You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
After an extraction, when a dense polytetrafluorethylene (d-PTFE) barrier is used in conjunction with a bone graft to regenerate a buccal dehiscence, typically buccal and lingual flaps are elevated to facilitate barrier placement.1 However, flap elevation is a shortcoming of this technique, especially in the esthetic zone, because it has the potential to induce bone loss and recession due to disturbance of the periosteal blood supply.2 Historically, to avoid tissue manipulation, a procedure referred to as the "ice cream cone" technique was used.2,3 This method consists of flaplessly extracting a tooth and placing a resorbable barrier shaped like an ice cream cone into the socket. The barrier is compressed against the defective bony plate. Then, a bone graft is inserted into the socket, and the barrier is folded over the bone graft and sutured to the palatal tissue. Resorbable barriers, however, begin to degrade within 2 weeks,4 which can cause loss of graft material and development of a soft-tissue defect.
This article presents a modification of the ice cream cone technique. A nonresorbable d-PTFE barrier is placed in and over a socket that has received a bone graft without a buccal flap being raised. (Editor's Note: The barrier the authors use is Cytoplast® [Osteogenics Biomedical, osteogenics.com]. Other d-PTFE barriers available include TefGen FD™, Lifecore Biomedical LLC, lifecore.com; Symbios OsteoShield®, DENTSPLY Implants, dentsplyimplants.com; and High-density Gore-Tex, W.L. Gore & Associates Inc., gore.com.) Employing d-PTFE prevents the barrier from resorbing prematurely, thereby facilitating guided bone regeneration (GBR). The authors have labeled this technique the Cytocone procedure, because it uses a Cytoplast barrier in the shape of an ice cream cone.
Background Information
In 2007 Elian et al proposed a classification for post-extraction sockets: type I, type II, and type III.2 In type I sockets, both soft tissue and bone are at normal levels relative to the cementoenamel junction (CEJ). Type II cases are those in which the soft tissue is level or coronal to the CEJ, but the buccal bony plate is dehisced. In type III sockets, the soft tissue and the buccal bony plate are compromised.2
Regarding type II defects, Elian et al advocated using the ice cream cone technique with a resorbable barrier to manage a buccal plate dehiscence,2 a technique, it should be noted, that was originally described by Tarnow.3 The case described and illustrated in the present article modifies the ice cream cone technique. The alterations consist of using a nonresorbable barrier (ie, d-PTFE), which is tucked under the palatal flap to enhance its stability and facilitate long-term retention (ie, 5 weeks). The lingual flap and nonresorbable barrier are secured with Vicryl® sutures (Ethicon, ethicon.com).
With respect to characteristics of d-PTFE barriers, Greenstein et al reviewed the benefits of using d-PTFE versus expanded polytetrafluorethylene (e-PTFE) barriers and the advantages of employing d-PTFE barriers versus resorbable membranes.1 It was noted that d-PTFE and e-PTFE have different pore sizes, which affects their ability to avoid infections.5 The pore size of e-PTFE ranges from 5 μm to 30 μm, while that of d-PTFE is 0.2 μm.1 The d-PTFE barriers prevent bacteria from penetrating the barrier. This is beneficial, because bacterial penetration of the barrier can induce an infection at the grafted site and cause failure of the GBR procedure.5 Furthermore, diminished pore size impedes cellular ingrowth, and fibroblasts can only adhere to d-PTFE, thereby enabling relatively easy removal of the barrier.5
d-PTFE barriers can be left exposed in the oral cavity for 4 to 6 weeks or longer without concern for their premature dissolution or inducing an infection.1 Good oral hygiene by the patient and postoperative care are also necessary to ensure success of the Cytocone procedure. To circumvent barrier displacement, patients should be instructed not to chew where the barrier is present and to avoid using a pulsating water device or sucking in that area.
Cytocone Procedure: Case Report
A 33-year-old woman presented with a buccal fistula at the apex of No. 8, and there was an 8-mm mid-buccal probing depth (Figure 1). The tooth had been treated multiple times by an endodontist. Based on the tooth's dental history, mobility, and its poor endodontic and periodontal prognosis, it was deemed hopeless and scheduled for extraction (Figure 2).
