You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
In 2014, Americans were one and a half times more likely to die from an opioid overdose than from a motor vehicle crash.1 The ongoing misuse and abuse of highly addictive prescription opioids has led to a public health crisis in the United States. Since 2000, there has been a 200% increase in opioid overdose deaths due to prescription opioid analgesics and heroin. In 2014, 61% of drug overdose deaths were attributable solely to opioids.1 In 2016, healthcare providers wrote more than 214 million prescriptions for opioid pain medication, a rate of 66.5 prescriptions per 100 people. In 2018, the government declared a public health emergency and allocated part of a $1.3 trillion spending bill to combat the opioid addiction epidemic, which is estimated to have a total economic burden of $78.5 billion per year, including the costs of healthcare, lost productivity, addiction treatment, and criminal justice involvement.2
The Opioid Epidemic
The factors contributing to this crisis are varied, although the beginning of the epidemic can be traced to OxyContin®, a sustained-release formulation of oxycodone manufactured by Purdue Pharma,3 a drug that was not commonly prescribed by dental professionals. Ag-gressive marketing of opioid pain medications promoting their effectiveness while de-emphasizing their addictive potential was a major contributor to overprescribing by clinicians.
In 2001, the Joint Commission's Pain Management Standards led to the popularization of pain as "the 5th vital sign," and what followed were efforts to treat acute pain as aggressively as possible.4 Some providers may have had noble intentions to prevent any pain or discomfort for patients, but they may have overestimated the magnitude of patients' postoperative pain; others cited concerns for patient satisfaction and online practice reviews as justification for their prescribing practices.4 Nevertheless, these ensuing prescribing practices contributed to an increase in opioid exposure and an increased amount of leftover medication that could be misused, abused, or diverted to others.5
Efforts are currently under way to minimize the use of opioid analgesics for acute pain.6 Many major opioid distributors and manufacturers now face criminal investigation from dozens of states, cities, and counties with regard to their misrepresentation of the safety and efficacy of opioids. In addition to the culture of overprescribing, other factors contributing to the epidemic include "doctor shopping" and prescription fraud.
Opioid Prescribing Practices in Dentistry
Dental prescribers are unique because the management of acute postoperative pain is a central component of their practices. In 2012, dentists prescribed 6.4% of the total opioid prescriptions in the United States, second just to primary care physicians.7,8 Although dentists do not account for the largest number of prescriptions, they are the top prescriber of opioids for adolescents.9 Dentists were reported to write approximately 31% of their immediate-release opioid analgesic prescriptions (acetaminophen plus codeine, hydrocodone, or oxycodone) for youth aged 10 to 19 years, ages when dental surgery for third-molar removal is prevalent.10 It has been estimated that there are approximately 5 million individuals, mostly young adults and adolescents, in the United States who undergo wisdom tooth extraction surgery annually.11 The overprescribing of opioids has significant implications for the developing adolescent brain. It has been shown that the prefrontal cortex is not completely developed until age 20 to 25 years.12 A recent study found that legitimate opioid use before high school graduation is independently associated with a 33% increase in the risk of future opioid misuse after high school.13
In a cross-sectional study of prescriptions for opioids in 2016, dentists in the United States were found to have prescribed 37 times the amount of opioids as dentists in England.14 The amount of prescription opioids peaked in 2010 at 782 morphine milligram equivalents (MME) per patient.15 Different opioids have different potencies, or the dose needed to produce a given effect or response. Oral medications such as oxycodone 5 mg, hydrocodone 10 mg, and codeine 60 mg are all equivalent to oral morphine 10 mg, or are said to be equal to 10 MME. The comparison of MMEs adjusts for the potencies of different opioids. Although prescription rates have since been declining, it was observed that for individuals with private health insurance, the number of opioids prescribed by dentists increased from 2010 to 2015, with the greatest increase in prescriptions, as well as dosage, for adolescents aged 11 to 18 years.7,16
