You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Dentistry has not stood still. The new digital era is making a significant impact on the dental profession. The purpose of a digital radiography system is similar to that of the conventional system. The biggest difference is that images for a digital system are viewed and captured with a computer while conventional radiography captures its images on film that has to be processed with chemicals. The digital system can be used to expose periapical and bitewing films as well as panoramic and cephalometric films. More recent innovations include the use of digital CT scans and 3D imaging in the dental office similar to CT scans done in hospitals and medical imaging centers.1 The focus of this article will be the routine radiographs used in the dental office.
In the past decade, digital radiography has been gaining popularity and many offices are considering converting to digital radiography systems.2
The major obstacles to acceptance and general use of the technology included cost and the practitioner's lack of comfort with technology. It has been found that practice efficiency improves when a dental practice uses digital radiography.3
Digital radiography has a significant benefit over film in reducing the amount of radiation to which a patient is exposed. The reduction in radiation does not impact the diagnostic ability of digital images to provide for accurate diagnoses. Of note, when making radiographs with a digital system it is critical that the x-ray cone be as close to the face as possible to have correct exposures of sensors or phosphor plates. Always be certain the x-ray unit is set to the correct dosage and time for the image—anterior vs. posterior. Any very small changes in distance away from sensor or phosphor plate can have substantial negative effects on the diagnostic ability of the image.
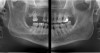
For the diagnosis of interproximal caries in posterior teeth, digital radiographic images have been shown to be equivalent to film.4 Also, for the diagnosis and evaluation of periodontal bone defects, digital images have been shown to be equivalent.5 One benefit of digital radiographs is the ability to use the software program to "process" the image (make digital adjustments to contrast, lightness and darkness, and use other tools) to better see conditions to make a more accurate diagnosis. Also, all digital radiographic programs offer a magnification tool to enlarge the image for an improved evaluation.6 Diagnosis and use of digital radiography during endodontic treatment has also become well accepted.7,8 Digital radiography through the use of digital panoramic units has improved diagnosis, and with the latest 3-D cone-beam technologies, allow for the use of extraoral imaging with excellent diagnostic potential (Figure 1).9,10 Digital radiography also provides an excellent patient education tool with the ability to use the computer monitor at chairside to better demonstrate conditions that have been diagnosed and possible proposed treatment.
Fundamentals of Digital Radiography
Because the purpose of a digital radiography system is the same as a conventional film x-ray, where do the differences exist within the dental office? For film x-rays, the dental office needs the film, film holders, intraoral (cone head) and extraoral (panoramic) x-ray units, film processor, film-processing chemicals, and a plan to dispose of the chemicals and the lead shielding present in film packets. In many cases digital x-rays use similar types of equipment with some differences in acquiring the digital image.
With digital radiography, film is replaced by an image-capture device, which is called an image receptor. Currently there are two types of systems for capturing the x-ray image. They are direct imaging systems, which include charge-coupled devices (CCD) and complementary metal oxide semi-conductor (CMOS/APS), and indirect imaging systems, which include photo-stimulable phosphor plates (PSP) and the use of digitally scanned, conventionally processed films that can be stored as a digital image in a computer hardware device. Scanning existing conventional films allows an office to convert to a digital system for radiography storage and retrieval purposes. It is important that the method of scanning will not degrade the image that has been digitized.11
While both types of systems can capture acceptable diagnostic images, there are advantages and disadvantages that can have a direct impact on the dentist, dental hygienist, and dental assistant. These differences relate to the method of image processing and the physical dimensions of the imaging-capture system. These advantages and disadvantages will be described later in this article.
CCD and CMOS/APS are basically solid-state sensors connected to a wire cable that attaches to a computer interface. Manufacturers have introduced wireless CCD/CMOS sensors similar to WiFi that computers use to access the Internet. The CCD, first invented in the 1960s, is the most commonly used sensor today. The CMOS/APS sensor is similar to the CCD sensor and is considered to be more durable and less expensive to manufacture. In basic terms, x-ray energy from the x-ray device exposes the sensor, which then converts the energy to a digital signal that is translated by the computer into an image that can be seen on the computer screen. This process occurs almost instantaneously.