The right central incisor was removed atraumatically (Figure 3) without elevating a buccal flap. The presence of the buccal bone dehiscence was confirmed with the use of a periodontal probe. Measurements from the free gingival margin to the crest of the buccal bone and a horizontal assessment of the defect size indicated a dehiscence that was 8-mm tall and 5-mm wide. The distance from the free gingival margin to the most apical point in the socket was 10 mm.
A d-PTFE (Cytoplast) barrier was trimmed into the shape of an ice cream cone to conform to the socket's morphology (Figure 4). The barrier was placed inside the alveolus and compressed laterally into the buccal dehiscence (Figure 5). Small-particle, mineralized cancellous freeze-dried bone allograft (ie, 0.25 mm to 1 mm) was inserted into the socket and packed against the barrier. The socket was filled 1 mm to 2 mm above the alveolar crest to aid in attaining a convex rather than concave gingival architecture at the socket opening upon removal of the barrier. The barrier was tucked under the palatal flap (3 mm) and secured with Vicryl 4-0 single interrupted sutures (Figure 6 through Figure 8).
Postoperatively, the patient was prescribed 875 mg amoxicillin twice a day for 7 days and instructed to use chlorhexidine gluconate 0.12% mouth rinse twice a day for 30 seconds for the first week. Subsequently, the exposed barrier surface was swabbed with chlorhexidine on a Q-tip twice per day for the next 4 weeks.
The patient was scheduled for weekly postoperative assessments. The barrier was removed after 5 weeks using a college plier without anesthetizing the patient. After the barrier was removed, osteoid tissue (red connective tissue) was seen covering the bone graft, as anticipated (Figure 9). If bone graft particles are present at the extraction site, they can be left in place, as connective tissue will cover them within 1 to 2 weeks. The epithelium creeps across the reddish connective tissue, and the site becomes pinkish in approximately 2 weeks, as occurred in this case (Figure 10).6
Results
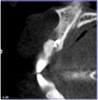
The patient returned at 4 months postoperatively for site evaluation (Figure 11). Bone sounding with an anesthetic needle indicated formation of hard bony surface. At 4 months lamellar bone is present.7 A cone-beam computed tomography (CBCT) scan of site No. 8 radiographically confirmed that the bony ridge had been regenerated (Figure 12). CBCT measurements indicated the maxillary ridge was 6.44 mm wide and 21 mm tall.
To place an implant without inducing recession, papillae-sparing incisions were created on the mesial and distal of the edentate area at site No. 8. Vertical incisions were made 1 mm away from adjacent teeth and connected with a mid-crestal incision (Figure 13). The extent of the vertical incisions was 3 mm buccally and lingually to expose the alveolar ridge. Horizontal and vertical bone regeneration was clinically confirmed (Figure 14). A 3.3-mm x 12-mm bone level tapered, narrow-connection implant (Straumann, straumann.com) was inserted, and it attained initial primary stability at 25 Ncm (Figure 15 and Figure 16). It was desired to have more than 1 mm of bone buccal and lingual to the implant so as to avoid bone resorption and recession. Then, 4-0 Vicryl single interrupted sutures were used to close the flap (Figure 17).
The patient was brought back weekly for 4 weeks for postoperative follow-up. Healing was satisfactory (Figure 18). Four months after implant placement, the final restoration, a porcelain-fused-to-metal screw-retained crown, was inserted at site No. 8 (Figure 19).
Discussion
The Cytocone procedure is a modification of the original ice cream cone technique.2,3 Its major benefit compared to the original technique is use of a nonresorbable barrier (ie, d-PTFE). This eliminates the possibility of premature barrier resorption by salivary enzymes, which can cause loss of bone graft material, interrupt the process of GBR, and result in a deformed ridge vertically or horizontally.