Aside from ambulatory care visits in dental offices, emergency departments (EDs) function as a venue for the receipt of opioid prescriptions for nontraumatic dental conditions (NTDCs) from physicians who are not familiar with the diagnosis and management of dental pain.17 Among adolescents and young adults who visited EDs in 2005 and 2015, opioids were prescribed for NTDCs at a rate of 59.7% and 57.9% per visit, respectively.17 These numbers are significant because teens exposed to oral opioids may be at increased risk of subsequent fentanyl and heroin use.18 It has been estimated that one in eight deaths in teens and young adults is linked to opioids.17
In dentistry, the most commonly prescribed immediate-release opioid formulation is acetaminophen with hydrocodone bitartrate for surgical dental visits; formulations with codeine and oxycodone are also prescribed frequently.5 On average, 20 opioid pills are prescribed after dental extractions; however, less than half of opioids prescribed after surgical extractions are used.5 The unused medications may lead to sharing and misuse of these medications for nonmedical purposes. Alarmingly, one-third of the opioid prescriptions are for nonsurgical dental visits.5,7,19
Changing Guidelines and Regulations
The recent decline in opioid prescribing is due to a combination of state legislation, federal laws, Centers for Disease Control and Prevention (CDC) reports, professional medical and dental organizations, continuing education, and prescription drug monitoring programs (PDMPs).20,21 PDMPs are tasked with collecting information about prescription data on controlled substances, with the goal of reducing prescription drug abuse and identifying patients who are on excessive doses or dangerous combinations of Drug Enforcement Administration scheduled drugs.22 Although they can be time-consuming for the provider, these programs are valuable in that they enable clinicians to identify patients with a history of drug-seeking behavior or a history of legitimate prescriptions for other opioids, benzodiazepines, or barbiturates that, if taken with an additional opioid prescription, may result in potentially lethal respiratory depression. Recent studies have shown that mandatory PDMPs caused a 78% reduction in the quantity of opioids prescribed and an increase in prescriptions for non-opioid analgesics.23 In New York State, a mandatory PDMP was instituted in 2014. It led to a significant decrease in doctor shopping. One study showed a 78% reduction in the quantity of opioid pills prescribed in a dental urgent care center.23 Currently all states except Missouri have a mandatory PDMP.
In 2016, the American Dental Association revised its statement on the use of opioids in the treatment of dental pain.24 The revision states: "Dentists should consider nonsteroidal anti-inflammatory analgesics as the first-line therapy for acute pain management." Although the official policy has changed, studies have shown that clinical practice guidelines are not effective in promoting behavioral change among healthcare professionals.25 Bolstering the guidelines with mandatory continuing education has proven a vital and important means of improving provider knowledge and competency in opioid prescription management.21 In addition, significant efforts in dental schools toward educating new generations of providers have been implemented, including curriculum and clinical protocol changes.26
The Evidence Supports a Multimodal Analgesic Approach for Prescribing Analgesics for Postoperative Dental Pain
Multimodal analgesia is a term that has received increased attention due to the opioid crisis. It means to intercept pain at multiple areas along the peripheral and central pain pathways, resulting in an additive analgesic effect while reducing the doses and side effects of each drug class utilized. It is an opioid-sparing strategy that at most can result in prescriptions for a 2- to 3-day course of opioids, as opposed to prescribing as many as 30 pills.27 Dentists who render an area anesthetized with local anesthetic and then prescribe postoperative oral analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and opioids are already using multimodal analgesic regimens.27-29
Despite their over-the-counter (OTC) status, NSAIDs and acetaminophen can provide at least equal, if not superior, analgesia to that of opioids for dental pain after removal of impacted third molars.27,28 The role of opioids in managing severe acute postoperative dental pain is limited. First-line treatments include profound long-acting postoperative local anesthesia, NSAIDs, and acetaminophen. Each of these drug classes have their own indications, contraindications, adverse effects, and drug-drug interactions of which the dental provider must be aware. A detailed discussion on the pharmacology of local anesthetics, NSAIDs, and acetaminophen is outside of the scope of this article.
