You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Cone-beam computed tomography (CBCT) has revolutionized dental diagnostic imaging. Its introduction marked a major turn in radiologic diagnosis, providing the “third dimension” that was missing in traditional dental radiographs (periapical and panoramic). However, the introduction of this technology raised a few important issues. The first was the dental profession’s overall lack of familiarity with multi-planar images and the sectional anatomy of the maxillo-facial region, which is crucial in diagnosis. Another was the importance of the scanner’s operator and the prescribing clinician. Technical expertise is critical in the acquisition of high-quality diagnostic CBCT images; however, it is equally important that the correct image type is prescribed and that the data is interpreted properly. To help practitioners make the most of their CBCT units, this article provides five key recommendations for the “day-to-day” utilization and operation of CBCT:
1. Properly Address the Diagnostic Concern
CBCT is an imaging modality used mostly for the assessment of hard tissues. Therefore, it's selection as an imaging tool is generally limited to the evaluation of osseous structures and teeth; however, in certain situations involving soft tissues, it can provide great value in ruling out some conditions. Its multi-planar imaging capabilities have provided the diagnostician with crucial information, including the depth of a developing pathological entity, its effects in the neighboring osseous boundaries, and more accurate identification of significant anatomical structures. Other pathological entities, such as caries, recurrent caries, and crown and root cracks or fractures, especially in the presence of extensive restorations, may not be visualized as well with CBCT. In such cases, the selection of CBCT should be made only in view of these shortcomings or more appropriate imaging modalities should be selected (eg, bitewing radiographs for caries and recurrent caries). CBCT has limited usefulness in soft tissue pathology, except in certain situations, such as cases in which the suspected soft tissue pathological entity is invading bone or when it produces calcified material.1 This makes taking an accurate medical and dental history and performing a thorough clinical examination absolutely mandatory in the process of prescribing the most appropriate imaging modality for the patient's situation.
CBCT also has proven itself to be an excellent diagnostic tool for surgical planning. Although its most common use is in dental implant pre-surgical planning, other complex oral surgical procedures have been “illuminated” diagnostically by CBCT, such as the removal of cystic lesions or complicated impactions.2
Similar to other radiologic examinations, CBCT scans are often required for periodic evaluation of possible changes in an ongoing pathological entity over time. In these cases, the clinician selects to periodically assess if a known lesion is progressing instead of taking an immediate treatment action. How often scans are performed is based upon the type of pathological entity and the rate at which it might be changing; however, clinicians must balance this decision with the principle of keeping patients' exposure to ionizing radiation As Low As "is" Reasonably Achievable (ALARA principle).
Follow-up radiologic examinations (including CBCT scans) are also prescribed in order to evaluate the results of a specific treatment or surgery. For example, a scan of the mandible can be ordered for the post-surgical evaluation of the jaw after the removal of a large cyst. These examinations are invaluable when determining the efficacy of a surgical procedure. As aforementioned, the extent of the procedure and the potential for recurrence of the lesion determines the frequency of the follow-up radiologic examinations needed. A direct comparison of the pre-surgical scan with the follow-up images can provide significant information about the success or failure of the procedure.3
2. Select the Appropriate CBCT Imaging Protocol
The imaging protocol establishes the proper technical parameters to allow for the best images to be acquired based on the special needs of the patient and the specific diagnostic concerns. For example, how large or small should the area of exposure (field of view) be? What level of image detail is required? Since almost all of the CBCT scanners currently on the market offer a range of fields of view, it is in the best interest of our patients to select one that will permit full assessment of the region of interest without missing anything or exposing too large of an area (Figure 1). The potential size of the pathological entity under investigation and the extent of the affected region will dictate the field of view necessary.4 A larger field of view should be selected when facial symmetry is to be investigated or skeletal anomalies that may require radiologic assessment of a large portion of the head. In most other cases, a single- or a dual-arch scan (or an even smaller field of view, such as 40 mm X 40 mm or 50 mm X 50 mm) is adequate for the evaluation of an area limited to 2 to 3 teeth or a quadrant of the jaw.
