You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Despite advances in preventive dentistry, edentulism remains a significant public health problem worldwide. In the United States, although the rate of edentulism is decreasing every decade, the elderly population is rising so rapidly that the adult population in need of one or two complete dentures will actually increase from 33.6 million adults in 1991 to 37.9 million adults in 2020.1 The total number of edentulous arches is estimated at 56.5 million in 2000, 59.3 million in 2010, and 61 million in 2020.1
According to Allan et al,2 patients with dentures have shown minimal improvement in their quality of life when compared to those with implant treatment. These same patients remain unhappy with their dentures due to poor denture retention and stability, pain, denture sores, and difficulties in eating.3,4 Locker4 has reported that edentulism can lead to impairment, functional limitations, and physical, psychological, and social disabilities and handicap. Implant-supported prostheses have been shown to markedly improve the quality of life of edentulous patients compared with conventional dentures.5-7
Immediate loading for full-arch implant-supported prostheses in both the maxilla and mandible has been reported as a predictable procedure.8-11 In addition, the literature reveals excellent success rates with immediately loaded fixed prosthetic reconstructions8,12-15 with long-term follow-up.16,17 These same immediately loaded, fixed, full-arch prostheses for maxillary and mandibular edentulous patients have been associated with a high level of patient satisfaction with regard to esthetics, phonetics, comfort, and functionality.2,9,10,18-21 Malo et al18 introduced the All-on-4® treatment concept that involves immediate loading of a full-arch fixed prosthesis secured with 4 implants in a maxilla or mandible. Two implants are placed anteriorly, and 2 angulated implants are placed in the posterior region. These longer, tilted implants allow for optimal implant distribution, anterior-posterior (A-P) spread, and bone-to-implant contact, and serve to minimize cantilever length. In addition, these angled posterior implants avoid key anatomic structures and are able to engage remote areas of good-quality bone for excellent primary stability. In the maxilla, the use of these implants typically precludes sinus grafting. In the mandible, they facilitate optimal bone anchorage without violating the mental neurovascular bundles.
The All-on-4 treatment concept requires certain inclusion criteria, which include medical stability of the patient, sufficient bone quantity and quality, and adequate primary implant stability. A cone-beam computed tomography (CBCT) and clinical evaluation that is performed comprises a traditional prosthetic-based approach for edentulous-arch fixed reconstruction. This involves an assessment of the following: smile line, transition zone of the maxillary alveolar ridge and prosthesis, facial flange requirements for lip support, and the vertical dimension of occlusion (VDO). The intraoral examination includes evaluating incisal edge position, interarch relationship, restorative space, and soft-tissue quality and quantity, as well as assessment for pathology. In the maxilla, the surgical protocol includes placement of 2 posterior tilted implants anterior to the sinus, typically at an angle of up to 45°. In the mandible, the posterior implants are positioned in the bicuspid region and are also tilted anteriorly 30° to 45° in order to avoid the mental foramen and neurovascular bundle. Two implants are then placed in the anterior region of either the maxilla or mandible and are usually axial. Minimal insertion torque for loading is 35 Ncm, and all implants are placed freehand with the use of a prosthetic guide and/or a malleable Malo guide. Transmucosal abutments are placed (typically 30° posterior, 0° or 17° anterior), and soft-tissue closure is then accomplished.
The prosthetic protocol usually involves multi-unit copings placed onto the abutments, which are then splinted with rigid wire and low-shrinkage autopolymerizing resin. This is followed by an open-tray impression with a rigid vinylpolysiloxane (VPS) material to capture both the implant and soft-tissue positions. The laboratory then completes the denture conversion, and the prosthesis is secured to the multi-unit abutments.
Since the introduction of the All-on-4 treatment concept, restorative teams have attempted to improve upon the procedure to increase accuracy, efficiency, and predictability. The immediate extractions (for a dentate arch), freehand bone reduction, and placement of the implants, along with the conversion of an immediate denture to accept the implant abutments, need to become more precise and predictable in order to reduce chairtime and increase convenience for the patient.