Concerning bone resorption after extractions, Tan et al reported 2.46 mm to 4.56 mm of horizontal bone loss (mean 3.79 mm) and 0.9 mm to 3.6 mm of vertical bone decrease (mean 1.24 mm) after teeth removal if flaps were elevated.8 In contrast, Lee et al noted there was around 1 mm of vertical bone loss and 1 mm of horizontal bone loss if a flap was not elevated extracting a tooth.9 Therefore, it is beneficial not to raise a flap when removing a tooth, especially in the esthetic zone, because excessive horizontal bone loss and possibly recession may result.10
With respect to the cause of bone resorption, after a flapless extraction, a limited amount of vertical bone loss often occurs due to loss of blood supply from the periodontal ligament.9 On the other hand, increased horizontal bone resorption occurs if a flap is elevated in conjunction with an extraction, because there is interruption of the periodontal and periosteal blood supply.9 The Cytocone procedure avoids raising a flap on the buccal where the bone is thinnest.11,12 A small flap is elevated palatally to allow the barrier to be secured. However, less bone loss is expected palatally, because the bone there is thicker than labially.13,14
Because the Cytocone technique uses a nonresorbable barrier, the clinician is able to dictate how long the barrier remains in place. Usually it is retained for 5 to 6 weeks to ensure predictable GBR.1 This interval allows enough time for osteoid formation and connective tissue coverage of the socket opening. After barrier removal, the epithelium migrates across the connective tissue within 2 weeks.6 Epithelium travels approximately 0.5 mm to 1 mm per day.15
Regarding the presented case report, because the barrier is placed within the socket, it precludes regenerating the ridge wider than the alveolar housing of the existing ridge. If a wide ridge, greater than the existing alveolar housing was desired, or if there was concern that the regenerated ridge would partially resorb, it would dictate altering the procedure and placing a barrier external to the buccal plate. This would entail elevating the buccal flap and possibly cause papilla blunting in the surgical site and induce resorption of the buccal plate in nongrafted sites.
Clinicians have several choices with respect to treatment planning a case if an implant is going to be inserted to replace a hopeless tooth that is adjacent to buccal bony dehiscence. After an extraction, a GBR procedure (bone graft plus a barrier) can be accomplished with a resorbable or nonresorbable barrier in conjunction with primary closure,16 or a d-PTFE barrier can be employed without primary closure.1 As discussed, the ice cream cone technique or the Cytocone procedure can be used to regenerate bone prior to placing an implant,2,3 or implantation can be performed in conjunction with a GBR procedure.17,18 All of these procedures have advantages and limitations.
In the first option, after bone grafting and placement of a barrier, primary closure is required and involves flap elevation. This approach may alter the mucogingival line and decrease the depth of the vestibule, and there is increased morbidity compared to GBR with a d-PTFE barrier that does not involve primary closure.1 Heretofore, d-PTFE barrier placement was associated with buccal and lingual flap elevation, which can induce horizontal ridge resorption.9 As previously discussed, if the ice cream cone technique is performed with a resorbable barrier, the barrier may degrade prematurely, which can result in incomplete GBR.4 In contrast, the Cytocone procedure assists bone regeneration without compromising esthetics; and, furthermore, patients have minimal discomfort.
Another technique to replace an extracted tooth entails implant placement with simultaneous bone grafting.17 This usually involves flap elevation to place a barrier and the need to attain primary closure. Some issues related to this procedure, however, require discussion. If the bone graft is not fully successful, the implant will be only partially encased in bone and this will complicate further therapy. Specifically, if additional bone grafting is needed, achieving osseointegration of the exposed threads of the implant will be problematic. Sarnachiaro et al recently published a modification of this procedure in which flapless procedures were used to remove teeth that had buccal bony dehiscences.18 An implant was inserted and, buccal to the implant, a bone graft and resorbable barrier were placed in juxtaposition to repair the osseous defect. Successful procedures were performed on 10 posterior teeth. The authors indicated posterior teeth were used to avoid any esthetic issues if the graft did not perform well. To occlusally retain the bone graft material, a custom healing abutment and a screw-down provisional were placed. It should be noted that without raising a flap, depending on the size of the socket, it may be difficult to place an implant and a bone graft between the barrier and the implant in a socket. In addition, similar to the above remarks, failure to attain optimal GBR would result in an implant only partially encased in bone.
