You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Dental caries among preschool-aged children in the United States (US) remains a public health concern. Despite early promotion efforts such as establishing a dental home, recommending the first dental visit by age one, and the integration of collaborative approaches with medical professionals,1 dental caries among young children continues to occur.2 In 2015-2016, 21.4% children aged 2-5 years were reported to have active dental caries while 8.8% had untreated dental caries.2 Untreated dental caries can negatively impact growth and development, learning, and overall health.3 Caregivers' oral health knowledge and overall awareness of the child's dentition may play a critical role in preventing a potential dental emergency. Divaris et al.4 found that a caregiver's reported oral health status for their young child generally correlated to the treatment needed. For example, children of caregivers who reported their child's oral health status as fair or poor were more likely to present with extensive treatment needs. Additionally, a small proportion of the caregivers with children under 2 years who indicated the child had good health status had actually underestimated the child's treatment needs.4 Similarly, Talekar et al. found that caregivers perceived a poor oral health status if they felt that the child needed treatment or preventive dental care, and if the child's general health was less than excellent.5 Conversely, if the child was caries free, caregivers perceived that as having better oral health.5
Caregivers' understanding of oral health has a significant impact on oral health behaviors and the adoption of professional recommendations for themselves as well as their child. Caregivers must be able to understand and apply health and oral health information so that the child receives appropriate and timely preventive services. This process, known as oral health literacy (OHL), has been defined as "…the degree to which individuals have the capacity to obtain, process and understand basic oral craniofacial health information and services needed to make appropriate health decisions."6 Baskaradoss et al. found that caregivers' poor OHL was related to untreated dental caries among children as well as a greater lifetime of dental caries and treatment needs than caregivers who were identified as having adequate OHL.7 Miller et al. also identified an association with caregivers' OHL and the child's oral health status.8 When examining the financial impact to the health care system, Vann et al. found that young children of caregivers with low OHL had higher expenditures for emergency dental care than caregivers with higher levels of OHL.9
The Rapid Estimate of Adult Literacy in Dentistry-30 (REALD-30) is a word recognition test10 that has been used to measure OHL among adults with young children4,9-10 Within the last decade, Richman et al. developed a 36-item Oral Health Literacy Inventory for Parents (OH-LIP), which focuses on pediatric oral health literacy by assessing word recognition, vocabulary, and comprehension of caregivers.11 Richman et al. administered the OH-LIP inventory among 45 caregivers of children who attended a Head Start program and found that 48% of caregivers demonstrated a misunderstanding of the term "decay."11 In fact, the comprehension of decay had the most incorrect responses of all terms in the inventory. Although "decay" is not a technical term, it is used in the vernacular frequently, and as such is a critical oral health related word. Understanding and comprehending the decay process is important for healthy, at-home oral hygiene and diet choices for both caregiver and child. While the OH-LIP allows for the evaluation of correct and incorrect responses of term recognition and vocabulary, examining the comprehension of terms is of equal importance.
Tooth decay and cavities are the most common oral health consequences for young children that may result from inadequate OHL or understanding of their caregivers. The purpose of this study was to answer the question "What are caregivers' comprehension and understanding of the terms ‘decay' and ‘cavities' related to children's oral health?" through the qualitative analysis of caregivers' responses on the OH-LIP inventory.
Methods
A qualitative analysis was performed on responses from the Oral Health Literacy Inventory for Parents (OH-LIP) made by consenting, English-speaking caregivers with children aged <6 years. Participants were recruited from two private dental practices in Washington State from February to August 2012. The OH-LIP instrument is a multi-part oral health literacy inventory that has been examined previously for face and content validity.11 The inventory contains 36 terms related to pediatric oral health and consists of three components: word recognition (part I), vocabulary knowledge (part II), and comprehension (part III).11 The OH-LIP was conducted by one of two interviewers both of whom were trained to administer the instrument. Interviews were recorded and transcribed, and the transcriptions were coded by one investigator to eliminate inter-examiner variability.