This article reviews the rationale, techniques, and advantages of a guided full-arch immediate-function treatment modality that includes placement of a prefabricated, bar-supported, monolithic polymethyl methacrylate acrylic (PMMA) prosthesis for edentulous and terminal dentition patients. The fully digital and automated approach includes: acquisition of patient data and digital records; patient-specific anatomical reconstruction and image fusion (PSARIF); software-driven interdisciplinary treatment planning; virtual extractions; ostectomy; and prosthetic design. Also described will be surgical and prosthetic sequence, laboratory validation, materials, and occlusal management of both the provisional and final prostheses. Total patient appointments for this protocol—especially for final prosthesis fabrication—are minimized compared to the conventional All-on-4 conversion protocol.
Protocol Stages
Digital records—Five recorded items are needed to initiate a case for this fully guided prosthetic protocol. First, clinical digital photographs are obtained to communicate the patient’s facial anatomy as it relates to the existing dentition, occlusion, orthodontic arch position, and tooth shade. The photographs are also used to generate a facially driven treatment plan and digital facebow. Secondly, an occlusal bite registration is obtained using an impression material with the patient in maximum intercuspal position. Next, full-arch impressions are made via an intraoral scanner or manually with PVS material. Fourthly, the patient is scanned in the CBCT machine wearing the bite registration. Lastly, the digital dental laboratory slip is completed online. The CBCT data and clinical photographs are uploaded to the laboratory at this time from a link in the online form.
Patient-specific anatomical reconstruction and image fusion (PSARIF)—The use of powerful software tools in cosmetic and reconstructive surgery can empower dental professionals to create facially driven treatment plans and guided surgery in a 3D environment. The patient’s unique tooth and soft-tissue anatomy are captured using an intraoral scanner, or with stone models from a conventional PVS impression, which are digitized via a desktop scanner. This digital 3D data set is then merged with the underlying 3D bone structure taken from the CBCT scan relative to one another, forming a complete 3D, patient-specific data set of hard and biomechanical relationships, thus creating the foundation for accurate 3D planning (Figure 1).
Software-driven interdisciplinary virtual workup—The fused patient 3D data sets are then ready for prosthetic and surgical planning based on the digital set of clinical photographs taken at appointment No. 1. An interdisciplinary team web meeting that includes the restorative dentist, surgeon, and laboratory technician is then scheduled to fully discuss the treatment plan. The surgeon will have performed a comprehensive clinical and CBCT-based sequential digital diagnostic evaluation prior to this meeting. Facially driven treatment principles include, but are not limited to: 1) facial and dental midline; 2) occlusal plane; 3) VDO; 4) force factors; 5) cantilever elements; 6) A-P spread; 7) bone volume and density; 8) implant and abutment selection and placement; 9) screw-access holes; 10) path of prosthesis insertion; 11) bone reduction; 12) discussion and virtual implementation of provisional and definitive prosthetic materials. Implants, abutments, and all other pertinent parts are then ordered for the patient-specific digital treatment plan.
Manufacturing: milling and rapid prototyping of the apparatus—Once the planning session is concluded, the finalized data sets are manufactured with additive and subtractive manufacturing machines. The body of the provisional is milled from a monolithic PMMA material, and a support bar is milled out of medical-grade titanium. All items are manufactured, inspected, and assembled in the dental laboratory for the final fit, finish, and artisan work.
Laboratory validation—The production of all finished parts, pieces, and prostheses is quality controlled according to the surgical reports and validated by the quality-control team using dry model surgery techniques developed by nSequence® Guided Prosthetics™ (nSequence Center for Advanced Dentistry,nsequence.com) to ensure that the ostectomy, as well as every osteotomy site, is accurately planned. The surgical report is followed on dry patient models (Figure 2). These steps are necessary to determine if the desired result in the surgical and prosthetic workflow will equal the digital workup that was done in the implant-planning software. This process is intended to remove all guesswork from the procedure.