Figure 1 illustrates the stepwise manner for prescribing analgesics for acute postoperative dental pain.27,28 Ibuprofen is the first-line drug for moderate to severe postoperative dental pain. For mild pain, ibuprofen 200 to 400 mg can be taken on an as-needed-for-pain basis every 6 hours. As the pain escalates to mild to moderate pain, ibuprofen 400 mg can be taken on a fixed interval (around the clock) every 4 hours for the first 24 hours, followed by ibuprofen 400 mg every 4 hours on an as-needed basis. For moderate to severe pain, ibuprofen 400 mg plus acetaminophen 500 mg would be taken on a fixed interval every 6 hours for the first 48 hours, followed by ibuprofen 400 mg every 4 hours as needed. For severe pain, ibuprofen 400 mg plus an acetaminophen 650 mg plus hydrocodone 10 mg combination would be taken every 6 hours on a fixed basis for 48 hours, followed by ibuprofen 400 mg and acetaminophen 500 mg every 4 hours as needed.
The maximum daily dose for ibuprofen should not exceed 2400 mg, and the maximum recommended daily dose of acetaminophen should not exceed 4000 mg.27,28 The maximum recommended daily dose of Tylenol® (McNeil Consumer Healthcare Division of Johnson & Johnson), the brand-name formulation of acetaminophen, is 3000 mg. Medical literature supports the safety of the maximum recommended daily dose of acetaminophen at 4000 mg for a short period. The manufacturers voluntarily reduced the maximum recommended dose because there are many combination drug products that contain acetaminophen, including not only opioid-acetaminophen combination prescription drugs but also OTC cold and cough medications. The concern was that an overdose and hepatotoxicity would occur if an individual were unknowingly taking several acetaminophen-containing products.30 Dentists should query patients about their intake of such products and educate them about the potential dangers of using multiple products that contain acetaminophen.
If NSAIDs are contraindicated, the first-line medication becomes acetaminophen. Acetaminophen is synonymous with paracetamol and N-acetyl-para-aminophenol, abbreviated as APAP. For mild pain, acetaminophen 650 to 1000 mg can be taken every 6 hours on an as-needed-for-pain basis. The reason for many published guidelines stating 650 to 1000 mg of acetaminophen is that the available formulations of acetaminophen include 325 mg and 500 mg tablets, so two tablets would be 650 mg or 1000 mg, respectively. Additionally, because the maximum recommended dose for generic acetaminophen is 4 g (4000 mg) per day, dosing of 1000 mg every 6 hours would be the maximum dose. For moderate pain, acetaminophen 650 mg plus hydrocodone 10 mg can be taken every 6 hours for a fixed interval for 24 hours. Then, acetaminophen 650 to 1000 mg can be taken every 6 hours on an as-needed-for-pain basis. For patients who cannot tolerate NSAIDs and are experiencing severe pain, acetaminophen 650 mg plus hydrocodone 10 mg can be taken every 6 hours for a fixed interval for 48 hours. Then, acetaminophen 650 to 1000 mg can be taken every 6 hours on an as-needed-for-pain basis. The maximum daily dose of acetaminophen should not exceed 4000 mg.28
Other strategies to reduce pain include preemptive analgesia and postoperative long-acting local anesthetics. Preemptive analgesia means taking analgesics before the start of the procedure or postoperatively before pain has arisen. Postoperative pain is driven by a variety of inflammatory mediators, including prostaglandins. Administering ibuprofen before an incision will limit the production of prostaglandins from the outset rather than after a procedure-or if taken immediately after surgery, before the effects of the local anesthetic have dissipated. The preemptive administration is practical because the patient may have limited ability to eat or take oral medications postoperatively.31,32