To evaluate word recognition, caregivers were asked to read the terms aloud. Vocabulary knowledge was assessed by the examiner reading the terms aloud and the caregiver providing a definition. Comprehension by caregivers was measured by brief passages from oral health literature.11 This was not designed as an exhaustive measure of comprehension; however, it provides a way to measure whether the caregiver understands the basic term far more than reading recognition alone. For example, another OH-LIP term "erupt" led many caregivers to suggest it meant an abscess, pus, or an infection versus a tooth coming into the mouth, even though they were able to read the term correctly. Caregivers were not asked to select from multiple options defining the term but were asked to define a term using their own words.
Participants' responses to the OH-LIP inventory were audio recorded, transcribed, and verified for accuracy.12 The focus of this investigation was to qualitatively analyze caregivers' comprehension (part three of the OH-LIP) regarding the terms "decay" and "cavities." The data used for this study was from a larger set of data collected by one of the investigators of the current study. The institutional research compliance office of Old Dominion University deemed the study as "not human subjects research" since the data was collected and provided to the authors without identifiers.
Data Analysis
Demographic data was analyzed using descriptive statistics including counts and percentages. A general inductive approach was used to qualitatively analyze responses from the OH-LIP-III for the terms "decay" and "cavities." The general inductive approach establishes meaning of the raw text to the research question or objectives, creates themes or categories from the raw text, and summarizes themes or categories, which may develop into a model or theory.13 The following approach was used: 1) Each term was coded based on the level of content related to "decay" and "cavities" to create the main themes; 2) Domains were created based on common responses and patterns observed for each of the themes; 3) Responses were categorized based on the participants' own words and corresponding term definitions. One investigator completed the initial review of responses associated with each term and created domains and categories. Next, two other investigators independently assessed and assigned responses to the predetermined categories by the first investigator. After this process was completed for both terms, the investigators reviewed responses and assignments together to assess the level of agreement with categories. For the term "decay," the investigators were inconsistent 33 times out of the 111 responses, and for "cavities" 26 times out of the 111 responses. For responses that were inconsistently assigned by the investigators, it was discussed until a mutual agreement was met for the category assignment.
Results
Demographic data and word inventory responses were provided for the caregiver participants (n=114); three participants did not provide responses to the word items "decay" and "cavities" and were excluded from the analysis. Descriptive statistics showed the majority of the participants were female (85%), between 18 and 35 years of age (97%), identifying as Caucasian or White (76%), Non-Hispanic (88%), with English as the primary spoken language at home (86%). More than half (67%) of the respondents reported a household income of less than $40,000 and 90% of caregivers reported obtaining at least a high school degree or GED or higher. (Table I).
All participants (n=111) responded correctly when asked to say the words "decay" and "cavities" aloud from the full list of thirty-six words used in the inventory. Participants were then asked to define each word in the inventory to the best of their ability. Each word definition was given a score of "not correct," "partially correct," or "fully correct," Fewer than 10% of the participants provided a fully correct response to the words, "decay" (6.3%) and "cavities" (5.4%). The majority had a partially correct response for "decay" (74.7%) and "cavities" (71.2%). Each participants' response (definition of the term) was categorized and placed under one of the established domains based on the collective themes found in the responses for the terms "decay" (Table II) and "cavities" (Table III).
The investigators then analyzed the participants' responses to the terms "decay" and "cavities," to examine their understanding and comprehension. Domains were developed based on common themes from the responses for each term.
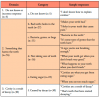
Participant responses to the "decay" term
Domain 1. Do not know
Nearly one-fifth of the participants (19.8%, n=22) indicated that they did not know what decay was or provided a definition that was incorrect or unrelated. Some stated they did not know the definition of decay while others concluded that decay was some type of flaw in the tooth structure. For example, "Decay is the wearing of the tooth."
Domain 2. Teeth going bad
A majority of the participants (71.2%, n=79) made the association that decay was something bad that happens to the teeth. Most of the respondents described decay as a tooth dying, falling apart, or rotting. A few of the respondents perceived the term "decay" as something that happens to the teeth when there was no oral hygiene care. In fact, one respondent stated, "What happens to our teeth if you don't take care of them."