Surgery and insertion—The surgical technique begins with the validation of the original occlusal bite registration. A clear splint is made to confirm the bite and is tried in the mouth before anesthetizing the patient. Once the original bite is confirmed, the tissue is reflected, leaving the teeth and bone exposed to the borders, which are determined during the virtual-planning session. The teeth are extracted, and the proprietary nSequence® bone foundation guide™ is set and fixed in place with anchor pins. Prior to pin fixation, the specific location of the bone foundation guide is verified with a bite index and the opposing arch (Figure 3). The guide struts are then removed, and the intended ostectomy is completed to the level of the guide.
At this point the bone is ready to receive the implants. The surgical guide is pin indexed onto the bone foundation guide. Next, the appropriate surgical drilling sequence is followed to complete the osteotomies for implant placement. The implants are then loaded with the guided surgery mounts and placed through the guide to the prescribed and predetermined trajectory, depth, and rotation. The implant mounts and surgical guide are removed, and transmucosal abutments are placed along with pre-cut temporary cylinders. These multi-unit abutments are preselected for height and angulation as per the digital and clinical evaluation. After each one is placed, the prosthesis is positioned to verify proper position and angulation. The copings have also been precut to the correct horizontal dimension for proper fit with the prosthesis. A silicone spacer is positioned onto the bone foundation guide to position the prosthesis at the correct vertical and centric relationship and to preserve the predetermined tissue height. This is done in lieu of a rubber dam to prevent locking in the prosthesis. The long-term provisional (LTP) is then coated with a thin layer of petroleum jelly and placed over the temporary cylinders with a clear occlusal guide to lock in the occlusal position during the pickup process. The patient is instructed to bite into the occlusal registration, and flowable composite material is placed into the facial and buccal holes to pick up the prosthesis to the temporary cylinders (Figure 4).
The composite is then light cured. No conversion is necessary due to the precise planning of the implants as they relate to the finished LTP. The bridge is then unscrewed from the multi-unit abutments and contoured with acrylic out of the mouth (Figure 5 and Figure 6). Soft-tissue closure is accomplished using 4-0 vicryl suture. Minimal time is required for this step due to the accuracy of the pre-planning and guides.
Clear duplicate pickup—The next step is to repeat the pickup process with a clear duplicate of the LTP with a new set of temporary copings. The purpose of the clear duplicate is to record the dental implants at abutment level, maintain the patient’s vertical and centric relationships, and translate the esthetic and orthodontic positions of the LTP. The clear duplicate replaces the appointments needed for an open-tray abutment-level impression, verification jig, bite block, and wax try-in all at the time of implant surgery and provisionalization.
After the clear duplicate has been used to pickup the second set of pre-cut temporary cylinders (Figure 7), the dental laboratory technician can then pour up a new abutment-level soft-tissue master cast using abutment-level laboratory analogs and the same bite registration used to pick-up the clear duplicate in the mouth to remount the dental arch to the opposing arch on the original articulator. This allows the laboratory to proceed to the definitive prosthesis, or at the very least, mill the final titanium bar and move forward with a wax try-in with teeth.
Occlusal management—Immediate implant placement and provisionalization offer a potential for premature loading, which could prevent osseointegration. The LTP occlusal contacts can be adjusted to the opposing arch and will produce simultaneous bilateral contact and group function in eccentric movements to help spread the occlusal forces evenly across the arch form.
Final prosthesis wax try-in with denture teeth and titanium milled bar—Using the clear duplicate protocol at stage 1 implant surgery eliminates the need for a conventional abutment-level impression that would normally be indicated at the scheduled patient appointment time. Instead, the final milled titanium bar and denture teeth set in wax on the clear duplicate base is created in advance. At this time the final fit, function, phonetics, esthetics, and tissue contours are checked and recorded.
Final prosthesis delivery—The definitive prosthesis is delivered at this patient appointment. It can be made of milled zirconia or of denture teeth and acrylic on a milled titanium bar in addition to other prosthetic designs and materials as per the clinician’s preference.
