You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Full-arch restoration can be a clinically challenging treatment modality. Multiple treatment variations exist, and evaluation of patients with limited and/or compromised dentition can result in confusion if the dental practitioner addresses patients' current treatment goals and preferences without also taking into consideration their possible future treatment needs.1 Patients who seek full-arch restorations (ie, edentulous patients) tend to have functional limitations, a lower education level, poorer general health, and a lower socioeconomic status than dentate individuals.2 As a result, these patients typically are concerned about the overall cost as well as the general ease of prosthetic reconstruction.
Before the era of dental implantology, patients requiring dentition replacement were treated with tissue-retained complete dentures, with acceptable results.3,4 Definitive treatment of patients with complete dentures can result in long-term management challenges, including tissue inflammation, bone resorption, limited nutritional intake, psychological impairment, functional challenges, and a generally impaired quality of life compared with dentate patients.5 As the use of titanium dental implants became commonly accepted, those patients who were traditionally treated with complete dentures began seeking implant treatments from an ever- expanding array of restoration options.
Although the rate of edentulism has been declining steadily since the 1970s, full-arch replacement options continue to be in demand.6 Clinicians and patients alike have embraced the use of dental implants to assist in stabilizing maxillary or mandibular dentures and for fixed restorations. However, for a variety of reasons (eg, financial concerns or anxiety about surgical complexity), some patients may choose not to be treated with fixed restorations and may instead opt for treatment with overdentures. Often these patients want to have the option to switch to a fixed restoration at a later time when it would be more feasible for them. The aim of this article is to discuss strategic implant treatment planning that will enable patients to convert to an alternative prosthetic restoration that can be undertaken at a future date.
FACTORS INFLUENCING PATIENT DECISIONS ABOUT FULL-ARCH RESTORATIONS
Several clinical factors influence the choice between fixed and removable implant restorations, such as masticatory performance, bone preservation, maintenance, and cost-effectiveness.7 Personal factors also impact a patient's decision to choose one type of restoration over another or to refuse dental implant treatment, with concerns about overall cost and surgical complexity widely reported to be two critically important factors.8,9 Surgical anxiety and lack of awareness about the treatment or its availability are other primary reasons for patients choosing not to be treated with dental implant restorations.
Lack of Awareness
Although many patients are aware that implant dentistry exists, they still tend to have a general lack of awareness of the role dental implants serve within dental treatment as a whole.10,11 Dental treatment in general can be befuddling for many neophytes to the dental office. Therefore, among those patients who are aware of implant dentistry, many may not fully understand their own treatment options. For example, patients may experience confusion regarding the timing and sequencing of the surgical aspects of implant treatment, with many unaware that dental implant restorations can be expedited or delayed. Some patients may also be confused by television advertisements claiming that dental implants can be pro- vided in a single appointment, whereas for some of the patient's relatives or friends, treatment may have taken considerably long- er to complete. Unfortunately, the dental industry and even clinicians themselves may contribute to this confusion through the marketing and advertising of dental implant procedures, which may promote a particular process as more convenient and simple or less invasive than it may in fact be. Patients' trust in the clini- cian is of paramount importance, and dental clinicians whose practice focuses on full-arch dentistry often need to work tire- lessly at building trust and rapport with patients.
In addition, a disparity often exists between the amount of clinical information that the practitioner discusses with the patient during a consultation and the amount that the patient can recall after leaving the consultation.12 Each implant treatment plan should be highly personalized, and a high degree of clarity should be expressed during consultation sessions. Some clinicians emphasize following up with the patient at a later time, and send him or her out of the consultation appointment with informational pamphlets or patient-centered books on the treatment. Additional consultations with the patient's spouse or partner to increase awareness about dental implant procedures may serve an important role in the planning phases of treatment.