The administration of the long-acting local anesthetic 0.5% bupivacaine plus 1:200,000 epinephrine at the end of a procedure can reduce pain scores for up to 48 hours postoperatively. A reduction in postoperative pain will result in less analgesic consumption, fewer drug-specific side effects, and potentially less exposure to opioids. In a study by Gordon et al of patients who had their third molars removed under general anesthesia, pain scores were reduced for 48 hours if the long-acting local anesthetic solution of 0.5% bupivacaine plus 1:200,000 epinephrine was administered immediately postoperatively compared with patients who were not given this regimen (Figure 2).33 It is thought that the long-acting bupivacaine reduces the afferent barrage of nociceptive input and prevents central sensitization to pain; the benefit of long-acting local anesthetic is still significant at 48 hours even though the local anesthetic will have worn off.27-29
Liposomal bupivacaine injectable suspension (Exparel®, Pacira BioSciences) is a long-acting local anesthetic formulation that was granted Food and Drug Administration (FDA) approval in 2011.34 This local anesthetic is indicated for postsurgical analgesia by local (infiltration) administration to the surgical site.34,35 It is not indicated as a replacement for preoperative local anesthesia.34,35 It is formulated as a multivesicular liposomal formulation with lipid bilayers arranged like a honeycomb, with the bupivacaine in the aqueous core, that slowly releases the bupivacaine over time.34,35 Liposomal bupivacaine can persist for 96 hours after administration, which makes it a valuable tool in keeping patients numb and comfortable in the 2- to 3-day window of postoperative pain and inflammation after removal of impacted third molars.34,35 A thorough discussion of liposomal bupivacaine injectable suspension is beyond the scope of this paper.
The use of liposomal bupivacaine may be cost prohibitive at approximately $175 for a single-use, single-patient vial of 133 mg/10 mL or $325 for a single-use, single-patient vial of 266 mg/20 mL.35 However, studies suggest that infiltration with an appropriate volume of traditional bupivacaine to cover the surgical site may be equally effective in reducing pain scores.36 A prospective, randomized, double-blinded trial comparing pain scores, analgesic consumption, and soft-tissue numbness in patients with untreated, symptomatic, irreversible pulpitis with either 4 mL liposomal or 4 mL traditional bupivacaine plus 1:200,000 epinephrine supports the use of traditional bupivacaine for postoperative pain control.36 The patients had no significant differences in the amount of pain and analgesic consumption for 3 days after the injections but did report more soft-tissue numbness with the liposomal formulation.36
Another prospective, randomized, double-blind trial compared liposomal and regular bupivacaine, also 4 mL each, on symptomatic, necrotic teeth after endodontic debridement.37 The patients were followed for 5 days postoperatively to assess pain, soft-tissue anesthesia, the use of opioid rescue medication, and the use of non-opioid analgesics.37 Success was defined as patients not using an opioid and reporting no pain or mild pain.37 The success rate was statistically similar for both groups, 29% for liposomal bupivacaine and 22% for bupivacaine.37 It is notable that there was no statistical difference in the use of rescue medication (opioids) in either group.37 A study of patients after dental impaction surgery showed only modest benefits for those treated with liposomal bupivacaine over those receiving placebo postoperatively.38 Further research is needed to explore the utility of liposomal bupivacaine after traumatic dental procedures.
