You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Face-touching has been identified as an important transmission route to self-inoculate viruses and other transmissible microorganisms.1 This is a particularly important factor to consider during the COVID-19 pandemic. Guidelines provided by the Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) to avoid COVID-19 include limiting close contact with others; wearing a mask; washing hands frequently; and avoiding touching one's eyes, nose, and mouth.2,3 The eyes, nose, and mouth are areas of the face identified as target mucosal membranes,4 or the T-zone for infection transmission. Hands may touch many surfaces, some of which may be contaminated with pathogens.
Touching one's eyes, nose, or mouth can potentially transmit (or self-inoculate) pathogens through oro-naso-ocular mucus membranes. For example, bacterial self-inoculation of Staphylococcus aureusis possible through
face-touching behavior. S. aureushas been identified in the nasal mucosa of nearly one-fourth of both community and healthcare settings.5,6 Similarly, viral self-inoculation is possible through face-touching behavior. Self-inoculation of herpes simplex virus type-1 (HSV-1) may occur if cold sores are touched. Viral transmission to fingers (herpetic whitlow) and eyes (herpes zoster opthalmicus) are possible. The extent to which face-touching behavior is responsible for pathogen transmission in any particular disease is difficult to determine.5 Nevertheless, there are anecdotal reports demonstrating that decreasing face-touching behavior, particularly of the T-Zone, has resulted in fewer upper respiratory tract infections.4,7
When diseases are highly transmissible with high levels of morbidity and mortality, and limited therapeutics, every consideration for safety should be in place. This is especially true for healthcare workers who may inadvertently transmit disease to themselves or others through unconscious face/mask/respirator touching behaviors. Some face/mask/respirator touching behavior has been attributed to an urge to relieve the irritation of the presence of mild abrasions on the face, especially those resulting from the mask/respirator.8 Data collected prior to the COVID-19 pandemic has shown that personal protective equipment (PPE) protocol breaches are common. In a study of acute care hospital workers in the United States, 26% of the participants touched the front of their mask while doffing and nearly half of them touched the mask's surface with ungloved hands.9 In a behavioral observation study in the United Kingdom, medical students were observed for face-touching behavior and participants were shown to have had a mean of four mouth touches and three nose touches per hour.5
Face-touching behavior also has cultural differences and gender differences may also be possible. In a study comparing face-touching behavior between British and Japanese participants, the British participants were more likely to touch the left side of the face with the left hand as compared to the Japanese participants.10 Another study indicated that men were more likely to engage in non-verbal self-touching behavior than women; however, women were reported to be more likely to self-touch during anxiety-inducing situations.11
Overall, there is limited research examining self-inoculation from face-touching behavior. However, given the nature of the COVID-19 pandemic and the recommendations from the CDC and WHO regarding face-touching and self-inoculation behaviors, it is critical address these behaviors in dental and dental hygiene students so that targeted awareness campaigns and professional education can reduce exposure risks. The purpose of this study was to observe unconscious face-touching behaviors of dental hygiene and dental students in a non-clinical setting and examine whether differences exist between dental and dental hygiene students or between genders.
Methods
This cross-sectional study was approved by the West Virginia University Institutional Review Board (protocol 2003954300). The data used in this study were extracted from archived proctoring videos for dental and dental hygiene courses. These courses had online final examinations following the COVID-19 pandemic shutdown of 2020. The sample consisted of dental students (n=45) and dental hygiene students (n=42); all participants were 18 years or older. Prior to taking the spring semester final examinations, all students (n=87) had access to the School of Dentistry's COVID-19 Task Force's clinical training documents and resources. These resources, based upon guidance from CDC, American Dental Association, Occupational Safety and Health Administration, and the Organization for Safety Asepsis and Prevention, recommended strict infection control policies, which included avoiding touching the T-zone of the face. All dental and dental hygiene students, as well as all faculty members, were required to complete the infection control educational training modules specifically addressing COVID-19 and pass the post-test.
Two researchers (RCW and AKTS) viewed 20 minutes of archived proctoring videos of dental and dental hygiene students taking their online final examinations. In watching the archived proctoring videos, incidents of touching face, eyes, glasses, nose, mouth, hair, and ears were recorded for each student. A statistical program (SPSS version 26, IBM; Armonk, NY) was used for the data analysis. Descriptive statistics are presented as frequencies, percentages, mean, and standard deviation. Differences between the face-touching behavior of dental and dental hygiene students as well as the differences between genders were analyzed using independent samples t-test. Statistical significance was assessed at p<.05. Due to limited cell sizes and potential for participant identification, all cell sizes were suppressed when cell was <10.
Results
A total of three videos of dental and dental hygiene students were viewed (n=87). The sample consisted of 24 males (27.9%) and 62 females (72.1%). Approximately half of the students were dental hygiene students (n=42, 48.8%) and the rest were dental students (n=45, 51.2%). The vast majority of the participants (95.5%, n=83) touched the mucosal membrane T-zone (mouth, nose, and eyes) at least once during the twenty minutes of viewing. The mean number of T-zone touches was 10.3 (SD, 9.8; minimum 0, maximum 41). Although not the focus of this study, the mean number of any face touching (mouth, nose, eyes, hair, ear, and/or glasses) was 15.5 (SD, 11.1; minimum 2, maximum 51).