Case Presentation
This guided full-arch immediate-function treatment modality is well-demonstrated with the following patient. A 62-year-old man presented with a maxillary complete denture and mandibular removable partial denture (RPD) that he had worn for 10 years. He was dissatisfied with the mobility of his dentures and expressed strong interest in having permanent teeth.
A thorough clinical and CBCT sequential digital diagnostic radiographic evaluation revealed a moderately atrophied edentulous maxillary arch and partially dentate mandible with severe periodontal involvement of the remaining teeth. The clinical evaluation included information regarding lip length and support, existing tooth position within the denture and natural teeth, occlusion, restorative space, and phonetics. It also revealed adequate restorative space present to avoid bone reduction and to allow for a flapless approach to the maxilla, while the mandible would be treated with full flap reflection and alveolectomy. A graftless solution was then presented to the patient that included full-arch immediate teeth in both the maxilla and mandible, all delivered via a fully guided immediate-function approach at one appointment that would include placement of prefabricated, monolithic PMMA bar-supported maxillary and mandibular fixed provisional prostheses.
The patient was scheduled for diagnostic records that included clinical digital photographs, full-arch impressions, and bite registration, along with CBCT scans with the bite registration in place. Fiduciary markers were placed into the existing maxillary denture (Figure 8), which was then scanned separately as per the dual-scan protocol. The denture, which was deemed appropriate in terms of esthetics, phonetics, tooth position, and VDO, was hard relined to provide stability for accurate recording. The DICOM data sets and clinical photographs were then uploaded to the laboratory using a digital form.
In the laboratory the patient’s digital 3D data set was then merged with the underlying 3D bone structures taken from the CBCT scan relative to each other, forming a complete 3D patient-specific data set. This was accomplished by fusing the digitized impressions, bite, and clinical photographs, together with the underlying 3D bony anatomy from the CBCT scan, to form a complete data set of hard tissue, soft tissue, and biomechanical relationships.
This fused data set served as the foundation for a virtual online interdisciplinary meeting that included the surgeon, restorative dentist, and laboratory technician. The virtual workup was based on all the assembled digital and clinical data (Figure 9 through Figure 12), and allowed for a true collaborative accountability22 among the respective clinicians and laboratory personnel. The treatment plan was then formulated among all team members and included optimal implant size, location, and angulation, as well as implant-supported immediate fixed maxillary and mandibular PMMA prostheses with bar that would be worn for 5 to 6 months prior to fabrication of the final fixed hybrid prostheses. A flapless approach with 5 implants was planned for the maxilla, and a flapped approach with alveolectomy and placement of 6 implants was planned for the mandibular arch. The patient was seen for final case presentation, informed consent, prescriptions, and scheduling the date of surgery.
The next appointment was for the planned surgery. The patient was appropriately sedated with intravenous medications, and local anesthesia was administered in both arches. The maxilla was treated first. A surgical guide was placed over the edentulous maxillary arch and secured with 3 fixation pins while using a bite registration against the opposing natural teeth and RPD to verify its appropriate 3D position (Figure 13). A fully guided flapless protocol was used with the appropriate drilling sequence to place 5 NobelActive™ implants (Nobel Biocare, nobelbiocare.com), one each in the following sites: right second bicuspid, right cuspid, right central incisor, left lateral incisor, and left second bicuspid. All implants were placed with insertion torque values varying from 35 Ncm to 45 Ncm. The surgical guide and implant mounts were then removed and the preselected multi-unit abutments were placed and torqued into position according to manufacturer’s recommendation. Periapical radiographs were used to verify full seating of all abutments. Pre-cut temporary cylinders were then placed into the multi-unit abutments, and after access-hole block out, the prefabricated, bar-supported PMMA bridge was positioned over the cylinders with a silicone gasket in place. Next, a bite index was used to verify accurate positioning of the bridge. The prosthesis was then luted to the temporary abutments by injection of flowable composite via previously drilled buccal flange-access holes (Figure 14). The prosthesis was unscrewed, cleaned, and contoured with acrylic out of the mouth, and soft-tissue closure was accomplished using 4-0 vicryl suture. The maxillary bridge was then screwed into place with a bite confirmation guide against the mandibular dentition (Figure 15 and Figure 16).