Surgical Anxiety
While routine dental visits are often stressful for many patients, dental surgery can cause much greater anxiety. According to some reports, surgical anxiety is a major reason for refusing implant treatment.13,14 Other patients are anxious about the limited treatment options presented by the clinician. Many patients report a generalized fear of unknown procedures that may stem from the effects of information disseminated by social media and on the internet.
Cost Concerns
Finally, the cost of dental implant procedures can be a surprising and often prohibitive proposition for some patients. Evidence shows that many patients who opt for complete dentures rather than implant treatment are often motivated by cost savings.15,16 Cost is also a major factor for patients in deciding whether to have a standard complete denture, two-implant overdenture, four- to six-implant overdenture, or a fixed hybrid restoration. As implant number and prosthetic complexity increases, the total cost to the patient tends to increase. Yet despite the fact that the cost of dental implants can be, on average, three to six times greater than that of nonimplant replacements, in a study that evaluated long-term outcomes of patients who were treated with dental implants, patients with dental implants were found to be happier overall than those treated with conventional dental prostheses.8 Furthermore, prosthetic stabilization with implants has been shown to be widely effective, with patients reporting that despite the cost of the procedure, they would readily choose implants over nonimplant restorations if they had to do it over again.17 Finally, although patients may be unable to afford a particular treatment initially, they may be willing to have the treatment at a later date or to increase the number of implants over time when finances permit.
IMPLANT OVERDENTURES: PLANNING FOR TODAY AND TOMORROW
The mandibular two-implant overdenture is widely considered the first-choice standard of care for the edentulous or soon-to-be edentulous mandible.18 Factors that are important to consider for effective implant overdenture restoration include implant number, implant position, restorative/prosthetic space underneath the prosthesis, distribution of implants, abutment selection, and prosthesis design.
The two-implant overdenture prosthesis is designed to have resiliency and move slightly while seated on the edentulous ridge. Patients who are older, are looking for surgical simplicity, or are hoping to reduce the costs of treatment may opt for choosing fewer implants rather than more. Number of implants is often reported in the literature as not necessarily being a major factor for long-term patient satisfaction, yet many clinicians empirically feel that a higher number of implants is more likely to result in greater prosthetic stability and patient engagement.
Implant position for overdentures and fixed restorations has been extensively discussed in the literature, with many advocating for six implant location options on the maxillary arch and seven location options on the mandibular arch19 (Figure 1). The implant positions are based upon anatomical factors, bone quality, bone quantity, proximity to critical structures such as nerves and sinuses, and operator comfort and accessibility. When patients present with compromised or resorbed alveolar ridges, sufficient bone quality and quantity typically exists in the anterior mandible between the mental foramina. When a clinician evaluates this interforaminal space, five possible positions exist, labeled A-E, with the A and E positions 5 mm anterior to the mental foramen, the C position in the midline, and the B and D positions halfway between the A-C and C-E positions. While some clinicians may assume that the B and D positions roughly correspond with the mandibular canine positions, they actually are slightly closer to halfway between the mandibular lateral incisor and canine positions. When posterior foramina bone is sufficient for the placement of shorter implants safely above the mandibular nerve, the mandibular first molar may be an optimal position for overdentures as well. On the maxillary arch, the second/first molar, first/second premolar, and lateral incisor positions are considered ideal implant positions. Evidence has emerged that wider distribution and number of implants may lead to a more stable prosthesis.20
Diagnosis and treatment planning rely on a thorough assessment of the patient's remaining dentition, periodontal examination, dental charting, and radiographic analysis. When a patient with a failing dentition presents, formal assessment of the remaining dentition may show a compromised dentition, and the patient may request a full-arch replacement.
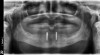
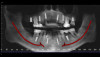
Case Study 1
A 75-year-old man presented with a failing dentition (Figure 2 and Figure 3). Upon evaluation, the patient indicated that he desired a new maxillary complete denture and a mandibular overdenture, and the clinician discussed with him the possible option of two or four implants for his mandibular arch. However, upon further analysis, the patient was found to have extensive periapical lesions in the mandibular left first molar region. Additionally, the patient expressed that, owing to his advanced age, he was concerned about surgical complexity and the cost of reconstruction with four implants, and stated a preference for a simpler and more expedited treatment.
