You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The digital restorative workflow starts with an optical or digital impression, resulting in a virtual or physical model, followed by CAD/CAM technologies to create the restorations. In the case of a single crown, inlay, onlay, or veneer, a master cast no longer is needed since an intraoral impression provides a streamlined transfer. Immediate access to the scan also allows the practitioner to look at preparations and assess occlusal clearance. Digital workflow is generally more efficient, more accurate, and less time consuming than conventional processes.1-6 A digital impression also offers an advantage in dealing with a patient whose gag reflex is triggered by traditional impression-taking materials.7 The two main advantages of digital technology are how it has improved communication and predictability in treatment.2-4
Furthermore, digital impressions allow the clinician to quickly obtain high-resolution records, while eliminating the need for impression-making materials. No longer using trays and impression material not only reduces cost and time for keeping track of inventory but also offers several other advantages that will be discussed below through case examples.
Cases Highlighting the Benefits of Digital Dentistry
High-Resolution Scans Capturing Precise Margins
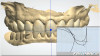
A patient presented to the author with six crowns on maxillary anteriors needing replacements. After the dentist removed the old crowns, cleaned off the preparations, and refined the margins, the patient was ready for the impression. In the digital world, practitioners still follow some of the same protocols as with a traditional impression: isolating the area and retracting the tissues. But then, rather than preparing and applying the impression material, dental professionals take a digital impression and do high-resolution zoom scans of the preparations to capture more of the details (Figure 1).
While analog methods worked well in restorative dentistry for many years, practitioners can do things with digital technology that would be more difficult to accomplish in the physical world. Consider, for example, locking the areas capturing the margins of the preparations in a scan, as shown in Figure 2. This ensures that the retracted soft tissue does not change if the area is rescanned in the impression-making process.
The use of high-definition photography is also possible to assist the laboratory in identifying where the tooth preparation margin stops and where the soft tissue starts.
Once the upper impression has been taken, the practitioner can then scan the opposing arch, and a virtual bite registration is then taken, completing the final impression appointment using a digital workflow.
Predictability in Impression Workflows
Digital technology also fosters more predictable restorations because of the enhanced communication between the dentist and the laboratory, reducing errors and miscommunication, as exemplified in this next case.
A patient presented with a single roundhouse maxillary bridge, splinted together from molar to molar, which displayed deep, bulky margins. The patient was displeased with the esthetics of the bridge and mandibular teeth due to spacing and the difference in color between the mandibular teeth and the maxillary bridge. The upper bridge was removed and the patient was prepared for a full-mouth reconstruction and put into laboratory-made provisional restorations to confirm esthetics, occlusal vertical dimension, occlusion, and functional movements.
Traditional full-arch or full-mouth impressions of preparations on teeth can be difficult, requiring the isolation of tissues. Flowing light body and regular body impression materials risk introducing bubbles on the margins, which would require the impressions to be taken again. With intraoral digital technology, however, the practitioner can capture a pre-preparation scan of provisionals, capturing the esthetics, occlusion, and all surface features. Once the provisionals have been captured, the practitioner can then remove all of them except for two or three, to be used as reference points. The provisionals that were removed can be trimmed away from the scan, and a scan of the preparations is then completed using the remaining provisionals as a common landmark to initial the scan. After scanning, the practitioner can digitally trim away the remaining provisionals, remove them, and scan those remaining preparations. The practitioner is able to work across the arch two or three preparations at a time, removing retraction cords only from teeth about to be scanned.
By capturing high-definition, high-resolution scans of the preparations, locking the surfaces of the margins so they do not change as the scan continues, and moving all around the arch, every preparation is captured accurately and verified in real time. In the author's experience, this is a very predictable and quick procedure, especially in cases where preparations proved to be less than ideal, with overly deep margins. The practitioner was able to capture the bite over the preparations using provisionals on the contralateral side to hold and reference the vertical dimension and relationship record. The resulting scan provided a wealth of information that could be used by the laboratory to create the final layered zirconia restorations. Before and after photographs of this case are shown in Figure 3.
Enhanced Communication With Lab Technicians
Using conventional methods, practitioners sent only a dental model to dental technicians who would layer wax to design the teeth; everything was based on the technician's interpretation of the model, with no reference to the patient's lips, smile, or face. However, the following case exemplifies how digital dentistry can offer more holistic patient information to the laboratory.