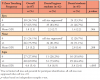
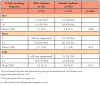
Dental hygiene students were more likely to touch their lips, nose, ears, T-zone, bite their nails, or touch any T-zone, hair, ears, and/or glasses than dental students. Face-touching behavior details of the participants are presented in Table I. In analyzing face-touching behaviors by gender, males were more likely to touch their noses (p= 0.012) and females were more likely to touch their lips (p=0.011). The difference in touching the T-zone or touching any T-zone, hair, ears, and/or glasses failed to reach significance between the sexes. Face-touching behaviors by gender are shown in Table II.
Discussion
Findings from this study showed that over 95% of dental and dental hygiene students unconsciously touched their mucosal membrane T-zone (mouth, nose, and/or eyes) during the first twenty minutes of taking a final examination during the COVID-19 pandemic shutdown in the spring of 2020. Both male and female students demonstrated this behavior, although the area of the face touched varied by gender.
In a recent systematic review on the frequency of T-zone touching, amidst the COVID-19 pandemic, no significant difference in face-touching behavior between sexes was identified in nine out of the ten reviewed studies.1 The review included studies from different settings and regions of the world and it was concluded that the participants touched their eyes, nose, mouth, and chin approximately 69 times per hour.1 Extrapolating the results from this study from twenty minutes to an hour, there would be an estimated occurrence of 46.5 touches to the T-zone, hair, ears, and/or glasses, indicating rates lower than those of the systematic review.
While there is limited research reporting on the face-touching behaviors of medical/health professionals or students, 5,12 clinicians and staff in medical offices in a study were found to have touched their T-zone an average of 19 times over a two-hour period12 These rates were lower than those observed in the current study. However, face-touching behaviors of health care providers in medical practices might differ based on the setting. In this study, oral health care students were engaged in a stressful activity outside of the clinic setting and unconscious face-touching behavior might have differed due to the environment.
Little has been reported in the literature regarding self-inoculation of respiratory viruses through contaminated hands coming in direct contact with mucous membranes.1 However, some studies have shown that reducing the frequency of touching eyes, ears, and mouth also reduces the likelihood of respiratory tract infections.7,12 The question remains as to why future health care providers would continue to exhibit unconscious face-touching behaviors that promote the potential to transfer pathogens to themselves and to others. Researchers believe one of the difficulties for infection control or prevention lies in the fact that pathogens are invisible to the naked eye.13 The invisible nature of pathogens makes it more difficult to improve hand hygiene in settings where hands may not be visibly soiled, yet still need disinfection, even in the home environment.13
The mismatch between expressed intentions and the actual behavior of the participants in this study is similar to the now widely accepted belief that certain processes that determine behavior are unconscious.13 Unconsciousness or unconscious influence has recently been defined as "a lack of awareness regarding the influences or effects of a triggering stimulus."14 However, the apparent unconscious behavior exhibited by the participants, such as face-touching behavior or removing their glasses, could be an inherent characteristic of human cognitive decision making, based on the causality between the glasses and eye pain, or skin sensitivity to pressure and pain.15
Therefore, not all behaviors are necessarily unconscious. Sax et al., observed nurse hand hygiene within an intensive care unit following participation in simulation-based hand hygiene training a few days earlier and found that when assessing the verbalized attitudes and beliefs against the theory of planned behavior, the nurses would certainly have scored high on intention to act.16 Moreover, the participants would also respond positively if questioned about social norms in regard to expressed positive beliefs about the outcome of the activity, yet they failed to perform proper hand hygiene and infection prevention strategies.16 The behavior in question was not obstructed by any of the frequently cited barriers to hand hygiene since time pressure did not appear to be an issue, and hand-rub dispensers were abundant and conveniently located.13,17 Similar outcomes would be assumed of the students in this study in regard to self-inoculation risks from face-touching behavior. Both groups of students have undergone training and would have scored high on intention to act, based on their verbalized attitudes and positive beliefs regarding the outcomes of infection prevention. However, the face-touching behaviors of the participants were observed frequently, which could present significant risk factors for pathogen transfer and infection.
One reason face-touching may be a difficult habit to correct is due to the soothing effect of touching the face where the trigeminal and facial nerves are close to the surface (for example, the supraorbital nerve of the trigeminal at the supraorbital foramen, and the suborbital nerve of the trigeminal at the suborbital foramen). These points have been used in alternative and complementary medicine (acupressure, acupuncture, tapping) for relief of pain and stress. Perhaps increasing awareness of the underlying aspects of these habits will be beneficial in avoidance of face-touching behavior in a clinical setting.
