You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Disclosures: The authors had no disclosures to report.
In young patients (≤30 years old), the ideal treatment for deep caries lesions is to preserve the vitality of the dentin-pulp complex through adequate protection.1 Pulp is responsible for the formation of the reparative dentin/mineralized barrier in teeth with carious lesions.2 However, dental professionals may have some confusion regarding the applicability and indications of such procedures; they need to fully understand the effects of lesion depth and the response of the pulp after the stimuli.
The first step may be the pulp-condition diagnosis, resulting in a treatment plan.3,4 Frequently the proximity of the pathological cavity with the pulp organ, especially during cavity preparation, can lead to pulp exposure. This may allow the penetration of bacteria or toxic substances originating from the restorative materials.5
To make the maintenance of pulp vitality possible, different conservative treatments can be used, depending of the presence or absence of remaining deep caries lesions (Table 1).
The indirect pulp capping can be indicated for deep cavities because there is no pulp exposure to decay. The procedure involves the application of a biocompatible material on the pulpal wall,6 which stimulates tertiary dentin production and sclerotic dentin, resulting in a biological seal, capable of avoiding irritant substances released from the final restorative material, especially the adhesive systems.7 For this purpose, the most widely used material is calcium hydroxide, due to its high biocompatibility, handling, and low cost.6,8,9 More recently, with its high success rates due to the material resilience and biological properties, mineral trioxide aggregate (MTA) is also employed.7,10 Following the application of the capping material, a protective base of glass-ionomer cement (GIC) and a final restoration, with resin composite or amalgam, has to be placed.
In some clinical situations, during deep cavity preparation and after the complete removal of the decayed dentin, pulp can be exposed accidentally and needs to be protected to guarantee the maintenance of its vitality. In these situations, calcium hydroxide powder or MTA can be used. Both materials present great hemostatic properties, resulting in pulp tissue repair due to superficial necrosis by contact. The contact between pulp tissue and the material also stimulate mineralized barrier formation after cell differentiation on the exposed area, resulting in a new biological sealing.11,12 After placement of the powder to protect the pulp-dentin complex, the restorative procedure is similar to the process for deep cavities indirect capping: calcium hydroxide cement, GIC base, and amalgam/resin composite.
Another scenario consists of the presence of decay compromising the pulp organ. These cases generate many doubts for clinicians regarding the best therapeutic approaches (Table 1).5 In general, conservative techniques can be an option for young patients, keeping the tooth’s pulp vitality and allowing conservative interventions in the future.13
The more conservative approach, indicated in deep caries lesions with respect to minimal pulp exposure, is stepwise excavation. The goals of this tactic are to mechanically remove the infected (demineralized) dentin, reducing the amount of cariogenic microorganisms,2 and to seal the partially demineralized dentin by placement of calcium hydroxide paste over the remaining pulpal wall and to perform a provisional restoration with GIC (first intervention). The biological mechanism consists of the reduction of the cariogenic microorganisms’ action (bacteriostatic action) and stimulation of odontoblasts to form reparative and sclerotic dentin.14 After 45 to 90 days, the remaining carious dentin can be removed and the cavity preparation can be performed with a lower risk for pulpal exposure.15 In fact, this procedure has been shown to reduce pulp exposures by 98% when compared with the one-visit approach in which all carious lesions are removed; the literature supports this technique to avoid more complex restorative procedures.16-20
Direct pulp capping is another conservative treatment that involves vital pulp exposure without surrounding decayed tissue. In such cases, a direct capping with biomaterial (calcium hydroxide paste/powder or MTA) is essential for maintaining the pulp vitality,20,21 through the formation of a new mineralized barrier.22 Then, a provisional restoration may be executed with the use of a calcium hydroxide cement and GIC. After 45 to 90 days, the mineralized barrier should be clinically checked and the same sequence described for indirect capping can be adopted.