One major problem with CCD sensors is their thickness and rigidity. Although the manufacturers provide for sensor holders similar to those used for positioning films, these sensors are more difficult and more time-consuming to place in a patient's mouth. Some patients will have difficulty tolerating the size and thickness of the sensor. This is especially true with pediatric patients. Also, care must be taken to not damage the cable. For infection control, the sensor is not autoclaved or disinfected, but rather barriers (plastic sleeves) must be used over the sensor and cable. If necessary, a sensor can be disinfected with ethyl alcohol. It is important that the dental staff and dentist follow the recommendations of each manufacturer. Sensors are expensive, ranging in cost from $4,000 to over $12,000 a sensor. Everyone in the office must be diligent in not abusing and misusing the sensors.
A PSP system uses thin plates similar in shape and size to that of conventional film.12 Patients tolerate their use intraorally at the same level as conventional film. PSP differs from the CCD and the CMOS/APS in that the images are produced in a two-step process. A reusable unwired sensor is used. The sensor is a flexible phosphor-coated plate containing rare earth elements. When the plates are exposed to the x-ray beam, they store the energy in the form of photons. Using a manufacturer's specified laser scanner, the PSP plates are processed in the laser-scanning unit. The plate is exposed to light released by the laser, which then transmits it as an electronic signal to the computer that is then converted to a visible digital image that can be seen on the monitor. The plates are reusable. They are discharged either by the scanner or by exposing them to a very bright light source. The plates must be stored in darkness to extend their time of usability. It is advisable to "process" the PSP plates in the laser scanner right after exposure. There have been reports of degradation of image quality if there is a delay in processing and over time of use.13,14 Typically a single PSP sensor costs approximately $30 to $40.
Infection control requires that the PSP be placed in a plastic pouch that is sealed from the oral fluids. The x-ray energy "exposes" the plate, leaving a latent image that is then taken to a processing device. The plastic pouch is discarded and the PSP is placed into a laser-scanning device that is part of a given manufacturer's system. Through the scanning process, the analog image is converted to a digital image for viewing on the computer monitor. Scanning may take from 30 to 90 seconds to process the image as compared to the almost instantaneous processing of the CCD/CMOS sensor.
The Digital Image
Resolution and Pixels
Digital images are typically viewed on a computer monitor. A digital image is composed of pixels. Pixel is an abbreviation for the two words "picture elements." A pixel is defined as one dot in the digital image. The image is composed of all the pixels that form the image and the image resolution is determined by the size and the number of pixels.
Gray Scale
Digital images captured by a sensor are displayed on the monitor in shades of gray (Figure 2). The grayscale displayed by the monitor is comprised of 256 distinct visible shades of gray even though some systems can contain up to 64,000 values.15 The human eye can only distinguish up to 32 shades of gray; this fact will be important later when the concept of image processing is presented. Each pixel in the digital image has a number ranging from 0 to 255. The radiation is registered when the sensor captures it. Maximum radiation is zero on this scale (pure black) and no radiation penetration (total radiopacity) is 255 (pure white).15 This radiation intensity is sent to the computer and stored. Dental professionals rely on the contrast of a radiograph to be able to detect disease processes; the longer the scale of contrast in the image, the easier it is to make a diagnosis. With the ability to enhance gray scales using the software that accompanies the sensor in an x-ray digital imaging system, a clinician may be better able to diagnose even subtle changes that may have been missed previously with conventional films.16-18
Computer Hardware
In most dental offices, the digital x-ray software will run faster with an upgraded computer system.8 Each digital radiographic manufacturer will recommend the minimal speed of microprocessor, hard drive storage size, computer RAM (Random Access Memory), graphic display card, processor speed, and monitor resolution for a computer to adequately run the imaging software. It is always a wise financial decision to purchase more computer speed, storage, and higher resolution imaging for the graphics card and monitor than the minimum that is recommended because as the software is updated, it may require a hardware upgrade if running on a minimal computer system. It is always less expensive in the long run to purchase hardware upgrades when initially purchasing the computer. The ideal today is at least 3 to 4 gigabytes of RAM, the memory in the computer that holds the data and programs that are currently running. The higher the RAM, the faster the computer will process images.
