You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Very little has changed in clinical technique for denture fabrication over the past few decades. Traditional five-appointment denture protocol remains the standard of care taught by many dental schools. This protocol requires meticulous attention to detail in order to provide clinical success, and its very nature can lead clinicians into a linear reasoning process during diagnosis and initial treatment for denture patients. However, variations in patient anatomy can be overlooked or misinterpreted when following a linear approach, and the Class II denture patient will respond unpredictably when treated in this manner. There is a compelling temptation to “correct” these patients to a Class I tooth-to-tooth relationship.
Successful impression taking is a prerequisite to develop a stable base upon which a denture can be fabricated. There is a misconception that denture stability and comfort is primarily dictated by adaptation of the denture base to the edentulous tissues. On its face, this is a legitimate idea. All dentures must conform to the basal seat upon which they function; however, functional dynamics, and thus stability, are dictated by many factors. Residual ridge dimension, occlusion scheme, patient adaptability, patient coordination, and interarch relationship play an equal or greater role in denture stability and ultimately patient satisfaction. This article explores the Class II (retrognathic) patient and the impact that jaw relation has on denture fabrication. This subject is poorly covered in the existent literature; most references are relatively old but are still considered relevant by today’s standards.
Class II jaw relationships regularly occur in the general population. While studies indicate varying percentages of occurrence, Profitt reports that 15-20% of the general population is Class II.1-2 Many Class II patients function in a different manner than the typical Class I patient. This functional difference is particularly important to understand when Class II patients become edentulous, as retrognathic patients tend to function over an extensive range of motion.3 They often posture into a forward rest position, which can be several millimeters anterior to the centric relation position of the mandible. Ricketts noted these acquired positions aid respiration and speech, and improve lip seal for swallowing.4 In addition, retrognathic patients often recognize that a forward jaw position improves their facial esthetics. The combined effect of function and facial esthetics can create a lifelong habitual behavior.5 In the opinion of this author, this habitual behavior is evidenced even upon loss of natural dentition. The underlying skeletal condition does not change, and as resorptive changes occur the arch forms become more Class II due to interarch differences in the bone loss process.6 The habitual rest position continues into the edentulous condition for the aforementioned reasons.
Centric relation is a non-tooth–dictated mandibular position. This most superior, anterior position of the mandible is well documented as a consistent reference for restorative dentistry.7 This bone-braced position, from which the arc of closure is initiated, provides maximum efficiency of mandibular closure during chewing function. Free access to this jaw position is necessary for a proper functioning denture occlusion. Occlusal prematurities to the arc of closure lead to denture instability and inefficiency of chewing. The relationship of centric relation to acquired rest position/acquired centric occlusion is of particular concern when treating the retrognathic patient.
Mandibular anterior denture teeth should be set to follow the shape of the residual arch form. These teeth should be set over the edentulous ridge.8 The relationship of tooth to ridge is important so as not to create cantilever forces upon incising food. This cantilever force increases with the distance that teeth are positioned away from the ridge, and these forces directly affect denture stability. Retrognathic jaw relationships typically require a moderate to possibly significant amount of overjet to satisfy this tooth-to-edentulous ridge relationship. As previously mentioned, many Class II patients exhibit a habitual jaw position that is anterior to initial contact in centric relation. Long overjet and habitual anterior rest position dictate the occlusal scheme for these appliances. Initial simultaneous contact in centric relation should occur on as many posterior teeth as possible, and the occlusal scheme must not restrict the patient’s ability to posture forward into his or her habitual jaw position. These factors contraindicate full anatomical denture teeth.
Steep cuspal inclines potentially limit the technician’s ability to provide balanced protrusive occlusion. Monoplane posterior teeth or semi-anatomic (20°) teeth are more appropriate when looking to avoid tooth interferences during excursive movements. These teeth are also easier to set into balanced occlusion. Balancing occlusal contacts are indicated during all excursions from centric relation. When the overjet is excessive, it is expected that lower anterior teeth will not be in contact in CR. These teeth will contact upon forward movement.