In cases in which the pulp tissue is involved with decayed tissue, a partial pulpotomy may be performed, characterized by the superficial removal of the contaminated pulp tissue; the contaminated pulp is removed to the level of healthy tissue.23 Despite the described procedures, in cases in which the pulp tissue is more contaminated, the total removal of coronary pulp tissue is a more conservative choice compared with performing root-canal treatments.
The goal of partial and total pulpotomies, stepwise excavation, and direct pulp capping is to ensure a clean surgical wound and improved interaction between the pulp and capping agent, stimulating the differentiation of mesenchymal stem cells,24 forming a new mineralized dentin barrier, and isolating the pulp cavity. For all these approaches, the patient’s age is an important factor due to the higher capacity of pulp tissue to regenerate in young patients.11,25 The authors recommend the use of this technique for permanent teeth.
Considering the vast array of therapeutic procedures, professionals face numerous concerns. Thus, this article attempts to present the different treatment sequences for maxillary incisors with extensive carious lesions, with maintenance of the pulp vitality and restoration of teeth anatomy and function. The authors advise against using this procedure in cases in which irreversible pulpitis is diagnosed.
Case Report
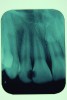
A 12-year-old male presented with extensive carious lesions observed on teeth Nos. 7 through 10, which were accompanied with gingivitis (Figure 1). The pulpal condition was verified through thermal sensitivity tests and vertical percussion, both being satisfactory (Figure 2). The proximity of the lesions with the pulp chamber and the absence of periapical lesions, especially in the right lateral incisor, were observed by the radiographic examination (Figure 3).
The established treatment plan consisted of stepwise excavation in all compromised teeth and the subsequent restoration with resin composite. During the cavity preparation, the pulp of the right lateral incisor was accidentally exposed, so a partial pulpotomy was performed.
First Session
For the stepwise excavation, isolation with a rubber dam was performed prior to the removal of the infected tissue in the whole extension of the surrounding walls, with the aid of Nos. 3 and 4 rounded stainless steel burs at low speed. The disorganized dentin of the axial walls was removed with manual excavators (Figure 4). A 1-mm layer of calcium hydroxide paste was applied on the axial walls, and a GIC provisional restoration was performed; GIC was inserted with a syringe to avoid the incorporation of air bubbles into the material, thus, enabling better sealing. The option for a GIC relied on its good sealing properties, allowing more favorable conditions for the pulp-repairing activity.
The partial pulpotomy was performed for tooth No. 7 due to the pulp exposure during the caries removal procedures (Figure 5). The superficial contaminated pulp tissue was removed with a No. 1012 spherical diamond bur at high speed with water cooling to allow a better reparative response. This procedure was limited to removal of the infected dentin and damaged pulp tissue, removing the injured odontoblast cell layer. During this step, the remaining pulp tissue was analyzed and found to have good consistency and abundant red bleeding (Figure 6). After the pulpotomy, a solution of calcium hydroxide was used for irrigation along with a sterile cotton pellet to achieve hemostasis and disinfection. After hemostasis, the tooth was treated with direct pulp capping: the exposed area was covered with calcium hydroxide powder (Figure 7) and calcium hydroxide cement (Figure 8). The cavity was provisionally restored with the use of a restorative GIC (Figure 9).
Second Session
Ninety days after the first session, clinical and radiographic examinations were performed, showing normal pulp response, absence of spontaneous pain, and no evidence of apical pathology in all teeth. Radiographic evaluation of tooth No. 7 showed the presence of a mineralized barrier (Figure 10).
Once the maintenance of pulp vitality was verified, esthetic restorations of the teeth were performed. Initially, the teeth color shade was selected with the aid of a commonly used shade guide. After the isolation with a rubber dam, complete removal of the decayed dentin was performed in the teeth that received the stepwise excavation. The clinical verification of the presence of the mineralized barrier was performed in the maxillary lateral incisor with the aid of a disinfected gutta-percha cone, compatible with the diameter of the cavity. The authors recommend this procedure, because it allows the clinician to verify the formation of a mineralized barrier without compromising this critical area or causing a new exposure of the pulp tissue to the oral environment (Figure 11). After this, all teeth were treated with an indirect pulp capping technique. To obtain esthetics and functionality, beveling of both buccal and lingual surfaces was performed with No. 3118 diamond burs (Figure 12).
