. 2010;54(2):275-289.
18. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997;30(5):297-306.
19. Friedman S, Abitbol S, Lawrence HP. Treatment outcome in endodontics: the Toronto Study. Phase 1: initial treatment. J Endod. 2003;29(12):787-793.
20. Sunde PT, Olsen I, Debelian GJ, Tronstad L. Microbiota of periapical lesions refractory to endodontic therapy. J Endod. 2002;28(4):304-310.
About the Author
David Clark, DDS
Private Practice
Tacoma, Washington