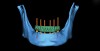
The remaining mandibular teeth were then extracted after full lingual and buccal flap reflection. The mandibular bone foundation guide was placed and indexed with fixation pins with a bite registration in place opposing the maxillary hybrid prosthesis (Figure 17). Next, appropriate alveolectomy was performed, followed by indexed placement of the surgical guide onto the bone foundation guide. Again, a fully guided digital protocol with appropriate drilling sequence was used to allow for placement of 6 NobelActive implants in the following sites: left first molar, left first bicuspid, left lateral incisor, right lateral incisor, right first bicuspid, and right first molar (Figure 18). All implants were placed with insertion torque values that ranged from 35 Ncm to 60 Ncm. The sole exception was the left first molar site implant, which had a 20-Ncm reading and was not loaded until the final prosthesis was fabricated. Next, the surgical guide and mounts were removed, preselected multi-unit abutments were placed, and periapical radiographs were taken to verify abutment implant fit. Temporary copings were placed, and the prefabricated petroleum jelly-coated PMMA hybrid prosthesis was seated with a silicone gasket. A pickup was done with flowable composite syringed through previously drilled buccal flange holes. The prosthesis was then removed, cleaned, and contoured with acrylic. Once again, soft-tissue closure was accomplished using 4-0 vicryl suture. Next, the bridge was secured to the copings and a slight bite adjustment was made (Figure 19 through Figure 22). The patient then returned for follow-up visits at 1 week, 2 weeks, 1 month, and 4 months for bite adjustment and supportive care prior to fabrication of the final prostheses.
The final restorative phase of treatment was initiated after 5 months of healing and stabilization of hard and soft tissues. The procedural steps within the protocol were designed to minimize the time and number of appointments and maximize the accuracy produced in the provisional restorations. Three appointments were necessary to allow for seating of the final prostheses, which consisted of a maxillary full-arch monolithic zirconium screw-retained bridge (Prettau® Bridge, PrettauLab, prettaulab.com) and a mandibular full-arch screw-retained bridge constructed of acrylic with denture teeth and a milled titanium substructure (Figure 23).
Discussion
Inherent in digital technologies for full-arch guided implant surgery and immediate fixed prosthetic reconstruction is the need for each of the multiple disciplines involved to participate in the collaborative goal of an optimized reverse-engineered implant and prosthetic treatment plan.23 Diagnostic CBCT imaging, intraoral and extraoral optical imaging systems, 3D CBCT interactive implant planning software, implant surgical guides, implant systems and prosthetic abutments, and CAD/CAM laboratory manufacturing technology all are making advances that potentiate improved case results.24-28
Two-dimensional (2D) diagnosis with freehand surgical application and conversion of an immediate denture are the hallmarks of the All-on-4 approach as presented by various authors.9,10,12,18-21,29-34 Inherent in this system are the inaccuracies of 2D radiographic diagnosis and planning, prosthetic compromise and complications, and clinical success directly proportional to operator skill, experience, and technique variables.
The ability to accurately and predictably pre-plan the implant positions relative to the ideal dentofacial-based titanium-reinforced prosthesis has preemptive advantages over the status quo reactive freehand conversion of a nonreinforced immediate denture. One notable benefit of this guided protocol could arguably be for the patient as well as the dental team. The level of strength and esthetics provided by the two-piece construction of a titanium milled bar with a PMMA bridge overlay—independent of the dental implant abutments—allows for a custom patient-specific passive fit at stage 1 implant surgery. Therefore, the patient is not subject to long hours of waiting as with the conversion technique. In addition, patients leave the surgical experience with the confidence of knowing they have a “real bridge” in their mouths that was specifically designed for their surgical case. Moreover, the dentist need not be concerned about unnecessary patient appointments to repair denture teeth that have fallen out of the denture as a result of functional force factors, or early fractures of the converted denture base—both common problems when attempting to fixate a denture that has been converted into a fixed hybrid without support from a stronger milled substructure to guard against masticatory, eccentric, and cantilever forces.