Storage is also important. In today's dental practice, office management software, an electronic patient record, digital radiographic images, and digital photographic images of the patient's oral conditions and treatment use a significant amount of digital storage space on a computer. It is advisable to purchase at least a 1-terabyte hard drive in the computer with an equivalent amount of storage on an external hard drive. When determining a hard drive, look not only at the amount of storage, but also at the speed of the hard drive (how fast the hard drive will access data). The faster the better—7,200 rpm is better than 5,400 rpm. When deciding on how you plan to store the images, have the manufacturer's representative make a recommendation for image storage and how to back up images so that they will not be lost if the computer has a malfunction. Each system may have different requirements.
With an optimal processor, RAM, hard drive, and additional hard drive storage, data can be input and retrieved in a reasonable time while patients are being treated. The current generation of laptops is almost comparable to desktop computer systems. In fact, it may be possible with a system to use the latest generation of computer tablets to look at radiographic images anywhere in the office using wireless access. Monitors used with computers have changed significantly in both resolution and cost. Today, LCD flat-screen monitors have become more affordable and are available in larger sizes. At a minimum, consider a 17-inch monitor, although the practice should have at least one 19-inch monitor to view and process x-ray images.
There will be times when it is beneficial to print the images, such as to send to a specialist the patient is being referred to or when requesting insurance reimbursement. Laser printers have come down in price in the past 2 years, and high-quality black-and-white and color laser printing provide a more cost-effective alternative to inkjet printers. For best image reproduction, follow the printer's guidelines for the paper that should be used for highest image definition.
Computer Software
Most digital radiology systems have their own proprietary software. As part of the purchase of the system, the manufacturer will offer training and usually an 800 number help line in case problems arise. Within the software package, the clinician and staff will have the ability to process the image by changing contrast, brightness, sharpness, and other parameters. For some software, a single "button" will automatically optimize the image. For other software, the processing is in the hands on the dental professional using the software to optimize the image for best diagnosis.
Even though the images captured by the sensor will be of a diagnostic quality equal to or better than conventional film17,18 the processing (changing) of the image can enhance diagnosis. Some typical examples of image processing include changes in contrast and image density, use of a magnification tool when viewing the image, subtraction radiography, image reversal, embossing, and other features. The software will also allow the operator to rotate, flip, and swap images.
Many systems have templates so that a full-mouth series can be projected or bitewings can be projected (Figure 3 and Figure 4). Some software programs allow the operator to create custom templates, such as for endodontic treatment cases, for example. The operator will be able to display several images on the screen side-by-side and compare them. One has to be careful not to over-enlarge an image or to over-process an image by changing the grayscale or over-sharpening an image. This can create "noise" and distortions that can create artifacts that give a false positive for caries, boney pathology, or periodontal disease, and hinder diagnosis. One feature of digital x-ray software is magnification or zoom, which allows the operator to view areas enlarged to project details of subtle changes that may otherwise go undetected.
The contrast and density modifications allow the operator to correct for over- and under-exposures without distorting the image, which with conventional film will lead to the need for a remake of the image. Other features include reversal of the grayscale where all black areas are converted to white and white areas are converted to black. This reversal can aid in better viewing of certain areas or objects by darkening or lightening them. The operator can colorize an image and compare images taken previously to evaluate changes in bone remodeling and bone healing.19,20 Some systems allow for combining images and looking at changes in bone height, which is especially useful for implants. In some cases specialized software for caries diagnosis may be available.
Each gray shade is assigned a specific color. This can enhance interpretation and diagnosis as the human eye is more sensitive to colors than shades of gray. Digital subtraction is also a feature of the software. This will allow the operator to merge two images taken at different visits in the same area. The images are then subtracted from each other, leaving behind only the changes between them. By doing this the operator can determine whether or not a change has occurred in a specific area over time. This is very useful when monitoring an implant, periodontal disease progression, or the advancement of decay in a specific location. For digital subtraction to work successfully, the two images must be standard. Any changes in sensor placement or beam angulation will display changes that may not be true physical changes.
Additional features in software can include having the ability to place notes over a particular location on an image. A valuable tool in software programs is the measurement tool. This digital ruler allows the operator to measure bone loss in a patient diagnosed with periodontal disease or measure the length of a root canal during endodontic treatment. In all cases, the software can save processed images as additional images without changing the archived original images. At any time, the specific information for any image to include patient name, date the image was made, and whether or not the image was processed will be accessible for each image.