Future research exploring the risk-benefit ratio of glucocorticoids and the selective cyclooxygenase-2 (COX-2) inhibitor celecoxib also appears warranted. Glucocorticoids work by inhibiting phospholipase A2, the enzyme responsible for the release of arachidonic acid from damaged cell membranes, therefore preventing the synthesis of prostaglandins and leukotrienes.39 Data support the reduction of early and late edema as well as early trismus after third-molar extraction when steroids are injected submucosally.40
NSAIDs are highly efficacious medications for acute postoperative dental pain because such pain is of an inflammatory nature, but the side-effect profile may preclude use in patients with gastrointestinal ulcers, perforations, and bleeds, or those with coagulopathies. NSAIDs interfere with both COX-1 and COX-2 enzymes. COX-2 inhibitors, as their name implies, block COX-2 selectively and possess lower ulcerogenic and bleeding effects than non-selective NSAIDs such as ibuprofen and naproxen sodium.39 However, COX-2 inhibitors such as celecoxib have been associated with an increased risk of heart attacks and strokes, at least when taken chronically. That factor prompted the drug manufacturer Merck to remove rofecoxib (Vioxx®) from the market. Subsequently the FDA also removed the highly selective COX-2 inhibitor valdecoxib. Moreover, the FDA issued its most serious warning, a black box warning, on all NSAIDs, including those available OTC and celecoxib.41,42 One double-blinded study evaluated the analgesic efficacy of diclofenac 50 mg, acetaminophen 1000 mg, celecoxib 400 mg, and placebo and found that all treatment groups were superior to placebo, and that celecoxib was as effective as diclofenac for postoperative pain after minor oral surgery procedures.43 The study lacked an assessment of whether celecoxib resulted in less postoperative bleeding.43
Another randomized, placebo-controlled, parallel-group study compared the efficacy of ibuprofen liquid-gels 400 mg and celecoxib 200 mg.44 The results demonstrated that both medications were superior to placebo. Ibuprofen demonstrated faster onset time and statistically superior analgesic efficacy except at the time of redosing the second or third dose (ie, hours 3, 4, and 8), which is consistent with a shorter duration of action compared with celecoxib.44 Patients in the ibuprofen group were 50% less likely to take a rescue analgesic than the celecoxib group in the first 12 hours after impacted third-molar surgery.44 The recommended dosing for celecoxib for acute pain is an initial dose of 400 mg that can be followed by an additional 200 mg if needed on the first day. On subsequent days, the dosing is 200 mg every 12 hours as needed for pain.45 Given the side-effect profile of COX-2 inhibitors and the delayed analgesic onset of celecoxib in particular, the clinician should carefully review the patient's medical history for cardiovascular disease.42,45
Data Demonstrate That NSAIDs Be the First-Line Medications for Acute Postoperative Dental Pain of Moderate to Severe Intensity
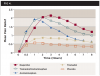
Analgesic studies have demonstrated the efficacy of NSAIDs in the management of moderate to severe postoperative dental pain. They have included use of the Dental Impaction Pain Model, one of the most widely used acute pain models.46 Much of these data have been available since the early 1980s, which only serves to heighten the tragedy of the role of dental prescribing practices in the opioid epidemic.3 Hundreds of trials involving thousands of patients illustrate the data summarized in Figure 347 and justify the prescribing regimens in Figure 1.27,28 Cooper et al demonstrated that ibuprofen 400 mg has superior analgesic efficacy to aspirin 650 mg plus codeine 60 mg, followed by aspirin 650 mg, which was better than codeine 60 mg, and lastly placebo (Figure 3).47 These data originated from a 1982 trial in which aspirin was used. However, acetaminophen can be logically substituted for aspirin because it has been demonstrated that acetaminophen, although lacking anti-inflammatory activity, is equianalgesic to aspirin: 650 mg of acetaminophen will produce equivalent analgesic to 650 mg of aspirin.48
Edwards et al collected data from multiple clinical trials involving dental pain and demonstrated that the opioid tramadol was only marginally better than the placebo control.49 Acetaminophen 650 mg demonstrated marked improvement over tramadol 75 mg and placebo. The combination of acetaminophen 650 mg and tramadol 75 mg was slightly better than acetaminophen 650 mg alone, demonstrating that the benefit of tramadol was secondary to the pain relief from acetaminophen alone. Lastly, ibuprofen 400 mg demonstrated superior analgesic efficacy and longer duration of pain relief than the acetaminophen plus opioid combination (Figure 4).49
Conclusions
There is an ongoing opioid crisis in the United States, and prescription analgesics play a major role in the exposure and potential for misuse, abuse, and diversion of medications. In 2012, dentists were the second-highest prescribers of immediate-release opioids, after primary care physicians.7,8 Dentists were also the top prescribers for adolescents, and opioid use in adolescence is associated with an increased risk of future opioid misuse.9,13 Less than half the opioids prescribed after surgical extractions are typically used, leaving leftover medications for potential diversion, misuse, or abuse by either the patient or other individuals with access to the medications.5,19 Increased awareness of the role of prescribing practices in the opioid epidemic has resulted in changes in guidelines and regulations, including state and federal legislation, implementation of PDMPs, and increased continuing education requirements.