The freehand surgical technique currently employed in dentistry does have an advantage in patients with poor bone quality, because multiple implant osteotomies can be drilled into alternate implant sites until the desired torque has been attained to support an immediate fixed hybrid that will be custom fitted to various implant levels and abutment trajectories. One could also argue that the freehand technique has the advantage of allowing for better tactile proprioception for bone “feel” during the drilling and hand insertion sequence and implant placement. With fully guided protocols, the implants are placed through the master tubes by a “guided implant mount” that has tight tolerances to mate with the inner diameter of the master tube in the acrylic surgical guide, decreasing feel for the bone quality and density. Nevertheless, as dentists learn how to interpret the virtual DICOM data on bone quality, density, and volume as it relates to the actual biological bone quality, density, and volume, that knowledge will be applied to consistently achieve predictable initial torque and implant stability, ultimately resulting in the confidence to trust the fully guided surgical planning and implant placement.
Implant dentists striving for consistent clinical excellence in guided implant surgery and immediate full-arch fixed prostheses face myriad challenges, the most difficult of which are the integration and coordination of these multiple technologies and definitive communication of the clinical and virtual variables inherent in 3D digital implant and prosthetic software planning. Despite the accuracy of digital technology, the surgeon and prosthetic dentist are faced with objectively identifying, communicating, and maintaining the clinical prosthetic variables of centric relation, vertical dimension, midline, and patient-specific esthetic parameters of tooth position, smile line, and lip support. New dental laboratory technologies, communication with dental laboratories, and an inherent lack of experience in full-arch cases among all parties can further compromise excellence.
The nSequence-guided prosthetic protocol combines 3D CT-guided surgery with a definitive fixed immediate prosthesis, allowing implant clinicians to maximize the biomechanical and patient experience variables inherent in the All-on-4 philosophy. Compared with a freehand 2D approach, the precision, predictability, and consistency of this fully guided surgical and immediate fixed prosthetic method presents such clinical advantages as: 3D-precision digital implant planning and virtual surgical and prosthetic work-up; optimized interdisciplinary treatment planning and communication; maximization of All-on-4 engineering, implant lengths, diameter, and angulation, and available bone; CAD/CAM-definitive, screw-retained immediate fixed prosthesis; objective clinical control of 3D occlusal variables; fewer patient appointments and less chairtime; and excellent professional/medicolegal documentation.
Additionally, this protocol allows controlled 3D modification of bony anatomy to facilitate optimized implant planning, implant surgery, and prosthetic design via a precision stackable alveolectomy guide. Furthermore, this concept provides definitive control and accurate communication of virtual surgical planning, especially in immediate extraction cases in which alteration of the bony ridge is required.
Conclusion
Over the past 5 years, the authors have found that the use of the nSequence Guided Prosthetics fully guided system for both edentulous and terminal dentition patients, along with a comprehensive clinical and CBCT-based evaluation, has proven to be a more effective, efficient, and predictable protocol to provide full-arch immediate fixed teeth compared to conventional denture conversion techniques. Patient selection, accurate records, and detailed virtual planning are of paramount importance in utilizing this system. In total, 4 base patient appointments are needed from scan to delivery of the final prosthesis: 1) record taking; 2) surgery and provisionalization with clear duplicate protocol; 3) wax try-ins on titanium milled bars; and 4) final delivery of the definitive full-arch implant-retained prosthesis.