If health care workers were to visualize the connection between behavior and outcome or given immediate feedback following an unsafe behavior, then unsafe behaviors that promote faulty mental models would no longer be viewed as harmless.13 Furthermore, short-term training in and of itself may not suffice for long-term behavior change. Educational principles recommend reinforcement and overlearning of behaviors.19 Most large medical/dental facilities, along with credentialing and licensing agencies, recognize the importance of reviewing and updating infection control practices and have requirements in place for ongoing continuing education.20 Future research is needed to determine evidence-based educational strategies for behavioral changes that have positive implications for the reduction of disease transmission for both health care providers and patients.
This study had limitations. Participants were from two courses in one university, and the small sample size reduced the generalizability of the findings. However, the small sample size was free from non-response bias as all students taking the exam were part of the study. Videos for this study were from an off-campus examination location and were recorded outside of the health care setting. Test taking is a stressful activity and unconscious face-touching behavior might be different during such a stressful situation. However, the finding of high frequency of face-touching behavior is of concern, given that the study participants are future health care providers who had completed required infection control educational modules specifically addressing COVID-19 transmission factors. Future studies should take place on the clinic floor in educational settings.
Conclusion
It is general knowledge that the hands may touch objects that may be contaminated and have the potential to transfer pathogens to oneself and to others as well as self-inoculation. The high incidence of face-touching behaviors observed in dental and dental hygiene students in a non-clinical setting may indicate the transfer of pathogens from these behaviors may not be considered consciously. Given the significance of the COVID-19 pandemic and the recommendations for prevention of the spread of disease, avoidance of face-touching has become an important public health message and a behavior for health care providers to model for their patients.
References
1. Rahman J, Mumin J, Fakhruddin B. How frequently do we touch facial T-zone: a systematic review. Ann Glob Health. 2020 Jul 6;86(1):75.
2. CDC. Interim infection prevention and control recommendations for healthcare personnel during the Coronavirus disease 2019 (COVID-19) pandemic; [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; Updated February 23, 2021 [cited 2020 Oct 2]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html
3. WHO. Country and technical guidance-Coronavirus disease [Internet]. Geneva (CH): World Health Organization; 2020 [cited 2020 Oct 2]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance
4. Nicas M, Best D. A study quantifying the hand-to-face contact rate and its potential application to predicting respiratory tract infection. J Occup Environ Hyg. 2008 Jun 5(6):347-52.
5. Kwok YL, Gralton J, McLaws ML. Face-touching behavior: a frequent habit that has implications for hand hygiene. Am J Infect Control. 2015 Feb 43(2):112-4.
6. Wertheim HF, Melles DC, Vos MC, et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis. 2005 Dec 5(12):751-62.
7. Bertsch R. Avoiding upper respiratory tract infections by not touching behavior the face. Arch Intern Med. 2010 May 10;170(9):833-4.
8. Kantor J. Behavioral considerations and impact on personal protective equipment use: Early lessons from the coronavirus (COVID-19) pandemic. J Am Acad Dermatol. 2020 May;82(5):1087-8.
9. Phan LT, Maita D, Mortiz DC, et al.: Personal protective equipment doffing practices of healthcare workers. J Occup Environ Hyg. 2019 Aug;16(8):575-81.
10. Hatta T, Dimond SJ. Differences in face-touching behavior by Japanese and British people. Neuropsychologia. 1984 Jan 1;22(4):531-4.
11. Heaven L, McBrayer D. External motivators of self-touching behavior. Percept Mot Skills. 2000 Feb 1;90(1):338-42.
12. Elder NC, Sawyer W, Palleria H, et al. Hand hygiene and face touching in family medicine offices: A Cincinnati area research and improvement group (CARInG) network study. J Am Board Fam Med. 2014 May-Jun;27(3):339-46.
13. Sax H, Clack L. Mental models: a basic concept for human factors design in infection prevention. J Hosp Infect. 2015 Apr 1;89(4):335-9.
14. Bargh JA, Morsella E. The unconscious mind. Perspect Psychol Sci. 2008 Jan;3(1):73-9.
15. Rozsa L, Apari P. Why infest the loved ones-inherent human behavior indicates former mutualism with head lice. Parasitology. 2012 May 1;139(6):696.
16. Sax H, Allegranzi B, Uckay I, et al. ‘My five moments for hand hygiene': a user-centred design approach to understand, train, monitor and report hand hygiene. J Hosp Infect. 2007 Sep 1;67(1):9-21.
17. Pittet D. Improving compliance with hand hygiene in hospitals. Infect Control Hosp Epidemiol. 2000 Jun;21(6):381-6.
18. Lunn PD, Belton CA, Lavin C, et al. Using behavioral science to help fight the coronavirus. JBPA. 2020 Mar 29;3(1).
19. Bawa P. Retention in online courses: Exploring issues and solutions-a literature review. SAGE Open. 2016 Jan; 6(1):1-11.
20. Wiener RC, Bhandari R, Waters C, et al. Dental and medical CE requirements across the United States: infection control and CPR/BLS. Poster session presented at: Destination: Summit Reaching Impactful Research Heights. 2019 WVCTSI Annual Meeting; 2019 Apr 2-3; White Sulphur Springs, WV.