The Dental Impaction Pain Model, which has been widely used for nearly four decades, has shown that NSAIDs are effective, non-addicting analgesics for postsurgical dental pain.46 The multimodal analgesic approach intercepts pain at various points on the pain pathways and interferes with different processes by using medication in different drug classes. This approach produces additive analgesia while reducing the dose of any single analgesic, thus reducing the side effects of each drug used. This concept is not unusual in dentistry, with the ubiquitous use of local anesthetic to prevent the transmission of afferent pain signals followed by the prescription of some combination of NSAIDs, acetaminophen, and opioids. The use of long-acting local anesthesia can reduce the breakthrough of pain, whereas NSAIDs should be used as a first-line drug (or acetaminophen when NSAIDs are contraindicated). Opioids should be reserved for severe breakthrough pain or when NSAIDs are contraindicated, and the prescriptions should be minimized to a 2- to 3-day course. Patients with persistent pain should be evaluated before additional opioids are prescribed.23,24,27,29
About the Authors
Nadia Laniado, DDS, MPH
Assistant Professor, Department of Dentistry and Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, New York
Elliot V. Hersh, DMD, MS, PhD
Professor, Oral Surgery and Pharmacology, Director, Division of Pharmacology, University of Pennsylvania School of Dental Medicine, Philadelphia, Pennsylvania
Victor M. Badner, DMD, MPH
Chair, Department of Dentistry/OMFS, Jacobi Medical Center and North Central Bronx Hospital, Bronx, New York
Mana Saraghi, DMD
Director, Dental Anesthesiology Residency Program, Jacobi Medical Center, Bronx, New York; Assistant Professor, Department of Dentistry, Albert Einstein College of Medicine, Bronx, New York
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
References
1. Rudd RA, Aleshire N, Zibbell JE, Gladden RM. Increases in drug and opioid overdose deaths-United States, 2000-2014. MMWR Morb Mortal Wkly Rep. 2016;64(50-51)1378-1382.
2. Florence CS, Zhou C, Luo F, Xu L. The economic burden of prescription opioid overdose, abuse, and dependence in the United States, 2013. Med Care. 2016;54(10):901-906.
3. Van Zee A. The promotion and marketing of OxyContin: commercial triumph, public health tragedy. Am J Public Health. 2009;99(2):221-227.
4. Chisholm-Burns MA, Spivey CA, Sherwin E, et al. The opioid crisis: origins, trends, policies, and the roles of pharmacists. Am J Health Syst Pharm. 2019;76(7):424-435.
5. Maughan BC, Hersh EV, Shofer FS, et al. Unused opioid analgesics and drug disposal following outpatient dental surgery: a randomized controlled trial. Drug Alcohol Depend. 2016;168:328-334.
6. Wardhan R, Chelly J. Recent advances in acute pain management: understanding the mechanisms of acute pain, the prescription of opioids, and the role of multimodal pain therapy. F1000Res. 2017;6:2065.
7. Gupta N, Vujicic M, Blatz A. Opioid prescribing practices from 2010 through 2015 among dentists in the United States: what do claims data tell us? J Am Dent Assoc. 2018;149(4):237-245.e6.