The occlusal schemes most cited in the literature are lingualized occlusion and monoplane occlusion.9 Both occlusal philosophies have merits and are widely reviewed in the literature. The lingualized occlusal relationship provides a predictable laboratory procedure and also a simplified remount and adjustment protocol for the dentist. The position of the facial maxillary molar cusps can be objectionable to patients with high esthetic demands; this is also the case with monoplane teeth. The lack of cusp definition gives a worn, old appearance to the dentition. Many Class II patients exhibit a steep Frankfort Mandibular plane angle. When combined with a steep condylar guidance, it can be difficult to achieve adequate protrusive balancing contacts with monoplane teeth. The 20° denture tooth can satisfy esthetic requirements on the maxillae and provide more opportunity to create balancing excursive contacts. It is imperative to understand that each case must be considered individually and no single occlusal scheme will work universally. Regardless of the selected occlusion, patients must have unrestricted access to centric relation10 and the freedom to posture forward into their habitual rest position. There is a temptation to cantilever lower teeth in such a way as to create a faux Class I appearance. This results in denture instability, but more importantly, it creates a limited envelope of Class II function. Inappropriate position of the lower anterior teeth leaves patients “locked in” to the occlusion and prohibits their ability to function within their habitual patterns. This restriction limits “normal” Class II function and leads to patient frustration and dissatisfaction.
Transitional treatment from failing dentition to treatment dentures is a complex, potentially frustrating experience for both patient and clinician. Failing dentitions may offer few clues as to appropriate incisal edge position, lip support, or vertical dimension of occlusion. Bite registrations taken with failing dentitions can be difficult to record in centric relation. Patient adaptation to collapsed, failing dentition makes jaw relation records suspect at best, particularly in regard to capturing centric relation, as patients will maintain a path of closure that protects the failing dentition. This protective mechanism, along with a habitual forward rest position, make the Class II patient even more unpredictable during the dentate to edentulous transition.11 The extensive range of motion exhibited by Class II patients only adds to this difficulty. This forward position can easily become an acquired maximum intercuspation occlusion with flaring of anterior teeth and loss of posterior support.
Case Presentation
A 58-year-old male presented in reasonably good general health. No contraindications to providing dental care were discovered. He was referred for evaluation for full mouth extraction and subsequent placement of a full upper denture and implant-retained lower denture. Intraoral examination revealed a failing dentition with loss of posterior supporting teeth and flared, supra-erupted anterior teeth; panoramic radiograph confirmed the failing dentition diagnosis. The patient exhibited a deep overbite and excessive overjet (Figure 1 through Figure 4). Upon interview, the patient approved the treatment for which he was referred. No intraoral contraindications to treatment were encountered. The treatment plan consisted of two distinct phases. A first phase of treatment was suggested to transition the patient from failing dentition to treatment dentures. A second phase of treatment six months later was recommended to provide definitive treatment. This plan would include implant treatment to stabilize the mandibular appliance.
Treatment records were accomplished, and impressions taken for custom tray fabrication. At a secondary records appointment, impressions were taken in custom trays, tentative bite records were taken in centric relation, protrusive bite records were taken, facebow transfer was done, and photography was shot in multiple views.
Initial case work-up was done at this second appointment. The patient was evaluated at rest position. Display of existing teeth was evaluated,12 and the incisal edge position was considered too long and facially flared. Centric occlusion was determined to be precisely repeatable. Manipulation to centric relation proved to be challenging and coincident with centric occlusion; this result was suspicious due to posterior collapse and flaring of anterior teeth. The facial profile of this patient was somewhat difficult to evaluate due to the beard that he had grown to conceal a “weak chin” and strong angle of mandible (Figure 5). Desired position of midline and tentative incisal edge position were identified using permanent marker drawing on natural teeth. This drawing was recorded with photography to communicate with the technician. A complete prescription was developed and sent to the laboratory along with the entire clinical product developed during the case workup. Photography is an often overlooked communication tool for working with the dental laboratory: Denture technicians can gain better insight into tooth relationships when viewing images of the patient, not just the stone casts (Figure 6 through Figure 8).
The laboratory was instructed to mount the case on a semi-adjustable articulator. Models were mounted with facebow transfer and bite records, and condylar inclination was adjusted with protrusive records. Mounted models were returned for evaluation and final design of treatment dentures. Study of the mounted models completed the diagnostic evaluation of the patient (Figure 9 and Figure 10): failing dentition, suspect occlusal relationship, and Class II jaw relationship were diagnosed. The loss of normal esthetic references was an additional complication for the treatment.
The treatment plan consisted of two distinct phases. A first phase was suggested to transition the patient from failing dentition to treatment dentures. Once teeth were extracted and immediate treatment dentures were delivered, a second phase of treatment six months later was recommended. This secondary treatment would consist of final definitive dentures based on findings developed during transitional phase of treatment. In addition, the mandibular denture would be retained with four implants in an immediate loading protocol.