The patient presented with missing mandibular posterior teeth, which led to super-eruption of the maxillary posterior teeth and increased forces on the anterior teeth. This resulted in attrition and wear, shortened maxillary and mandibular incisors, and a reverse smile, as the incisal plane did not follow the curvature of the lower lip (Figure 4). The patient did not show incisal edges in his physiological rest position, and lengthening of the incisors was indicated.8
After a digital scan, the practitioner presented smile designs chairside using a smile design application (Figure 5). With the incisal edge position as the starting point, the practitioner modified the design to correct the inverse smile and showed the patient the predicted esthetic result, providing them motivation for treatment during the initial consultation. Additionally, the practitioner provided all of this information to the laboratory. Thus prepared, the dental technicians took the 2D virtual smile design approved by the patient and transferred it into a 3D design at the approved increased vertical dimension, positioned the incisal edges properly, and corrected the overall esthetics and occlusion for the patient.
Following conventional protocols, the dentist still created a direct mockup to verify that all was correct before performing irreversible procedures (Figure 6). Figure 7 shows the chairside provisionals at the new vertical dimension based on the laboratory's design. A digital impression of the chairside provisionals can then be taken, and another round of smile design can be done for further improvements when fabricating the long-term polymethylmethacrylate (PMMA) provisionals. Digital technology allowed the practitioner to give the laboratory very specific instructions. Scans of chairside provisionals were overlaid with laboratory designs, allowing measurement of lengthening and shortening to the exact micrometer; in this case, the incisors were lengthened by 0.6 mm and a premolar was shortened by 0.7 mm from the position of the chairside provisionals (Figure 8). Those precise, fine details made a significant difference in the overall quality of the smile and allowed correction of the reverse plane through enhanced communication with both the patient and the laboratory.
Patient Engagement and Communication
In the next case, the patient presented with a high smile line and with veneers on her central incisors that were too square-shaped, discolored, and chipped (Figure 9). Using conventional methods, the practitioner could do a direct mockup using flowable materials or an indirect mockup based off of a wax-up. Although this technique has been successful, it is time-consuming and lacks a visual tool to facilitate communication between patient and clinician.
Instead, the practitioner followed a digital workflow by taking photographs and completing a simple virtual smile design using a Keynote template (Figure 10). This virtual smile design can all be done in a few minutes or less. Communication with both the patient and the laboratory is detailed, as the dentist can send a screenshot of the post-smile-design image to the laboratory and request a dental technician to base their design from it.
3D printing may be utilized in this digital workflow to fabricate a reduction guide and a gingivectomy guide (Figure 11). This acts as a gingival recontouring guide, and once the veneers are removed, it also acts as a reduction guide, showing the practitioner how much room there is and whether more tooth structure needs reduction. In this case, the patient was happy with the outcome and, most importantly, not surprised because she knew what to expect from the first consultation appointment (Figure 12).
It is important to note that these technologies in no way replace the fundamentals of good dentistry. They are not a shortcut. While it is easy for practitioners to put beautiful-looking teeth on a computer screen, they must not over-promise and under-deliver. The practitioner must employ basic fundamental guidelines of restorative, esthetic, and implant dentistry to ensure he or she can deliver what is shown to the patient.
Predictability and Communication in Occlusal Registration
Another aspect of dentistry where digital technology is having an impact is occlusion. After scanning upper and lower teeth, the scans can be merged for more accurate virtual registration or occlusion using bite scans.1,2 The focus has been on static occlusion-occlusion in one position, whether it is in maximum intercuspal position or centric relation. The new technologies in intraoral scanners allow practitioners to also capture patient-specific dynamic motions and movements in protrusion, and lateral excursive movements. Eventually, this may eliminate the articulator.1,2 Practitioners set up the articulator based on recorded aspects captured from a patient or using average settings, then try to dynamically mimic those motions, knowing that the process has the potential for error. With virtual occlusion, dentists can predictably capture what the patient actually does in his or her own mouth with the most accurate "articulator"-the patient's own jaw. Digital technology in dentistry offers the capability to capture each patient's specific jaw movements, as shown in the following case.
A patient presented after periodontal treatment, with a mandibular incisor that had lost too much bone and required extraction. The incisor was extracted and bonded as a provisional restoration (Figure 13). An implant was contraindicated due to compromised periodontium and limited space; instead, a resin-bonded bridge was planned. Having minimal occlusal forces on the cantilevered pontic would be crucial to the long-term success of the prosthesis.9
The author captured the minimal preparation done on the lingual of the right mandibular lateral incisor and captured the occlusion in the static maximal intercuspal position (MIP). Patient-specific protrusive movements were then captured digitally, and all
information was sent to the laboratory. The laboratory had all the information needed for designing the resin-bonded bridge to fit well and have the cantilevered pontic out of occlusion. Figure 14 shows the lithium disilicate one-wing resin-bonded bridge bonded into place.