After the cavity preparation, calcium hydroxide cement and a lining with resin-modified GIC were employed for protection of the pulp-dentin complex (Figure 13). Then the enamel and dentin were conditioned with 37% phosphoric acid for 30 seconds and 15 seconds, respectively, followed by the application of the adhesive system according the manufacturer’s guidelines (Figure 14).
The insertion of nanohybrid composite resin was performed with the stratified technique to mimic teeth’s different colors and shades. First, an opaque (saturated chroma) layer was employed, followed by translucent layers simulating buccal and proximal enamel (Figure 15). Restoration excesses were removed with a No. 12 scalpel blade and No. 7214 multi-laminated burs, and an occlusion adjustment was made.
After 7 days, final finishing and polishing were performed using abrasive discs (Figure 16), multi-laminated burs, abrasive rubber points, and, finally, a felt disk with 40-μm diamond paste (Figure 17 and Figure 18). The results could be observed after 200 days (Figure 19), demonstrating the absence of a pathologic lesion in the apical region of the lateral incisor with an esthetic favorable condition, gingival health reestablishment, and pulp vitality maintenance.
Conclusion
This case report showed different conservative approaches capable of preserving tooth vitality through removal of total or a greater part of the bacteria, their components, and breakdown products from dentin matrix, allowing better interaction between the material and dental pulp.
The fundamental point is to recognize that there are different treatments that are dependent on the lesions’ depths. Thus, the philosophy behind such approaches is the advantages of tooth vitality associated with the absence of signs and symptoms of irreversible pulpitis, pulpal necrosis, and/or apical pathology. Finally, yet most importantly, adequate sealing of the instrumented cavity is essential in the different clinical stages to ensure maintenance and healing of the pulp tissue, in a bacteria-free environment.
About the Authors
Carlos Andres Villavicencio Espinoza, DDS, MSc, PhD
PhD candidate
Department of Restorative Dentistry
Endodontics and Dental Materials
Bauru School of Dentistry - University of São Paulo
Bauru, São Paulo, Brazil
Juan Fernando Ordoñez Aguilera, DDS, MSc
Department of Restorative Dentistry
Endodontics and Dental Materials
Bauru School of Dentistry - University of São Paulo
Bauru, São Paulo, Brazil
Private Practice
Equador, Brazil
Fabio Antonio Piola Rizzante, MSc, PhD
PhD candidate
Department of Restorative Dentistry
Endodontics and Dental Materials
Bauru School of Dentistry - University of São Paulo
Bauru, São Paulo, Brazil
Rafael Massunari Maenosono, MSc, PhD
PhD candidate
Department of Restorative Dentistry
Endodontics and Dental Materials
Bauru School of Dentistry - University of São Paulo
Bauru, São Paulo, Brazil
Eduardo Batista Franco, MSc, PhD
Associate professor
Department of Restorative Dentistry, Endodontics and Dental Materials
Bauru School of Dentistry - University of São Paulo
Bauru, São Paulo, Brazil
Sérgio Kiyoshi Ishikiriama, MSc, PhD
Assistant professor
Department of Restorative Dentistry
Endodontics and Dental Materials
Bauru School of Dentistry - University of São Paulo
Bauru, São Paulo, Brazil
Queries to the authors regarding this course may be submitted to authorqueries@aegiscomm.com.
Referencess
1. Stanley HR. Pulp capping: conserving the dental pulp—can it be done? Is it worth it? Oral Surg Oral Med Oral Pathol. 1989;68(5):628-639.
2. Ricketts DNJ, Kidd EAM, Innes N, et al. Complete or ultraconservative removal of decayed tissue in unfilled teeth. Aust D J. 2007;52(3):252-253.