Intended incisal edge positions were communicated to the laboratory based on intra oral evaluation (photographic) and on anthropometric averages13 (22 mm maxillary incisal edge, 18 mm mandibular from mucobuccal fold, and 8 mm facial to the incisive papillae).14 It was assumed that the vertical dimension of occlusion was inaccurate due to occlusal collapse and flaring of failed dentition, and VDO was opened one millimeter beyond existent occlusion. Initial tooth selection was based on existing central incisors in the failing dentition. Removing teeth segmentally maintained the adjacent references on the modified casts. Laboratory putty matrices were developed as a further reference to incisal edge modification. The laboratory was instructed to develop a Class II occlusal relationship with balanced occlusion in all excursions. 20° semi-anatomic denture teeth were ordered to develop reasonable esthetics and adequate cuspal inclines to provide balancing contacts but not so steep as to lock patient into centric relation. Teeth were set to prescribed relationship, and lingual cusps of maxillary first premolars were modified to allow non-interference in balance. Final setup was approved and then processed. The case was remounted and bite relationship confirmed prior to the surgical appointment (Figure 11). Modified casts were duplicated for manufacture of clear surgical guides (Figure 12): these guides were particularly important in the lower anterior region as implant placement was allowed for in the model modification that occurred prior to setting teeth (Figure 13).
Delivery of immediate treatment dentures was accomplished with minimal alveolectomy on the upper arch (Figure 14). The lower arch was reduced in vertical height in anticipation of the restorative space required by planned implant components. The clear surgical guide provided a precise means by which the surgeon could evaluate the amount of bone to remove. The immediate treatment dentures were delivered uneventfully; the patient was instructed to wear them continuously for 24 hours, at which time he was seen for a postoperative evaluation. Remount records were taken and dentures were articulator-mounted for minor occlusal adjustment. Intaglio adjustments were made to relieve sore spots and slight border overextension. Subsequent recall appointments consisted of further adjustments and eventual placement of a temporary reline material to provide ongoing tissue adaptation during healing.
The patient was very pleased with the esthetics of his treatment dentures but was plagued with insufficient denture stability and poor phonetics during the interim phase (Figure 15). It became evident over the course of postoperative care that one or more treatment assumptions were mistaken. The vertical dimension of occlusion was evaluated and accepted, and minor esthetic modifications, including midline correction, were noted. Stability and phonetics were the primary concerns requiring a solution. Clear duplicate dentures were fabricated from lab putty duplication jigs (Figure 16), and minor esthetic changes were identified (changes in esthetic corridors, midline marked). At this point, no solution for stability and phonetics was readily evident.
Modifying Treatment Assumptions
Transitional treatment dentures are an indispensable part of edentulous rehabilitation. The transition from dentate to edentulous requires a number of treatment assumptions. The unfortunate fact is that there is no way to do a preview try-in for an immediate delivery denture case, and it is unlikely that all the parameters for successful denture treatment will be met upon delivery of these appliances. The clinician must decipher what modifications must be made to the treatment assumptions in order to deliver a successful definitive prosthesis. One crucial finding in this case was discovered during the clear duplicate denture try-in. The clear appliances were adjusted for even pressure on intaglio surfaces, and a closed bite wash impression was taken in each appliance. At this point, occlusion seemed consistent with previously delivered treatment dentures. Upon further examination and bimanual manipulation,15 it was discovered that the initial treatment appliances had been fabricated in an acquired habitual jaw position. Centric relation was 4-5 mm posterior to the initial treatment denture occlusion. This finding was consistent with previously referenced literature regarding the difficulty in recording centric relation on Class II patients. The forward habitual posture of the mandible was exacerbated by the gradual deterioration of the patient’s dentition, and what was once a habitual rest position became the patient’s centric occlusion. Once the proprioceptive stimulus from multiple failing teeth was removed, the patient could be more easily manipulated into centric relation (Figure 17).
The clear duplicate denture technique provides an excellent platform with which to modify treatment assumptions. Esthetic concerns can be communicated to the laboratory by adding or removing acrylic, and midline communication can be precisely communicated. Border modifications are easily accomplished with new border molding procedures. Wash impressions provide a final impression upon which excellent tissue adaptation can be attained in the final appliance. The critical “missing element” of this case was discovered during the bite registration following all previously described steps. In effect, the just washed bases were very stable and lent themselves to successful mandibular manipulation into centric relation. The stable bases allowed placement of bite registration material and use of bimanual manipulation.