Innovation and Efficiency
Digital technology exhibits great potential for innovation and efficiency. It can enable practitioners to think outside the box, as demonstrated in this next case.
A patient presented to the practice with worn-down and discolored teeth, several of which had received root canals; various worn and discolored restorations; and a slight reduction in vertical dimension (Figure 15). A full-mouth reconstruction was indicated. The author met with the patient for an initial consultation and performed diagnostics, assessed incisal display, and performed a chairside smile design (Figure 16). The patient expressed heightened expectations and was excited and motivated after seeing a digital representation of the projected result.
Information was sent to the laboratory, which took the 2D smile design and transferred it to a 3D digital wax-up, allowing the author to assess not only what the final restoration would look like, but how much tooth reduction was needed. In Figure 17 and Figure 18, the purple represents the patient's existing teeth; the virtual wax-up is outlined in white, showing that not much incisal reduction was indicated on the two centrals, but that the right canine required more reduction to tuck it in. Again, the virtual wax-up facilitated an understanding of where selective, conservative reduction was needed and offered predictability in achieving results.
Once the virtual wax-ups were completed and approved, 3D printing came next, and innovation and thinking outside the box were possible. Preparing an arch or full mouth in a conventional manner requires a long appointment, and once all the teeth are prepared, references are lost, so the practitioner may not capture the correct vertical dimension or may introduce a cant to the occlusal or incisal plane.
The author took the virtual wax-up and created 3D-printed PMMA temporary shells of minimal thickness with palatal supports to allow seating (Figure 19). The goal was to prepare all of the teeth and use the palate as a reference point to seat the temporary shells and reline them in the mouth at the correct vertical dimension and orientation. The key to getting the shells to seat was to make sure preparation was precisely based on the virtual wax-up, which was why a 3D-printed reduction guide was also fabricated (Figure 20). After the teeth were prepared, the practitioner could seat the reduction guide, see where teeth were under-reduced, and reduce more to assure the temporaries would fit over the preparation. The temporary shell could then be relined, using palatal support as a reference for placement (Figure 21), the extensions were sectioned away to remove palatal support, and the multi-unit provisional was sectioned two or three units at a time. The practitioner could therefore predictably prepare and provisionalize an entire mouth while maintaining the correct planned vertical dimension and occlusal relationship. This allows for more efficiency and less appointments while maintaining predictability and good outcomes (Figure 22).
Conclusion
Philosophically, change need never be painful; only the resistance to change is painful. It is the responsibility of dental practitioners to update their procedures to provide patients with better quality care. Digital technology in dentistry enables patients to benefit from improved predictability and enhanced communication.
About the Authors
Faraj Edher, DDS, MSc, Dip. Pros., FRCD(C)
Prosthodontist, private practice
Clinical Assistant Professor, University of British Columbia
Director, Digital Dentistry Institute
Vancouver, British Columbia, Canada
Ariana Aram, DMD
candidate Harvard School of Dental Medicine
Boston, Massachusetts, USA
References
1. Edher F, Hannam AG, Tobias DL, Wyatt CCL. The accuracy of virtual interocclusal registration during intraoral scanning. J Prosthet Dent. 2018;120(6):904-912.
2. Abdulateef S, Edher F, Hannam AG, Tobias DL, Wyatt CCL Clinical accuracy and reproducibility of virtual interocclusal records. J Prosthet Dent. 2020;S0022-3913(10)30751-30756.
3. Cervino G, Fiorillo L, Arzukanyan AV, Spagnuolo G, Cicciù M. Dental Restorative digital workflow: digital smile design from aesthetic to function. Dent J (Basel). 2019;7(2):30.
4. Dawood A, Marti Marti B, Sauret-Jackson V, Darwood A. 3D printing in dentistry. Br Dent J. 2015;219(11):521-529.
5. Aragon MLC, Pontes LF, Bichara LM, Flores-Mir C, Normando D. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: a systematic review. Eur J Orthod. 2016;38:429-434.
6. Patzelt SB, Emmanouilidi A, Stampf S, Strub JR, Att W. Accuracy of full-arch scans using intraoral scanners. Clin Oral Investig. 2014;18:1687-1694.
7. Londono J, Abreu A, Baker PS, Furness AR. Fabrication of a definitive obturator from a 3D cast with a chairside digital scanner for a patient with severe gag reflex: a clinical report. J Prosthet Dent. 2015;114(5):735-738.
8. Bhuvaneswaran M. Principles of smile design. J Conserv Dent. 2010;13(4):225-232.
9. Sharma A, Rahul GR, Poduval ST, Shetty K. Assessment of various factors for feasibility of fixed cantilever bridge: a review study. ISRN Dent. 2012;2012:259891.