Domain 3. A disease on the tooth
Fewer than one-fifth of the participants (9%, n=10) identified decay as being caused by bacteria, germs, or infection. These respondents correctly identified decay as destruction of the tooth surface because of bacterial action. One respondent indicated that decay was a "Tooth that has an infection" (Table II).
Participant responses to the cavity term
Domain 1. Do not know or incorrect response
Only a few of the participants (4.5%, n=5) indicated that they did not know or could not explain the term "cavities." These respondents simply stated, "I don't know," or provided an incorrect response when asked to define the term.
Domain 2. Something that harms the teeth
Two-thirds of the participants (68.5%, n=76) indicated that cavities were something that is harmful to teeth. Nearly, one-half of the respondents in this domain associated the term "cavities" with "bad teeth or holes,"or "bacteria, germs, or bugs." One respondent reported, "Holes in your teeth that cause pain."The other respondents in this group associated cavities with poor oral hygiene, "A sign you're not brushing enough," or eating a high sugar diet, "Cavities are what you get from eating sugar."
Domain 3. A cavity is the result of decay
Over one-quarter of the participants (27%, n=30) made the association between decay and cavities. All respondents in this domain identified cavities as a result of the decay process. One respondent stated, "That's teeth that have started decaying" (Table III).
Discussion
Dental hygienists provide care in a variety of clinical settings including community health and public health centers, schools,14 and medical settings.15 As oral health care professionals, they play a critical role in educating caregivers as well as non-dental professionals on the impact of the caregivers' OHL as it relates the child's oral health status. Findings from this study revealed that only 5-6% of the respondents were able to provide a fully correct response to the definition of the terms "decay" and "cavities." In addition, fewer than 10% of the respondents were able to clearly make the connection that tooth decay is caused by bacteria or infection, and only about 25% of the caregivers were able to make the association between decay and cavities. In an earlier study by Richman et al., decay was found to be the most misunderstood term in the comprehension portion of the OH-LIP inventory among caregivers attending two Head Start programs.11 This finding was the motivation for the current study to determine whether similar results would be evident among caregivers attending a private dental office. Based on the findings of this study, comprehension of decay and cavities is still misunderstood by caregivers of children under the age of six years. Findings from the current study also demonstrate that the understanding and comprehension of the terms "decay" and "cavities" is inadequate, regardless of population settings (i.e. Head Start or private dental office), which further highlights concerns related to dental cavities and untreated decay among children observed at the national level.2
Caregivers' OHL and understanding of the dental caries process impacts the oral health outcomes of the children in their care. Furthermore, mothers' and/or caregivers' oral hygiene habits and behaviors are translated to the child, underscoring the importance of starting conversations about healthy oral hygiene behaviors during the prenatal period. In fact, these early conversations have been recommended by national guidelines and polices as a means to increase positive oral health outcomes for the child.16-17
In this study, caregivers were able to recognize the causes, symptoms, and oral hygiene behaviors to reduce the risk of decay and cavities; however, there was inadequate comprehension of the bacterial process. Similarly, in a focus group conducted by Lotto et al., participants were able to associate dental caries with negative short and long-term consequences for the child, such as problems with permanent teeth, discrimination, and psychological damages.18 In addition, parents also agreed with the importance of proper oral hygiene and dietary behaviors but reported deviating from these practices based on the behaviors of the child.18 For example, in terms of toothbrushing, one participant reported asking the child about toothbrushing but did not actually follow up to ensure the toothbrushing was performed, due to other responsibilities.18 This suggests that while parents may be aware of the practices needed to prevent dental caries, due to other extenuating factors, they may be unable to implement those practices. Horowitz et al. identified a similar finding concerning assistance and careful monitoring of toothbrushing among children in a focus group conducted among caregivers in the state of Maryland.19 Focus group participants reported not forcing the child to brush their teeth if it was not desired by the child, thus not recognizing the importance of proper oral hygiene care in preventing dental caries.19 Similar to findings in the present study, participants in the Horowitz et al. study were aware of the behavioral causes of dental caries but did not make the connection to the potential severity of the disease. In addition, none of the participants in the focus groups were able to connect the bacteria aspect of the disease process, particularly the vertical transmission from mother to child.19 Vertical transmission of dental caries is a common mode of spreading disease from mother to child or family members to child; thus, it is imperative for caregivers to comprehend the negative impacts of bacterial transmission.