Clinical perfection in dental practice is the result of a sequence of simple repetitive steps performed precisely and sequentially in every patient case. As such, the goal for any new technological and procedural integration in clinical dental implant practice should be to reduce multiple therapeutic modalities to a series of precise reproducible steps that ensure consistency and predictability of the patient’s surgical and prosthetic treatment plan. This guided protocol is the practical manifestation of this goal, resulting in a seamless integration of multiple digital diagnostic, surgical, prosthetic, and laboratory modalities to achieve a predictable and consistent reverse-engineered fully guided surgery and immediate full-arch fixed prosthetic result.
Disclosure
Dr. Pikos is a consultant to Nobel Biocare and BioHorizons.
About the Authors
Michael A. Pikos, DDS
Adjunct Assistant Professor
Department of Oral & Maxillofacial Surgery
Ohio State University College of Dentistry
Carl W. Magyar, DDS
Private Practice
Lecanto, Florida
Daniel R. Llop, CDT
Inventor
Founder and President
Sequence Center for Advanced Dentistry
Reno, Nevada
Executive Director of CT Guided Surgery and Implant Technology
National Dentex Corp.
Palm Beach Gardens, Florida
References
1. Douglass CW, Shih A, Ostry L. Will there be a need for complete dentures in the United States in 2020? J Prosthet Dent. 2002;87(1):5-8.
2. Allen PF, McMillan AS. A review of the functional and psychosocial outcomes of edentulousness treated with complete replacement dentures. J Can Dent Assoc. 2003;69(10):662.
3. Heath MR. The effect of maximum biting force and bone loss upon masticatory function and dietary selection of the elderly. Int Dent J. 1982;32(4):345-356.
4. Locker D. Measuring oral health: a conceptual framework. Community Dent Health. 1988;5(1):3-18.
5. Turkyilmaz I, Company AM, McGlumphy EA. Should edentulous patients be constrained to removable complete dentures? The use of dental implants to improve the quality of life for edentulous patients. Gerodontology. 2010;27(1):3-10.
6. Awad MA, Lund JP, Dufresne E, Feine JS. Comparing the efficacy of mandibular implant-retained overdentures and conventional dentures among middle-aged edentulous patients: satisfaction and functional assessment. Int J Prosthodont. 2003;16(2):117-122.
7. Awad MA, Lund JP, Shapiro SH, et al. Oral health status and treatment satisfaction with mandibular implant overdentures and conventional dentures: a randomized clinical trial in a senior population. Int J Prosthodont. 2003;16(4):390-396.
8. Ioannidou E, Doufexi A. Does loading time affect implant survival? A meta-analysis of 1,266 implants. J Periodontol. 2005;76(8):1252-1258.
9. Malo P, de Araujo Nobre M, Rangert B. Implants placed in immediate function in periodontally compromised sites: a five-year retrospective and one-year prospective study [published correction appears in J Prosthet Dent. 2008;99(3):167]. J Prosthet Dent. 2007;97(6 suppl):S86-S95.
10. Khatami AH, Smith CR. “All-on-Four” immediate function concept and clinical report of treatment of an edentulous mandible with a fixed complete denture and milled titanium framework. J Prosthodont. 2008;17(1):47-51.
11. Bellini CM, Romeo D, Galbusera F, et al. Comparison of tilted versus nontilted implant-supported prosthetic designs for the restoration of the edentulous mandible: a biomechanical study. Int J Oral Maxillofac Implants. 2009;24(3):511-517.
12. Del Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws: a systematic review. Clin Implant Dent Relat Res. 2012;14(4):612-621.
13. Nkenke E, Fenner M. Indications for immediate loading of implants and implant success. Clin Oral Implants Res. 2006;17(suppl 2):19-34.
14. Esposito M, Grusovin MG, Willings M, et al. Interventions for replacing missing teeth: different times for loading dental implants. Cochrane Database Syst Rev. 2007;18(2):CD003878.
15. Sennerby L, Gottlow J. Clinical outcomes of immediate/early loading of dental implants: a literature review of recent controlled prospective clinical studies. Aust Dent J. 2008;53(suppl 1):S82-S88.