8. Lutfiyya MN, Gross AJ, Schvaneveldt N, et al. A scoping review exploring the opioid prescribing practices of US dental professionals. J Am Dent Assoc. 2018;149(12):1011-1023.
9. Volkow ND, McLellan TA, Cotto JH, et al. Characteristics of opioid prescriptions in 2009. JAMA. 2011;305(13):1299-1301.
10. Denisco RC, Kenna GA, O'Neil MG, et al. Prevention of prescription opioid abuse: the role of the dentist. J Am Dent Assoc. 2011;142(7):800-810.
11. Friedman JW. The prophylactic extraction of third molars: a public health hazard. Am J Public Health. 2007;97(9):1554-1559.
12. Compton WM, Jones CM, Baldwin GT, et al. Targeting youth to prevent later substance use disorder: an underutilized response to the US opioid crisis. Am J Public Health. 2019;109(S3):S185-S189.
13. Miech R, Johnston L, O'Malley PM, et al. Prescription opioids in adolescence and future opioid misuse. Pediatrics. 2015;136(5):e1169-e1177.
14. Suda KJ, Durkin MJ, Calip GS, et al. Comparison of opioid prescribing by dentists in the United States and England. JAMA Netw Open. 2019;2(5):e194303.
15. Guy GP Jr, Zhang K, Bohm MK, et al. Vital signs: changes in opioid prescribing in the United States, 2006-2015. MMWR Morb Mortal Wkly Rep. 2017;66(26):697-704.
16. McCauley JL, Leite RS, Melvin CL, et al. Dental opioid prescribing practices and risk mitigation strategy implementation: identification of potential targets for provider-level intervention. Subst Abus. 2016;37(1):9-14.
17. Hudgins JD, Porter JJ, Monuteaux MC, Bourgeois FT. Trends in opioid prescribing for adolescents and young adults in ambulatory care settings. Pediatrics. 2019;143(6).
18. Schroeder AR, Dehghan M, Newman TB, et al. Association of opioid prescriptions from dental clinicians for US adolescents and young adults with subsequent opioid use and abuse. JAMA Intern Med. 2019;179(2):145-152.
19. Bicket MC, Long JJ, Pronovost PJ, et al. Prescription opioid analgesics commonly unused after surgery: a systematic review. JAMA Surg. 2017;152(11):1066-1071.
20. Fink DS, Schleimer JP, Sarvet A, et al. Association between prescription drug monitoring programs and nonfatal and fatal drug overdoses: a systematic review. Ann Intern Med. 2018;168(11):783-790.
21. McCalmont JC, Jones KD, Bennett RM, Friend R. Does familiarity with CDC guidelines, continuing education, and provider characteristics influence adherence to chronic pain management practices and opioid prescribing? J Opioid Manag. 2018;14(2):103- 116.
22. Keith DA, Shannon TA, Kulich R. The prescription monitoring program data: what it can tell you. J Am Dent Assoc. 2018;149(4):266-272.
23. Rasubala L, Pernapati L, Velasquez X, et al. Impact of a mandatory prescription drug monitoring program on prescription of opioid analgesics by dentists. PloS One. 2015;10(8):e0135957.
24. American Dental Association announces new policy to combat opioid epidemic [news release]. American Dental Association website. March 26, 2018. https://www.ada. org/en/press-room/news-releases/2018-archives/ march/american-dental-association-announcesnew-policy-to-combat-opioid-epidemic. Accessed August 6, 2020.
25. Hollingshead NA, Meints S, Middleton SK, et al. Examining influential factors in providers' chronic pain treatment decisions: a comparison of physicians and medical students. BMC Med Educ. 2015;15:164.
26. Contreras OA, Stewart D, Valachovic RW. The Role of Dental Education in the Prevention of Opioid Prescription Drug Misuse. Washington, DC: American Dental Education Association; March 2018.
27. Moore PA, Hersh EV. Combining ibuprofen and acetaminophen for acute pain management after thirdmolar extractions. J Am Dent Assoc. 2013;144(8):898- 908.