Making Digital Radiographs
If the decision is made to use PSP sensors, the transition from conventional film will be almost seamless. As noted earlier, CCD and CMOS sensors are thicker and larger than conventional film, so the sensor will require a special holder. Be certain to order enough sensor holders to accommodate sterilization and image-collecting cycles. Also, use the barriers for infection control when capturing images using sensors. When making several images or a full-mouth series, you will appreciate that the same sensor is used over and over again. For each sextant of the mouth, by experience and office protocol you will know when a number one or number two sensor should be used. One additional benefit is that you will know right away if you captured the view you desired. If the image is in any way unacceptable for diagnostic purposes, it is easy to just retake the image.
The act of exposing a sensor parallels conventional film. The sensor is placed in the patient's mouth and when the exposure is completed, the sensor stores the latent digital image just as a conventional film would. For a CCD/CMOS sensor, the latent image is transmitted and converted into a visible image by the computer. The image is displayed on the monitor in pixels as various shades of gray, black, and white. For PSP, the sensor must be discharged and processed in the laser processor.
Using digital radiography offers the patient benefit of reduced radiation. Because the sensors are more sensitive to the x-ray photons than conventional film, approximately 50% to 80% less radiation will be used when exposing the sensor compared to F-grade film. The existing x-ray unit can be the same radiation source for digital radiography as was used for conventional film. Depending on the x-ray unit, there may be a need to have the unit adapted for less radiation during exposures. The manufacturer will provide guidance to on what conversion changes need to be made.
Patient Preparation and Procedure
Using the digital sensor will be new to most patients. Explain the procedure to the patient. Before making an exposure, enter the patient information and date of exposure (for some software this is automatic) into the computer and select the type of radiographic examination that will be completed on the patient.
With the patient seated, the same positioning rules and techniques that are used for conventional film will be used. Similar sensor holders will be used when positioning the sensor in the patient's mouth. As with any radiographic examination, inspect the oral cavity for any intraoral conditions that may interfere with image capture. This can include bony tori, partial dentures, tongue or lip piercing, orthodontic appliances, and extraoral objects such as jewelry. Removable objects should be removed. Adjust the dental chair to the appropriate height for the operator and adjust the patient's head so that the maxilla is parallel to the floor and the mid-sagittal plane of the patient is perpendicular to the floor. Place a lead apron with a thyroid collar on the patient. Once the x-ray unit is turned on, the settings should be set according to the guidelines provided with the sensor system being used. It is a good idea to have a chart listing the recommended settings. In most cases you will find that your exposure with a digital sensor is at least half of that used for exposing F-speed conventional intraoral film.
The sensor should be covered with a disposable plastic barrier and placed in the appropriate holder so that the images can be exposed using the paralleling technique. Placement for sensors is similar to placement for conventional films with the exception that the sensor is more rigid than film and can be more uncomfortable for the patient. In this author's experiences, when placing a sensor, there are times you want to use special cushioning tabs on the periphery of the sensor so that the patient is more comfortable. With the sensor positioned, position the x-ray cone using the holder as a guide. Activate the sensor using the computer, leave the room, and complete the exposure by activating the x-ray head.
With the image captured, evaluate the image. If the image is not acceptable, perform the necessary equipment adjustment (eg, adjust the PID or adjust the sensor placement) to retake the image, and complete the exposure. If a PSP system is being used, after the exposure has been completed, remove the sensor from the patient's mouth, discard the barrier, and place the sensor in the scanner. View the image on the screen. If a retake is necessary, erase the phosphor plate by exposing it to light (with some scanners they are automatically discharged) and then retake the image.
As stated earlier, the images will be saved and a back-up of the images should also be created. Depending on the computer system or network, the back-up can be on a hard drive on the same computer or on a computer server at a remote location elsewhere in the dental office. This use of a back-up system allows the digital images to be protected against computer failures. All images must be stored via alternate methods, and this procedure should be completed on a daily basis. The images can be stored on tape, a mirrored hard drive, compact discs, and digital video discs.
Future of Digital Radiography
Digital radiography systems have improved significantly.15 In the past, these systems had many disadvantages, such as poor image quality and high cost. Over the past several years, image quality has improved tremendously with significant improvements to the software to provide for enhanced diagnosis and easier use of the software, and the systems themselves have become much more affordable. As a result, many offices are opting to convert to digital systems and many new practitioners are opting to install digital radiography systems in their offices.