16. Schnitman PA, Wohrle PS, Rubenstein JE, et al. Ten-year results for Brånemark implants immediately loaded with fixed prostheses at implant placement. Int J Oral Maxillofac Implants. 1997;12(4):495-503.
17. Ericsson I, Randow K, Nilner K, Peterson A. Early functional loading of Brånemark dental implants: 5-year clinical follow-up study. Clin Implant Dent Relat Res. 2000;2(2):70-77.
18. Malo P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark system implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res. 2003;5(suppl 1):2-9.
19. Malo P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark system implants for completely edentulous maxillae: a 1-year retrospective clinical study. Clin Implant Dent Relat Res. 2005;7(suppl 1):S88-S94.
20. Malo P, Nobre Mde A, Petersson U, Wigren S. A pilot study of complete edentulous rehabilitation with immediate function using a new implant design: case series. Clin Implant Dent Relat Res. 2006;8(4):223-232.
21. Malo P, de Araujo Nobre M, Lopes A. The use of computer-guided flapless implant surgery and four implants placed in immediate function to support a fixed denture: preliminary results after a mean follow-up period of thirteen months [published correction appears in J Prosthet Dent. 2008;99(3):167]. J Prosthet Dent. 2007;97(6 suppl):S26-S34.
22. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 1: diagnostics, imaging, and collaborative accountability. Int J Periodontics Restorative Dent. 2006;26(3):215-221.
23. Pikos MA, Mattia AH. Implant surgery interventions: three dimensional reverse tissue engineering for optimal dental implant reconstruction. In: Jokstad A, ed. Osseointegration and Dental Implant. 1st ed. Ames, IA: Wiley-Blackwell; 2009:197-204.
24. Worthington P, Rubenstein J, Hatcher DC. The role of cone-beam computed tomography in the planning and placement of implants. J Am Dent Assoc. 2010;141(suppl 3):19S-24S.
25. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 3: stereolithographic drilling guides that do not require bone exposure and the immediate delivery of teeth. Int J Periodontics Restorative Dent. 2006;26(5):493-499.
26. Vrielinck L, Politis C, Schepers S, et al. Image-based planning and clinical validation of zygoma and pterygoid implant placement in patients with severe bone atrophy using customized drill guides. Preliminary results from a prospective clinical follow-up study. Int J Oral Maxillofac Surg. 2003;32(1):7-14.
27. Sarment DP, Sukovic P, Clinthorne N. Accuracy of implant placement with a stereolithographic surgical guide. Int J Oral Maxillofac Implants. 2003;18(4):571-577.
28. Campelo LD, Camara JR. Flapless implant surgery: a 10-year clinical retrospective analysis. Int J Oral Maxillofac Implants. 2002;17(2):271-276.
29. Penarrocha-Oltra D, Candel-Marti, E, Ata-Ali J, Penarrocha-Diago M, Rehabilitation of the atrophic maxilla with tilted implants: review of the literature. J Oral Implantol. 2013;39(5):625-632.
30. Francetti L, Romeo D, Corbella S, et al. Bone level changes around axial and tilted implants in full-arch fixed immediate restorations. Interim results of a prospective study. Clin Implant Dent Relat Res. 2012;14(5):646-54.
31. Menini M, Signori A, Tealdo T, et al. Tilted implants in the immediate loading rehabilitation of the maxilla: a systematic review. J Dent Res. 2012;91(9):821-827.
32. Del Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws: a systematic review. Clin Implant Dent Relat Res. 2012;14(4):612-621.
33. Weinstein R, Agliardi E, Fabbro MD, et al. Immediate rehabilitation of the extremely atrophic mandible with fixed full-prosthesis supported by four implants. Clin Implant Dent Relat Res. 2012;14(3):434-441.
34. Hinze M, Thalmair T, Bolz W, Wachtel H. Immediate loading of fixed provisional prostheses using four implants for the rehabilitation of the edentulous arch: a prospective clinical study. Int J Oral Maxillofac Implants. 2010;25(5):1011-1018.