Utilizing the explanatory model interview catalogue (EMIC) in a Hispanic population, Rivera et al. also found that caregivers were aware of the causes of dental caries such as the consumption of sugary foods and inadequate toothbrushing and were able to communicate the symptoms of dental caries such as tooth color change and pain.20 Caregivers also believed the risk of dental caries could be lowered by daily toothbrushing,20 which was a similar finding in the current study.
Findings in this study demonstrated an incomplete and inaccurate understanding of the process of tooth decay and cavities. Simply indicating that decay is a rotting tooth does not imply comprehension of what is causing the outcome, such as frequent exposures to cariogenic foods and drinks. Dental and non-dental health care providers should be cognizant of utilizing the following practices to improve caregivers' understanding: use of simple language and open communication to confirm instructions; encourage questions to ensure the caregiver's understanding; and provide oral health literature that increases understanding of common dental terms.11
Limitations
This study had limitations. The data was collected in 2012 from two private dental practices in one state. While the data used to conduct the qualitative analysis was dated, to the best of the investigators' knowledge, only two studies11,12 have been conducted utilizing the OH-LIP instrument. The OH-LIP instrument is unique in that it captures knowledge and comprehension of parents with young children, which differs from other OHL tests such as the REALD-30. Findings from this study also highlight the need for focusing efforts on increasing caregivers' understanding and comprehension of dental terms. Another limitation may be due to the nature of the OH-LIP inventory and the potential of social desirability bias among the participants. The caregivers may have responded to the knowledge and comprehension portions of the OH-LIP inventory interview based on what they believed was socially acceptable. However, given these limitations, this study builds on previous research in examining caregivers' comprehension of tooth decay and cavities, and the results suggest that more discussion related to the dental caries process is needed to increase comprehension in this population.
Conclusion
There are disparities in caregivers' understanding and comprehension of the common oral health terms "decay" and "cavities." While caregivers may be able to recognize causes and how to reduce the risk of decay and cavities, understanding of the process is inadequate. All health care providers, including dental hygienists and dentists, who provide care to mothers, caregivers, and children play an essential role to ensure that the messaging of the dental caries process is understood. Assessing understanding can be easily integrated by asking caregivers open-ended questions regarding the content discussed during the visit. Limiting the amount of content presented at each care appointment may also be helpful to ensure better comprehension. Future studies may consider focusing on the role of these oral health literacy interventions on pediatric oral health outcomes over time.
Denise M. Claiborne, PhD, MS, RDH is an assistant professor and the Graduate Program Director, Gene W. Hirschfeld School of Dental Hygiene; Deanne Shuman, PhD, MS, RDH is a professor emerita, Gene W. Hirschfeld School of Dental Hygiene; Melissa Sullivan, MS, RDH is a doctoral student in the Health Services Research Program; all in the College of Health Sciences, Old Dominion University, Norfolk, VA, USA.
Julia Richman, DDS, MSD is in private practice in Covington, WA and is an affiliate assistant professor in the School of Dentistry, University of Washington, Seattle, WA, USA.
References
1. American Academy of Pediatric Dentistry. Periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents [Internet]. Chicago (IL): American Academy of Pediatric Dentistry; 2018 [cited 2020 October 9]. Available from: https://www.aapd.org/globalassets/media/policies_guidelines/bp_periodicity.pdf
2. Fleming E, Afful J. Prevalence of total and untreated dental caries among youth: United States, 2015-2016 [Internet]. Rockville (MD): National Center for Health Statistics; 2018 [cited 2020 Nov 18]. Available from: https://www.cdc.gov/nchs/data/databriefs/db307.pdf
3. Collado V, Pichot H, Delfosse C, et al. Impact of early childhood caries and its treatment under general anesthesia on orofacial function and quality of life: a prospective comparative study. Med Oral Patol Oral Cir Bucal. 2017 May; 22(3): e333-e341.