An alternate method of achieving this result would be through the use of a central bearing device.16 The central bearing device provides a consistent means by which one can identify centric relation. The device separates the posterior teeth and utilizes the deprogramming effect of having a single point of contact; the resultant gothic arch tracing pinpoints the location of centric relation.
The clear duplicate dentures with wash impressions, bite registration, protrusive record, facebow, and photographs were returned to the laboratory. A thorough written prescription was included with the clinical product. Printed photography with annotations was provided for the technician’s reference.
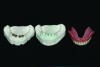
Impressions were beaded, boxed, and poured. Subsequent models were mounted on semi-adjustable articulator prior to separation. This ensures a totally accurate transfer of occlusal relationships prior to any possible distortion resulting from separation of the models. The facebow transfer and new bite registration records were used. Laboratory putty matrices were taken of the incisal edge position of the maxillary anterior region. Clear dentures were separated from models and retained for future reference. Stabilized baseplates were developed and a new wax set up was created using the existing maxillary incisal edge position and a completely new centric relation position. Lower anterior teeth were placed in appropriate position relative to the edentulous ridge and fully balanced occlusion was developed using a 20° semi anatomic denture tooth on the maxillary and a 0° tooth on the mandibular. The completed wax setup was returned for clinical evaluation and patient approval.
The wax try-in appointment was revealing, as the patient’s phonetics were immediately transformed from the original treatment dentures. Enunciation was crisp and sibilants were precise. Explanation for this dramatic change from the original treatment dentures is clear—the original was delivered in an anatomically undesirable position. The Class II speech pattern was inhibited by malposition of the original treatment denture occlusion (in advance of centric relation). This placed the lower central incisor in the wrong position for the patient to make sibilant sounds. Class II patients typically create S sounds in a different manner than a Class I.17 This tooth arrangement blocked the patient’s extensive range of motion and the preliminary treatment dentures effectively eliminated the patient’s ability to perform his lifelong acquired jaw movement and speech patterns. However, the new setup provided a solid occlusion based in centric relation and provided the freedom for his extensive range of motion (Figure 18).
The lower denture try-in was duplicated as a clear duplicate denture. A final confirmation of edentulous ridge to tooth position was completed. The implant system required 10 mm of restorative space for adequate support and clearance for the restorative components. Prosthetically driven implant placement provides the most predictable long- and short-term results.18 Desired implant locations were identified on the model. Then the clear denture was drilled with a 2 mm twist drill to simulate the surgical path of placement. Barium sulfate was placed into the guide channels (Figure 19). This appliance was then returned to the oral surgeon for cone beam survey, and scans revealed adequate bone volume in all four desired locations. The appliance was then converted to a surgical guide by removing the barium sulfate. The resulting 2 mm channel served to guide original surgical pilot drills.
Retentive abutments were simulated on the master mandibular cast following cone beam confirmation of locations. Clearance was waxed over the abutments to provide adequate clearance for subsequent clinical pick up procedures. This model was then duplicated (Figure 20) and the dentures were precision processed. Finally, the denture bases were characterized and made ready for delivery. The case was returned for delivery with dentures mounted on laboratory putty models, which could facilitate any remount procedures. The upper model was then mounted on a semi-adjustable articulator in the laboratory.
Due to meticulous surgical technique and adequate prosthetic planning and preparation, the delivery appointment was uneventful. Four implants were placed utilizing the previously described surgical guide. Immediately following the surgery, straight abutments were placed, precious alloy retentive elements were placed over the abutments, and clearance was confirmed for pickup procedures. A critical step in this procedure is to “tap” the retentive caps into place on the abutments to ensure total engagement. The retentive elements were picked up intraorally using an auto-mixing, self-curing composite material. The denture was removed and small discrepancies around retentive elements were filled with light-cured tissue color composite. Once the occlusion was evaluated and deemed acceptable, the patient was dismissed with strict instruction to leave the lower denture undisturbed for two weeks. Furthermore, the patient was instructed to remain on a soft diet for 3 weeks.
The first postoperative appointment was at 24 hours, at which the patient reported total satisfaction with the result and no issues with either appliance. Phonetic evaluation revealed crisp sibilants and clear enunciation. The second postoperative visit was performed at the end of the second week after surgery. The lower denture was removed for the first time (Figure 21) and the surgical sites were found to be healing well. No tissue impingements or denture sore spots were identified. A new centric relation bite record was taken and the dentures were remounted to refine the final occlusal relationship. Minimal adjustment was necessary. Patient response to the treatment was positive and enthusiastic.