Conclusion
The Cytocone procedure can be used to attain bony regeneration of a buccal dehiscence without elevating a buccal flap. This method avoids flap advancement and the need to attain primary closure. The procedure is relatively easy to carry out and the patient experiences only minor discomfort. Repair of a defective ridge in the esthetic zone prior to implantation helps eliminate untoward issues that can occur when implantation and bone grafting are attempted simultaneously.
About the Authors
Khashayar Kordbacheh Changi, DMD
Periodontal Resident, Department of Periodontics, College of Dental Medicine, Columbia University, New York, New York
Gary Greenstein, DDS, MS
Clinical Professor, Department of Periodontics, College of Dental Medicine, Columbia University, New York, New York; Private Practice, Surgical Implantology and Periodontics, Freehold, New Jersey
Queries to the author regarding this course may be submitted to
authorqueries@aegiscomm.com.
References
1. Greenstein G, Carpentieri JR. Utilization of d-PTFE barriers for post-extraction bone regeneration in preparation for dental implants. Compend Contin Educ Dent. 2015;36(7):465-473.
2. Elian N, Cho SC, Froum S, et al. A simplified socket classification and repair technique. Pract Proced Aesthet Dent. 2007;19(2):99-104.
3. Tarnow D. Ice cream cone technique. Lecture presented at: Annual Meeting of the American Academy of Periodontology. 2000.
4. Soldatos NK, Stylianou P, Koidou VP, et al. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017;48(2):131-147.
5. Cytoplast Regeneration Products Catalog. Seoul, Korea: Osteogenics Biomedical; 2014. http://www.osstem.de/data/library/2014enCytoplast.pdf. Accessed April 4, 2018.
6. Barber HD, Lignelli J, Smith BM, Bartee BK. Using a dense PTFE membrane without primary closure to achieve bone and tissue regeneration. J Oral Maxillofac Surg. 2007;65(4):748-752.
7. Eriksson C, Ohlson K, Richter K, et al. Callus formation and remodeling at titanium implants. J Biomed Mater Res A. 2007;83(4):1062-1069.
8. Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the "ice cream cone" flapless grafting technique. Int J Periodontics Restorative Dent. 2014;34(3):399-403.
9. Lee CT, Chiu TS, Chuang SK, et al. Alterations of the bone dimension following immediate implant placement into extraction socket: systematic review and meta-analysis. J Clin Periodontol. 2014;41(9):914-926.
10. Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results. Clin Oral Implants Res. 2007;18(5):552-562.
11. Januário AL, Duarte WR, Barriviera M, et al. Dimension of the facial bone wall in the anterior maxilla: a cone-beam computed tomography study. Clin Oral Implants Res. 2011;22(10):1168-1171.
12. Katranji A, Misch K, Wang HL. Cortical bone thickness in dentate and edentulous human cadavers. J Periodontol. 2007;78(5):874-878.
13. Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005;32(2):212-218.
14. Caneva M, Salata LA, de Souza SS, et al. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs. Clin Oral Implants Res. 2010;21(9):885-890.
15. Engler WO, Ramfjord SP, Hiniker JJ. Healing following simple gingivectomy. A tritiated thymidine radioautographic study. I. Epithelialization. J Periodontol. 1966;37(4):298-308.
16. Carpio L, Loza J, Lynch S, Genco R. Guided bone regeneration around endosseous implants with anorganic bovine bone mineral. A randomized controlled trial comparing bioabsorbable versus non-resorbable barriers. J Periodontol. 2000;71(11):1743-1749.
17. Becker W, Goldstein M. Immediate implant placement: treatment planning and surgical steps for successful outcome. Periodontol 2000. 2008;47:79-89.
18. Sarnachiaro GO, Chu SJ, Sarnachiaro E, et al. Immediate implant placement into extraction sockets with labial plate dehiscence defects: a clinical case series. Clin Implant Dent Relat Res. 2016;18(4):821-829.