4. Divaris K, Vann WF, Baker AD, et al. Examining the accuracy of caregivers' assessments of young children's oral health status. J Am Dent Assoc. 2012 Nov; 143(11):1237-47.
5. Talekar BS, Rozier RG, Slade GD, et al. Parental perceptions of their preschool-aged children's oral health. J Am Dent Assoc. 2005 Mar;136(3):364-72.
6. NIDCR. Healthy People 2010 oral health toolkit [Internet]. Rockville (MD): Department of Health and Human Services: n.d. [cited 2020 Nov 18]. Available from: https://stacks.cdc.gov/view/cdc/11474/cdc_11474_DS1.pdf
7. Baskaradoss JK. Relationship between oral health literacy and oral health status. BMC Oral Health. 2018 Oct;18(182):1-6.
8. Miller E, Lee JY, DeWalt DA, et al. Impact of caregiver literacy on children's oral health outcomes. Pediatrics. 2010 Jul;126(1):107-14.
9. Vann WF, Divaris K, Gizlice Z, et al. Caregivers' health literacy and their young children's oral-health-related expenditures. J Dent Res. 2013 Jul;92(1 Suppl):55s-62s.
10. Lee JY, Rozier RG, Lee S-YD, et al. Development of a word recognition instrument to test health literacy in dentistry: The REALD-30- a brief communication. J Public Health Dent. 2007 Spr; 67(2):94-8.
11. Richman JA, Huebner CE, Leggott PJ, et al. Beyond word recognition: understanding pediatric oral health literacy. Pediatr Dent. 2011 Sep/Oct;33(5):420-5.
12. Chi DL, Richman J, Senturia K, et al. Caregivers' understanding of fluoride varnish: Implications for future clinical strategies and research on preventive care decision making. J Public Health Dent. 2018 Sep;78(4):282-6.
13. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006 Jun;27(2):237-46.
14. ADHA. Facts about the dental hygiene workforce in the United States [Internet]. Chicago (IL): American Dental Hygienists' Association; 2020 [cited 2020 Nov 4]. Available from: https://www.adha.org/resources-docs/75118_Facts_About_the_Dental_Hygiene_Workforce.pdf
15. ADHA. Dental hygiene in medical settings and health clinics [Internet]. Chicago (IL): American Dental Hygienists' Association; 2020 [cited 2020 Nov 4]. Available from: https://www.adha.org/resources-docs/Dental_Hygiene_in_Medical_Settings.pdf
16. Oral healthcare during pregnancy: A national consensus statement [Internet]. Washington, DC: National Maternal and Child Oral Health Resource Center; 2012 [cited 2020 Nov 18]. Available from: https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf
17. Holt K, Clark M, Barzel R. Two healthy smiles: tips to keep you and your baby healthy (rev.) [Internet]. Washington, DC: National Maternal and Child Oral Health Resource Center; 2009 [cited 2020 Nov 18]. Available from: https://www.mchoralhealth.org/PDFs/pregnancybrochurefullpage.pdf
18. Lotto M, Strieder AP, Aguirre PEA, et al. Parental perspectives on early childhood caries: a qualitative study. Int J Paediatr Dent. 2020 Jul;30(4):451-8.
19. Horowitz AM, Kleinman DV, Child W, et al. Perspectives of Maryland adults regarding caries prevention. Am J Public Health. 2015 May;105(5): e58-e64.
20. Rivera Y, Boyd LD, Libby L. Hispanic seasonal farmworker caregivers' beliefs and perceptions of early childhood caries. J Dent Hyg. 2020 Oct;94(5):14-21.
v