The patient chose the two-implant overdenture option with implants placed at the time of the tooth extractions. The clinician discussed with the patient that additional implant placements could be undertaken at a later date, and the patient was pleased to learn that he had this future option. Teeth were extracted and two 3.4 x 12 implants (Biomet Osseotite®, Zimmer Biomet) were placed in the B and D positions in the interforaminal region of the anter-ior mandible (Figure 4). Implants placed in the indicated regions permit additional implants to be placed distally, in the mandibular first molar or interforaminal A and E positions. After osseointegration, stud-style abutments (LOCATOR R-Tx, Zest Dental Solutions) were placed and a new prosthesis fabricated (Figure 5). The patient was pleased with the final result.
Case Study 2
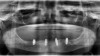
A 45-year-old man presented with a failing dentition (Figure 6). After a comprehensive analysis of his dentition, a cone beam computed tomography scan (Green CT, Vatech America) confirmed that the patient had bone quality and quantity sufficient for several different implant positions (Figure 7). Multiple treatment options were discussed with the patient, including complete dentures, implant overdentures, and fixed hybrid restorations. The patient indicated that he greatly preferred the fixed hybrid restorations, as he was not happy with the idea of removable dentition. After an extensive clinical and financial discussion, the patient concluded that fixed hybrid treatment was beyond his budget and requested implant overdenture treatment. He did inquire about the possibility of changing from the overdenture to the fixed hybrid later if his financial situation changed.
As a result of this discussion, a treatment plan of six implants on the maxillary arch and four implants on the mandibular arch was presented. The patient agreed to the treatment, and the teeth were extracted and dental implants (ET III, Hiossen) were placed in the tooth No. 2/3, 4/5, 7, 10, 13/14, 14/15 positions on the maxillary arch and the tooth No. 19, B, D, 30 positions on the mandibular arch. After osseointegration, definitive stud-style abutments (LOCATOR R-Tx) were placed and torqued according to the manufacturer's recommended torque value on implants in the maxillary and mandibular arches (Figure 8 and Figure 9).
Optical impressions were made using an intraoral scanner (TRIOS® 3, 3Shape). A cobalt-chrome metal framework was designed and produced with 3D printing. The prostheses were processed with conventional acrylic denture teeth (Pala® Mondial®, Kulzer) and acrylic resin. Composite resin (CHAIRSIDE® Attachment Processing Material, Zest Dental Solutions) was injected into the prepared recesses within the denture and the prostheses seated intraorally. After complete polymerization, the prostheses were removed and definitive retention inserts were placed (Figure 10). Overdenture restorations that have more than four abutments and housings tend to have an extremely high degree of prosthetic stability. Because the patient was new to an implant-retained prosthesis, he was started on lower retention-level insert strength (implants at tooth No. 2/3, 7, 10, 14/15 positions), with two of the implants having zero level of retention (implants at tooth No. 4/5, 12/13 positions). After a few recall appointments, he was converted to medium-retention inserts on all implants. The patient was satisfied with the result and, at the time of this writing, wishes to retain the overdenture prosthesis (Figure 11).
Case Discussions
Although the patients in these two case studies did retain their implant overdenture restorations, simply knowing that they could decide to convert from a simple overdenture to an alternative option at a later date enabled them to have enough trust and confidence in the clinician to accept dental implant treatment. For patients who present with a terminal dentition, it is important to openly discuss their treatment goals, comfort level with surgical procedures, and cost/budget concerns early in the diagnostic and treatment planning process. The patient in the first case study had multiple concerns-primarily regarding treatment costs and surgical complexity owing to his advanced age-which were minimized when he learned that he could have additional implants later if he decided that the two-implant prosthesis was insufficient. The patient in the second case study had substantial financial concerns and could not afford the fixed prosthesis, but he was extremely comfortable knowing that if he was not happy with the removable restoration, he could eventually transition to a fixed prosthesis without the need for additional surgical procedures.