3. Bjørndal L, Reit C, Bruun G, et al. Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci. 2010;118(3):290-297.
4. Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol. 1963;16:969-977.
5. Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 2011;37(5):581-587.
6. Stanley HR, Lundy T. Dycal therapy for pulp exposures. Oral Surg Oral Med Oral Pathol. 1972;34(5):818-827.
7. Maltz M, Alves LS. Pulp capping material is an important prognostic factor for direct pulp capping in permanent teeth. J Evid Based Dent Pract. 2013;13(3):117-119.
8. Nosrat A, Seifi A, Asgary S. Pulpotomy in caries-exposed immature permanent molars using calcium-enriched mixture cement or mineral trioxide aggregate: a randomized clinical trial. Int J Paediatr Dent. 2013;23(1):56-63.
9. Nosrat IV, Nosrat CA. Reparative hard tissue formation following calcium hydroxide application after partial pulpotomy in cariously exposed pulps of permanent teeth. Int Endod J. 1998;31(3):221-226.
10. Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: a preliminary report. Int Endod J. 2003;36(3):225-231.
11. Pereira JC, Stanley HR. Pulp capping: influence of the exposure site on pulp healing—histologic and radiographic study in dogs’ pulp. J Endod. 1981;7(5):213-223.
12. About I, Murray PE, Franquin JC, et al. The effect of cavity restoration variables on odontoblast cell numbers and dental repair. J Dent. 2001;29(2):109-117.
13. Matsuo T, Nakanishi T, Shimizu H, Ebisu S. A clinical study of direct pulp capping applied to carious-exposed pulps. J Endod. 1996;22(10):551-556.
14. Leksell E, Ridell K, Cvek M, Mejàre I. Pulp exposure after stepwise versus direct complete excavation of deep carious lesions in young posterior permanent teeth. Endod Dent Traumatol. 1996;12(4):192-196.
15. Stanley HR, White CL, McCray L. The rate of tertiary (reparative) dentine formation in the human tooth. Oral Surg Oral Med Oral Pathol. 1966;21(2):180-189.
16. Hilton TJ. Keys to clinical success with pulp capping: a review of the literature. Oper Dent. 2009;34(5):615-625.
17. Maltz M, Oliveira EF, Fontanella V, Carminatti G. Deep caries lesions after incomplete dentine caries removal: 40-month follow-up study. Caries Res. 2007;41(6):493-496.
18. Ricketts D. Management of the deep carious lesion and the vital pulp dentine complex. Br Dent J. 2001;191(11):606-610.
19. Hayashi M, Fujitani M, Yamaki C, Momoi Y. Ways of enhancing pulp preservation by stepwise excavation—a systematic review. J Dent. 2011;39(2):95-107.
20. Svizero NR, Bresciani E, Francischone CE, et al. Partial pulpotomy and tooth reconstruction of a crown-fractured permanent incisor: a case report. Quint Int. 2003;34(10):1-9.
21. Cvek M. A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endod. 1978;4(8):232-237.
22. Haskell EW, Stanley HR, Chellemi J, Stringfellow H. Direct pulp capping treatment: a long-term follow-up. J Am Dent Assoc. 1978;97(4):607-612.
23. Ghoddusi J, Forghani M, Parisay I. New approaches in vital pulp therapy in permanent teeth. Iran Endod J. 2014;9(1):15-22.
24. Asgary S, Ahmadyar M. Can miniature pulpotomy procedure improve treatment outcomes of direct pulp capping? Med Hypotheses. 2012;78(2):283-285.
25. Nahsan FP, Mondelli RF, Franco EB, et al. Clinical strategies for esthetic excellence in anterior tooth restorations: understanding color and composite resin selection. J Appl Oral Sci. 2012;20(2):151-156.
26. Asgary S, Ahmadyar M. Vital pulp therapy using calcium-enriched mixture: an evidence-based review. J Conserv Dent. 2013;16(2):92-98.