When there is a need for extra detail, a high-resolution (small voxel size) protocol should be selected. Contemporary CBCT machines can acquire imaging volumes with voxel sizes as low as 0.08 mm, which produces a highly detailed image. This type of protocol is excellent for diagnostic tasks such as the detection of possible ankylosis of an impacted tooth and possible root fractures or root resorption.5
Because the detail of the resulting images is higher, one may wonder why clinicians don’t acquire all CBCT scans in the smallest possible voxel size. This type of thinking should raise concerns for several reasons. First, the selection of a high-resolution protocol in most CBCT scanners will result in a higher dose of radiation being delivered to the patient, and radiation safety should be a prime concern of the dental professional. In addition, the higher-resolution imaging protocols often require a longer scan time, which can increase the chance of patient motion and have an affect on image quality and diagnosis.
As before, when a scan is taken for surgical planning, the field of view should be limited to the site of interest determined by the clinical examination, and the voxel resolution selected should be determined by the level of detail required.
3. Ensure CBCT Image Quality
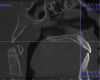
There is a documented link between radiologic image quality and diagnostic efficiency.6 In other words, a reduction in scan quality may obscure diagnostic information and compromise diagnosis. Patient motion during the scan acquisition and other image artifacts are the most important factors affecting image quality in CBCT studies. Patient motion is more likely to be seen in scans of either older individuals or children. The motion artifact can be recognized by the double margin it creates in the osseous boundaries, such as the maxillary and mandibular cortices. To limit motion artifacts, detailed patient instructions may be helpful as well as strict adherence to the manufacturer’s recommendations for scan acquisition (Figure 2). After the acquisition of a scan, the clinician should quickly review the image data for possible motion artifacts and retake the san if necessary.
Other kinds of artifacts that are related to the CBCT technology itself may be present and compromise image quality, sometimes rather significantly.7 These artifacts are an inherent problem of CBCT and medical computed tomography because their appearance is a product of the reconstruction algorithms employed to compose the digital CBCT and CT images. In addition, the presence of any radiopaque materials is a frequent cause of artifacts. Metallic dental restorations, fixed prostheses, posts, and even gutta-percha may create artifacts that can obscure the visualization of the region of interest (Figure 3). As a result, fine diagnostic tasks may be impossible in proximity to restorations with high radiopacity. A number of CBCT manufacturers currently offer artifact reduction applications. These seem to have improved the resulting image quality; however, any possible gain in diagnostic efficiency has yet to be determined (Figure 4).
Beam hardening is another type of image artifact that is closely linked to the metallic artifact in CBCT images. These are dark, linear or cup-like bands near metallic restorations or implants, which may mimic osseous defects around dental implants or dental caries around restorations. Sometimes, their existence in combination with metallic artifacts in a heavily restored dentition may severely affect image quality to the degree that close anatomical structures like the crest of the alveolar ridge may be completely obscured. If fine detail is of the essence, in order to avoid metallic artifacts, it is sometimes advisable to remove any large restorations or posts from the teeth prior to scanning (if there was a plan to replace the restoration). Other times, increasing the slice thickness of the respective sections will reduce the deteriorating effects of the beam hardening and metallic artifacts.
4. Select Proper Reconstructions
When volumetric data is acquired (as with CBCT and medical CT) the proper images need to be reconstructed in order to address a diagnostic concern. This is easy with CBCT because with very simple applications of the CBCT software a multitude of images are available in any desired plane of section. However, it is the diagnostician’s responsibility to reconstruct those images in the best way to provide an answer to the diagnostic task at hand. For example, if there is a need for alveolar bone height and width measurements, panoramic reconstructions and cross-sectional images (perpendicular to the jaws) are often the most appropriate. If there is a need for a thorough assessment of the maxillary sinuses, coronal orthogonal sections are usually best. Surface renderings (3D images) are usually the best for assessing facial asymmetry or fractures. In any case, instead of a standard set of reconstructions, a tailor-made set should be prepared to address each diagnostic task at hand.