For the allied dental professional, the use of digital radiology in your dental office will first appear to be burden. Within a short period of time it will prove itself to be the valuable tool it is. Digital radiography technology will save your office time, provide for reduced exposure for patients and dental staff, allow for immediate image correction, offer the ability to process images for better diagnosis, and provide a better method of organizing records that can be easily retrieved with accurate patient and date information.
Reference
1. Benington PC, Khambay BS, Ayoub AF. An overview of three-dimensional imaging in dentistry. Dent Update. 2010;37(8):494-500.
2. Petrikowski CG. Introducing digital radiography in the dental office: an overview. J Can Dent Assoc. 2005;71(9):651.
3. Hoos JC. Practice efficiency using digital radiography. Pract Proced Aesthet Dent. 2006;18(1):46.
4. Senel B, Kamburoglu K, Uçok O, et al. Diagnostic accuracy of different imaging modalities in detection of proximal caries. Dentomaxillofac Radiol. 2010;39(8):501-511.
5. Furkart AJ, Dove SB, McDavid WK, et al. Direct digital radiography for the detection of periodontal lesions. Oral Surg Oral Med Oral Pathol. 1992;74(5):52-60.
6. de Morais JA, Sakakura CE, Loffredo LC, Scaf G. Accuracy of zoomed digital image in the detection of bone defect : in vitro study. Dentomaxillofac Radiol. 2006;35(3):139-142.
7. Akdeniz BG, Soğur E. An ex vivo comparison of conventional and digital radiography for perceived image quality of root fillings. Int Endod J. 2005;38(6):397-401.
8. Levin MD. Advanced technologies in endodontic practice: computer infrastructure and digital radiography. Alpha Omegan. 2004;97(4):51-61.
9. Swennen GR, Schutyser F. Three-dimensional cephalometry: spiral multi-slice vs cone-beam computer tomography. Am J Orthod Dentofacial Orthop. 2006;130(3):410-416.
10. Cevidanes LH, Styner MA, Proffit WR. Image analysis and superimposition of 3-dimensional cone-beam computed tomography models. Am J Orthod Dentofacial Orthop. 2006;129(5):611-618.
11. Goga R, Chandler NP, Love RM. Clarity and diagnostic quality of digitized conventional intraoral radiographs. Dentomaxillofac Radiol. 2004;33(2):103-107.
12. Benjamin S. Phosphor plate radiography: an integral component of the filmless practice. Dent Today. 2010;29(11):89.
13. Ang DB, Angelopoulos C, Katz JO. How does signal fade on photo-stimulable storage phosphor imaging plates when scanned with a delay and what is the effect on image quality. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(5):673-679.
14. Akdeniz BG, Gröndahl HG. Degradation of storage phosphor images due to scanning delay. Dentomaxillofac Radiol. 2006;35(2):74-77.
15. van der Stelt PF. Filmless imaging, the uses of digital radiography in dental practice. J Am Dent Assoc. 2005;136(10):1379-1387.
16. Kitagawa H, Farman AG, Scheetz JP, et al. Comparison of three intra-oral storage phosphor systems using subjective image quality. Dentomaxillofac Radiol. 2000;29(5):272-276.
17. Vandre RH, Pajak JC, Abdel-Nabi H, et al. Comparison of observer performance in determining the position of endodontic files with physical measures in the evaluation of dental x-ray imaging systems. Dentomaxillofac Radiol. 2000;29(4):216-222.
18. Syriopoulos K, Sanderink GC, Velders XL, van der Stelt PF. Radiographic detection of approximal caries: a comparison of dental films and digital. Dentomaxillofac Radiol. 2000;29(5):312-318.
19. Edwards SP. Computer-assisted craniomaxillofacial surgery. Oral Maxillofac Surg Clin North Am. 2010;22(1):117-134.
20. Angelopoulos C, Aghaloo T. Imaging technology in implant diagnosis. Dent Clin North Am. 2011;55(1):141-158.
About the Authors
Howard E. Strassler, DMD
Professor, Division of Operative Dentistry
Department of Endodontics, Prosthodontics, and Operative Dentistry
University of Maryland Dental School
Baltimore, Maryland
Vaishali Singhal, DMD, MS
Associate Professor
School of Health Related Professions
University of Medicine and Dentistry of New Jersey
Newark, New Jersey