As shown in the first case study, older patients tend to gravitate towards simpler surgical procedures and more expedited treatment. Older patients also tend to have increased medical comorbidities that can complicate surgical and prosthetic procedures. Additionally, many are living on fixed incomes, which may make more expensive dental implant treatment prohibitive. By contrast, when a younger patient presents with a failing dentition, clinicians routinely discuss long-term maintenance and the potential for an alternative prosthetic treatment at a future date. Also, younger patients are more inclined to view dental implants as potentially transitional prostheses that may require additional treatment and/or revision at some point in their lifetime.
CONVERTING OVERDENTURES TO FIXED RESTORATIONS
As we discussed, patients who are successfully treated with im-plant overdentures may choose to convert their removable restorations to fixed prostheses at a later date. In such cases, clinicians must face the challenge of deciding on restorative space requirements. Placing implants in strategic positions for implant overdentures with wide distribution and where there is sufficient bone quality and quantity permits the clinician to eventually change prostheses from an overdenture into a fixed prosthesis.
For patients with a successful overdenture prosthesis, the primary motivator for converting their removable restoration to a fixed restoration is typically simply a desire for dentition that is nonremovable. Although the implant overdenture is a generally well-received prosthesis, some patients consider a fixed prosthesis "permanent" and a removable prosthesis as "less permanent." These patients tend to be motivated by personal preference and the perception that a fixed prosthesis has greater advantages than the removable prosthesis.
Implant-retained overdentures derive most of their prosthetic support from the edentulous ridge and the retention from the implant abutment and attachment system. In contrast, because a fixed hybrid implant restoration has only minor tissue contact, it derives all the prosthetic support from the implant and abutment itself. Several delineating factors are important to consider before switching a patient from an overdenture to a fixed restoration. First, implant overdentures require less prosthetic or restorative room within the prosthesis for strength than the fixed hybrid restoration. Locator implant overdentures typically require 9 to 11 mm from the platform of the implant to the outside surface of the prosthesis, whereas fixed hybrid restorations typically require 9 to 15 mm of prosthetic space from the implant platform to the outside surface of the denture. Traditional screw-retained fixed hybrid restorations require a greater amount of restorative space than contemporary fixed hybrid abutment systems. Patients who express an interest in converting to fixed restorations tend to be younger and medically fit to handle additional surgical procedures; such patients typically benefit from having the alveolar ridge prepared to ensure that sufficient restorative space is available later. Older patients who have increased comorbidities tend to opt for less invasive surgical procedures, with the tradeoff being less restorative space with less flexibility available later for future fixed restorations. The clinical tradeoff in the former scenario - ie, that of advocating for extensive alveolar ridge reduction simply for planning for a potential transition to a fixed restoration later - is that excessive alveoloplasty may result in an overdenture with less stability and may not be advantageous to the patient. Both clinical philosophies may be appropriate, and the benefits and risks of each should be weighed equally during the diagnostic and treatment planning phases.
Case Study 3
A 52-year-old woman presented with implants (Legacy 3, Implant Direct) placed in tooth No. 19, B, D, 30 positions and stud-style abutments (LOCATOR R-Tx) that had been functional for approximately 4 years before her consultation appointment (Figure 12). The patient requested to have her removable overdenture prosthesis converted to a fixed hybrid restoration. Because the implants were placed in strategic positions to allow possible future transitioning to fixed restorations with sufficient restorative space, additional surgical procedures would not be necessary for the transition, which the patient was very pleased to learn. Before removing any abutments and proceeding with clinical procedures, the clinician performed radiography to assess the health of the implants (Figure 13). The stud-style abutments were removed using a torque ratchet, and a fixed abutment system (LOCATOR F-Tx, Zest Dental Solutions) was placed with corresponding tissue heights as the previous abutments (Figure 14). The definitive fixed abutments were torqued according to manufacturer's recommended torque values (Figure 15).