28. Hersh EV, Kane WT, O'Neil MG. Prescribing recommendation for the treatment of acute pain in dentistry. Compend Contin Educ Dent. 2011;32(3):22-30.
29. Hersh EV, Saraghi M, Moore PA. The prescription opioid abuse crisis and our role in it. Gen Dent. 2018;66(4):10-13.
30. Krenzelok EP, Royal MA. Confusion: acetaminophen dosing changes based on NO evidence in adults. Drugs R D. 2012;12(2):45-48.
31. Dionne RA. Suppression of dental pain by the preoperative administration of flurbiprofen. Am J Med. 1986;80(3A):41-49.
32. Dionne RA, Cooper SA. Evaluation of preoperative ibuprofen for postoperative pain after removal of third molars. Oral Surg Oral Med Oral Pathol. 1978;45(6):851-856.
33. Gordon SM, Brahim JS, Dubner R, et al. Attenuation of pain in a randomized trial by suppression of peripheral nociceptive activity in the immediate postoperative period. Anesth Analg. 2002;95(5):1351-1357.
34. Saraghi M, Hersh EV. Three newly approved analgesics: an update. Anesth Prog. 2013;60(4):178-187.
35. Exparel prescribing information. San Diego, CA: Pacira Pharmaceuticals, Inc.; 2018.
36. Bultema K, Fowler S, Drum M, et al. Pain reduction in untreated symptomatic irreversible pulpitis using liposomal bupivacaine (Exparel): a prospective, randomized, double-blind trial. J Endod. 2016; 42(12):1707-1712.
37. Glenn B, Drum M, Reader A, et al. Does liposomal bupivacaine (Exparel) significantly reduce postoperative pain/numbness in symptomatic teeth with a diagnosis of necrosis? A prospective, randomized, double-blind trial. Endod. 2016;42(9):1301-1306.
38. Lieblich SE, Hassan D. Liposomal bupivacaine use in third molar impaction surgery: INNOVATE study. Anesth Prog. 2017;64(3):127-135.
39. Butterworth JF, Mackey DC, Wasnick JD. Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill Companies; 2013.
40. Chen Q, Chen J, Hu B, et al. Submucosal injection of dexamethasone reduces postoperative discomfort after third-molar extraction: a systematic review and meta-analysis. J Am Dent Assoc. 2017;148(2):81-91.
41. Lenzer J. FDA advisers warn: COX 2 inhibitors increase risk of heart attack and stroke. BMJ. 2005; 330(7489):440.
42. FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes. Food and Drug Administration website. Updated February 26, 2018. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-strengthenswarning-non-aspirin-nonsteroidal-anti-inflammatory. Accessed August 6, 2020.
43. Hanzawa A, Handa T, Kohkita Y, et al. A comparative study of oral analgesics for postoperative pain after minor oral surgery. Anesth Prog. 2018;65(1):24-29.
44. Doyle G, Jayawardena S, Ashraf E, et al. Efficacy and tolerability of nonprescription ibuprofen versus celecoxib for dental pain. J Clin Pharmacol. 2002;42(8):912-919.
45. Celebrex prescribing information. New York, NY: Pfizer, Inc.; 2016.
46. Cooper SA, Desjardins PJ. The value of the dental impaction pain model in drug development. Methods Mol Biol. 2010;617:175-190.
47. Cooper SA, Engel J, Ladov M, et al. Analgesic efficacy of an ibuprofen-codeine combination. Pharmacotherapy. 1982;2(3):162-167.
48. Cooper SA. Comparative analgesic efficacies of aspirin and acetaminophen. Arch Intern Med. 1981;141(3 spec no):282-285.
49. Edwards JE, McQuay HJ, Moore RA. Combination analgesic efficacy: individual patient data meta-analysis of single-dose oral tramadol plus acetaminophen in acute postoperative pain. J Pain Symptom Manage. 2002;23(2):121-130.