5. Analyze All Available Images with the Proper Diagnostic Utilities
After all of the available diagnostic information is collected, the area of interest is assessed from all perspectives in order to correlate the reported or observed clinical findings to possible changes in the radiologic appearance of the hard tissues in the affected site. This includes a comparison of the region with the contralateral side to evaluate for possible asymmetry or unilateral irregularities of the anatomical structures; altered appearance of known tissues/structures; possible alteration, discontinuity, or even destruction of osseous boundaries; possible shape changes in known anatomical structures; possible mass development and features of the developing mass; possible effects of a mass on known anatomical structures and boundaries; and more (Figure 5). An accurate description of the entity under investigation will reveal useful information about the tissue of origin, its structure (ie, hollowed, cystic, or solid), and its nature (fast growing/aggressive or slow growing/subtle). In the end, a list containing all collected radiologic data should be compiled and used to create a differential diagnostic list consisting of all possible pathological entities that fit the collected descriptive data.
During data collection, all available diagnostic utilities should be used, including tools for assessing measurement, angle estimation, bone density, image orientation, and more. All are part of the goal to establish a diagnostic list that is as accurate as possible.
Following this analysis, the remainder of the imaging volume (other than the region of interest) should be evaluated as the next step. It should be mandatory that a thorough review of all anatomical areas included in the scan be performed in order to detect any possible incidental, silent pathological conditions unrelated to the reason for which the scan was acquired. When a specific field of view has been selected for a CBCT study, the image may include, unavoidably, a wider zone of tissues than is of interest. For example, when a field of view to evaluate the maxilla is selected, it may include the temporomandibular joints due to their proximity. In this case, the joints should be included in the diagnostician’s review to exclude any possible significant findings that may need to be addressed. It has been reported that findings of incidental entities may reach high numbers in CBCT studies, which is concerning.8,9 A key strategy in addressing these incidental findings is to develop a system to ensure that all anatomical areas included in the scan are reviewed by the clinician so that any abnormalities are detected and diagnosed. To take advantage of the full potential of this technology, the diagnostician may require additional training to improve his or her familiarity with tomographic imaging. This may also require clinicians to develop a deeper knowledge of the anatomy of the maxillo-facial region, so that certain recognized incidental entities may be linked to specific anatomical structures.
In conclusion, if a clinician does not feel qualified to review imaging data or detects something unfamiliar, he or she should consult a maxillo-facial radiologist for advice, guidance, or even consultation services. CBCT will continue evolving and providing a great diagnostic contribution to the dental profession; it is ultimately up to the clinician’s professional responsibility, judgment, and knowledge to make the most of it.
References
1. Angelopoulos C. Cone beam tomographic imaging anatomy of the maxillofacial region. Dent Clin North Am. 2008;52(4):731-752.
2. Becker A, Chaushu S, Casap-Caspi N. Cone-beam computed tomography and the orthosurgical management of impacted teeth. J Am Dent Assoc. 2010;141(Suppl 3):14S-8S.
3. Kapila SD. Cone Beam Computed Tomography in Orthodontics: Indications, Insights, and Innovations. Hoboken, New Jersey: Wiley Blackwell; 2014.
4. Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am. 2008;52(4):707-730.
5. Vaz de Souza D, Schirru E, Mannocci F, Foschi F, Patel S. External cervical resorption: a comparison of the diagnostic efficacy using 2 different cone-beam computed tomographic units and periapical radiographs. J Endod. 2017;43(1):121-125.
6. White S, Pharoah M. Oral Radiology: Principles and Interpretation. 5th ed. St. Louis, MO: Mosby; 2004.
7. Bechara B, McMahan CA, Geha H, Noujeim M. Evaluation of a cone beam CT artifact reduction algorithm. Dentomaxillofac Radiol. 2012;41(5):422–428.
8. Dobele I, Kise L, Apse P, Kragis G, Bigestans A. Radiographic assessment of findings in the maxillary sinus using cone-beam computed tomography. Stomatologija. 2013;15(4):119-22.
9. Miles DA. Clinical experience with cone-beam volumetric imaging—report of findings in 381 cases. Computerized Tomography. 2005;20:416–424
About the Author
Christos Angelopoulos, DDS, MSc, Diplomate ABOMR
Past President
American Academy of Oral & Maxillo-facial Radiology