Discussion
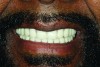
This case study presents the significant challenges inherent in treating the Class II retrognathic patient. The typical extensive range of function exhibited by this patient made it difficult to accomplish accurate and consistent jaw relationship records. This challenge combined with an existent failing dentition further complicated the process. This case demonstrates the value of treatment dentures. Treatment assumptions and anthropometric averages are often successful, however, they require confirmation. The treatment dentures are never intended to be the definitive solution: They are just what they are named, treatment dentures. They are a test-bed for the transition from the dentate to edentulous mouth restored with dentures. Modifications to the original treatment assumptions occurred during the clear duplicate denture impression appointment. Changes were reflected in the final wax try-in. The try-in appointment gives the necessary preview of the final definitive restorations. This patient exhibited a classic wide range of mandibular motion. Please note the exaggerated open mouth smile exhibited by the patient, his most comfortable and consistent smile. Again, this is another example of camouflaging behavior and increased range of motion seen with Class II patients.
Speech is a critical tool in the evaluation of tooth position and vertical dimension. This patient’s success directly followed his speech. Once given the freedom of motion and anterior tooth position in a Class II relationship, the patient’s satisfaction with the prostheses was remarkable. It certainly did not complicate matters to provide the implant retention of the lower appliance. Freedom to reach centric relation and balanced eccentric occlusion provided the patient with an efficient chewing solution (Figure 22 through Figure 24).
Acknowledgements
The author would like to thank the technicians at Drake Precision Dental Laboratories, Charlotte, NC. Their patience and attention detail was instrumental to the successful conclusion of this case.
References
1. Proffitt WR, Fields HW Jr, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13(2):97-106.
2. Harris JE. The heritability of malocculuison: implications for the orthodontic practitioner. In: Barrer HG, ed. Orthodontics: The State of the Art. Philadelphia, PA: University of Pennsylvania Press; 1981: 257-268.
3. Sperry TP. An evaluation of the relationship between rest position of the mandible and malocclusion. Angle Orthod. 1989;59(3):217-225.
4. Ricketts RM. Study of changes in temporomandibular relations associated with the treatment of Class II malocclusions. Am J Orthod. 1952;38:918-933.
5. Posselt U. Physiology of Occlusion and Rehabilitation. Oxford, England: Blackwell Scientific Publications; 1968.
6. Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: a mixed-longitudinal study covering 25 years. 1972. J Prosthet Dent. 2003;89(5)427-435.
7. Curtis TA, Langer Y, Curtis DA, Carpenter R. Occlusal considerations for partially or completely edentulous skeletal Class II patients. Part II: Treatment concepts. J Prosthet Dent. 1988;60(3):334-342.
8. Sowter JB. Dental:Laboratory Technology Prosthodontic Techniques. Charlotte, NC: University of North Carolina Press;1968: 57-78.
9. Clough HE, Knodle JM, Leeper SH, et al. A comparison of lingualized occlusion and monoplane occlusion in complete dentures. J Prosthet Dent. 1983;50(2):176-179.
10. Dawson PE. Evaluation, Diagnosis, And Treatment of Occlusal Problems. St. Louis, MO; CV Mosby Co.; 1989:28-32.
11. Drago CJ, Caswell CW. Prosthodontic rehabilitation of patients with Class II malocclusions. J Prosthet Dent. 1990;64(4):435-445.
12. Vig RG, Brundo GC. The kinetics of anterior tooth display. J Prosthet Dent. 1978;39(5):502-504.
13. Fayz F, Eslami A, Graser GN. Use of anterior teeth measurements in determining occlusal vertical dimension. J Prosthet Dent. 1987;58(3):317-322.
14. Sawiris MM. The role of anthropometric measurements in the design of complete dentures.
J Dent. 1977;5(2):141-148.
15. Dawson PE. Evaluation, Diagnosis, And Treatment of Occlusal Problems. St. Louis, MO; CV Mosby Co.; 1989:35-39.
16. Robbins JW. The use of a central bearing device for the dentulous patient. J Prosthet Dent. 1986;55(4):529.
17. Pound E. Utilizing speech to simplify a personalized denture service. J Prosthet Dent. 2006;95(1):1-9
18. Cooper LF, Limmer BM, Gates WD. “Rules of 10”—guidelines for successful planning and treatment of mandibular edentulism using dental implants. Compend Contin Educ Dent. 2012;33(5) 328-336.
About the author
Larry Holt, DDS
Director of Clinical Education and Research
Drake Precision Dental Laboratory
Charlotte, NC
Adjunct Faculty
UNC School of Dentistry
Chapel Hill, NC