Housings were removed from her existing prosthesis using an acrylic bur, and a functionally generated polyvinyl siloxane impression was made inside of the denture, with the patient closing into centric occlusion. The impression and the patient's opposing arch were optically scanned using an intraoral scanner to assist in digital planning. Housings were placed onto the fixed abutments and an intraoral optical scan (TRIOS 3, 3Shape) was performed to capture a detailed impression of the tissue surface (Figure 16).
The optical scans were sent to the laboratory for design of the definitive prosthesis. Using the existing prosthesis as a guide for esthetics, phonetics, incisal edge position, vertical dimension, and centric occlusion, the laboratory technician designed the prosthesis using dental laboratory design software (Dental System 2021, 3Shape) (Figure 17). The prosthesis was milled using a combination of fiber-composite polymer (TRINIA®, Bicon Dental Implants) for the bar, and polymethyl methacrylate (PMMA) was used for the denture base and teeth (Ivotion Denture System, Ivoclar Digital). The bar and the prosthesis were bonded using resin composite (CHAIRSIDE Attachment Processing Material).
The patient returned for definitive placement of the prosthesis. Housings were placed onto each fixed abutment and rotated into position. Composite resin (CHAIRSIDE Attachment Processing Material) was injected into the prepared recesses on the intaglio of the prosthesis and seated onto the edentulous ridge. The patient closed into centric occlusion and held light occlusal forces until the resin was completely polymerized. After polymerization, the prosthesis was removed, and adjustments and polishing procedures were completed. Medium-strength retention inserts were placed into the housings (Figure 18). The prosthesis was seated onto the abutments, and complete adaptation was confirmed to ensure the prosthesis was firmly attached to the abutments, converting it into a fixed prosthesis (Figure 19). The patient was pleased with the final esthetics and the feel of the final prosthesis.
The existing overdenture prosthesis and stud-style abutments were given to her to keep in a safe place in case she should ever wish to convert back to a removable overdenture prosthesis. The patient was seen periodically over the course of 2 years to ensure that she was satisfied with the prosthesis and that she was able to clean underneath the prosthesis. She has reported that she is very satisfied with the fixed prosthesis, and she is comfortable knowing that she can switch back to her existing overdenture if she chooses to do so.
CONCLUSION
Clinicians who are seeking to increase patient acceptance of dental implant procedures, especially those involving full-arch reconstruction, may recognize the challenges posed by patients' lack of awareness about the treatments, surgical anxiety, and concerns about treatment costs and may modify their practices to accommodate them. It is important to keep in mind that, although patients may be highly motivated to reduce the initial expenditures of the restoration, they may also be willing to increase implant number or prosthetic changes over time when finances permit. Ultimately, much of the patient's decision-making process is built upon establishing rapport with the clinician and feeling reassured that the clinician recognizes the patient's particular presentation and/or limitations.
Treating patients with limited dentition and/or edentulous patients with full-arch implant dentistry can be clinically challenging. However, strategic diagnostic protocols, including evaluation of anatomical factors, bone quality, and bone quantity to determine optimal implant location options, can be implemented to ensure that patients who choose treatment with implant overdenture prostheses may, in the future, be able switch to fixed prostheses. By following the protocols outlined in this article, a clinician can plan full-arch restorations with a "future planning" mindset.
About the Author
Michael D. Scherer, DMD, MS
Private Practice, Sonora, California;
Assistant Clinical Professor, School of Dentistry, Loma Linda University, Loma Linda, California
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com
References
1. Pjetursson BE, Heimisdottir K. Dental implants - are they better than natural teeth? Eur J Oral Sci. 2018;126 Suppl 1:81-87.
2. Weintraub JA, Orleans B, Fontana M, Phillips C, Jones JA. Factors associated with becoming edentulous in the US health and retirement study. J Am Geriatr Soc. 2019;67(11):2318-2324.
3. Jacob RF. The traditional therapeutic paradigm: complete denture therapy. J Prosthet Dent. 1998;79(1):6-13.
4. Lang BR. A review of traditional therapies in complete dentures. J Prosthet Dent. 1994;72(5):538-542.
5. Turkyilmaz I, Company AM, McGlumphy EA. Should edentulous patients be constrained to removable complete dentures? The use of dental implants to improve the quality of life for edentulous patients. Gerodontology. 2010;27(1):3-10.
6. Leles CR, Ferreira NP, Vieira AH, Campos AC, Silva ET. Factors influencing edentulous patients' preferences for prosthodontic treatment. J Oral Rehabil. 2011;38(5):333-339.
7. Goodacre C, Goodacre B. Fixed vs removable complete arch implant prostheses: a literature review of prosthodontic outcomes. Eur J Oral Implantol. 2017;10 Suppl 1:13-34.
8. Probst LF, Vanni T, Cavalcante DFB, et al. Cost-effectiveness of implant-supported dental prosthesis compared to conventional dental prosthesis. Rev Saude Publica. 2019;53:s1518-8787.2019053001066.
9. Vogel R, Smith-Palmer J, Valentine W. Evaluating the health economic implications and cost-effectiveness of dental implants: a literature review. Int J Oral Maxillofac Implants. 2013;28(2):343-356.
10. Suprakash B, Ahammed ARY, Thareja A, Kandaswamy R, Nilesh K, Bhondwe Mahajan S. Knowledge and attitude of patients toward dental implants as an option for replacement of missing teeth. J Contemp Dent Pract. 2013;14(1):115-118.
11. Zimmer CM, Zimmer WM, Williams J, Liesener J. Public awareness and acceptance of dental implants. Int J Oral Maxillofac Implants.1992;7(2):228-232.
12. Misra S, Daly B, Dunne S, Millar B, Packer M, Asimakopoulou K. Dentist-patient communication: what do patients and dentists remember following a consultation? Implications for patient compliance. Patient Prefer Adherence. 2013;7:543-549.
13. Sohrabi K, Mushantat A, Esfandiari S, Feine J. How successful are small-diameter implants? A literature review. Clin Oral Implants Res. 2012;23(5):515-525.
14. Walton JN, MacEntee MI. Choosing or refusing oral implants: a prospective study of edentulous volunteers for a clinical trial. Int J Prosthodont. 2005;18(6):483-488.
15. Narby B, Kronström M, Söderfeldt B, Palmqvist S. Changes in attitudes toward desire for implant treatment: a longitudinal study of a middle-aged and older Swedish population. Int J Prosthodont.2008;21(6):481-485.
16. Carlsson GE, Omar R. The future of complete dentures in oral rehabilitation. A critical review. J Oral Rehabil. 2010;37(2):143-156.
17. Rashid F, Awad MA, Thomason JM, et al. The effectiveness of 2-implant overdentures - a pragmatic international multicentre study. J Oral Rehabil. 2011;38(3):176-184.
18. Feine JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Montreal, Quebec, Canada. May 24-25, 2002. Int J Prosthodont. 2002;15:413-414.
19. Kaufmann R, Friedli M, Hug S, Mericske-Stern R. Removable dentures with implant support in strategic positions followed for up to 8 years. Int J Prosthodont. 2009;22(3):233-241; discussion 242.
20. Scherer MD, McGlumphy EA, Seghi RR, Campagni WV. Comparison of retention and stability of implant-retained overdentures based upon implant number and distribution. Int J Oral Maxillofac Implants.2013;28(6):1619-1628.